Pediatric Ankle & Foot Fractures: Understanding Short Leg Walking
Key Takeaway
Here are the crucial details you must know about Pediatric Ankle & Foot Fractures: Understanding Short Leg Walking. Pediatric ankle injuries often involve growth plates (physes), which are weaker than ligaments in children. Frequently sustained during sports, these injuries cause pain, swelling, and difficulty walking. Timely diagnosis and proper treatment are crucial to prevent complications like altered bone growth or limb length discrepancies, potentially leading to short leg walking. A thorough neurovascular assessment is vital.
Comprehensive Introduction and Patho-Epidemiology
Pediatric ankle and foot fractures represent a complex intersection of skeletal immaturity, dynamic biomechanical forces, and unique anatomical vulnerabilities. Ankle injuries are remarkably prevalent in the pediatric population, accounting for up to 18% of all physeal injuries. In the hierarchy of epiphyseal trauma, they rank third in overall frequency, superseded only by phalangeal and distal radius physeal injuries. The vast majority of these injuries—approximately 58%—are sustained during athletic participation, underscoring the high-energy, torsional forces subjected to the skeletally immature lower extremity. Furthermore, ankle fractures represent a significant 10% to 40% of all orthopedic injuries in skeletally immature athletes, mandating a thorough understanding of their patho-epidemiology by the treating orthopedic surgeon.
The epidemiology of these fractures is heavily dictated by the chronological and biological age of the patient, which directly correlates with the developmental state of the distal tibial and fibular physes. Tibial physeal fractures demonstrate a peak incidence between 8 and 15 years of age, whereas fibular physeal injuries most commonly present between 8 and 14 years of age. A fundamental tenet of pediatric orthopedic traumatology is that ligamentous injuries (sprains) are exceptionally rare in young children. This is due to the inherent biomechanical mismatch between the robust, highly elastic ligamentous complexes and the relatively weak cartilaginous physis—specifically the zone of provisional calcification and the zone of hypertrophy. When a deforming force is applied to the pediatric ankle, failure almost invariably occurs through the physis rather than the ligamentous restraints.

As the pediatric patient approaches skeletal maturity, typically after the age of 15 to 16 years, the biomechanical paradigm shifts. The physes begin their predictable sequence of closure, fortifying the bone and rendering the ligamentous structures the weakest link in the kinetic chain. Consequently, older adolescents begin to exhibit adult-type fracture patterns, such as classic Weber B or C fibular fractures, or isolated ligamentous ruptures. Understanding this epidemiological transition is paramount for accurate clinical suspicion, appropriate radiographic evaluation, and the formulation of an optimal treatment algorithm that mitigates the risk of long-term sequelae, such as premature physeal closure and angular deformity.
Detailed Surgical Anatomy and Biomechanics
Osteology and Physeal Development
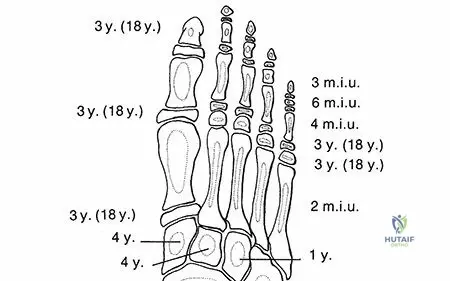
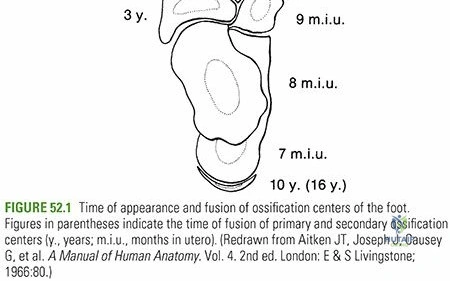
The pediatric ankle is a highly modified hinge joint, inherently reliant on the precise articulation between the talar dome and the complex mortise formed by the distal tibia and fibula. The distal tibial ossific nucleus typically appears between the ages of 6 and 24 months, gradually expanding to form the articular plafond. It ultimately fuses with the tibial shaft at approximately 15 years of age in females and 17 years of age in males. The distal fibular ossific nucleus appears slightly later, between 9 and 24 months of age, and unites with the fibular shaft 12 to 24 months after the complete closure of the distal tibial physis.
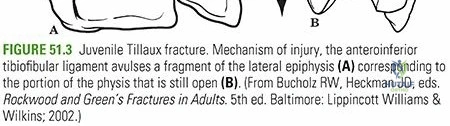
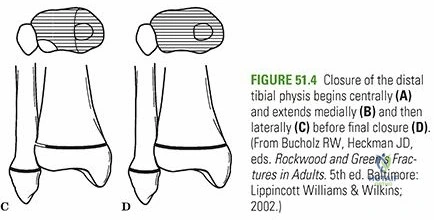
The most critical anatomical concept governing pediatric ankle trauma is the asymmetrical closure pattern of the distal tibial physis. Over an 18-month transitional period during early adolescence, the physis fuses in a highly predictable, sequential manner: beginning centrally, progressing to the anteromedial quadrant, then to the posteromedial quadrant, and finally closing laterally. This unique biological phenomenon creates a window of vulnerability where the lateral aspect of the distal tibial physis remains open and structurally weaker than the fused medial aspect. This precise anatomical quirk is the direct pathoanatomical genesis of the unique transitional fracture patterns, namely the Juvenile Tillaux and Triplane fractures.
Ligamentous Anatomy and Secondary Ossification Centers
The stability of the ankle mortise is maintained by the medial (deltoid) and lateral (anterior talofibular, calcaneofibular, and posterior talofibular) ligamentous complexes, alongside the robust syndesmotic ligaments. Crucially, in the pediatric patient, all major ligaments attach distal to the physes of the tibia and fibula. This distal attachment is the primary reason why avulsion forces translate directly into transphyseal shear or tension stress, resulting in the classic Salter-Harris fracture patterns rather than ligamentous ruptures. The anterior inferior tibiofibular ligament (AITFL), in particular, plays a starring role in the Juvenile Tillaux fracture, acting as the tether that avulses the unfused anterolateral tibial epiphysis when an external rotation force is applied.

Surgeons must also be acutely aware of secondary ossification centers, which can easily be misdiagnosed as acute avulsion fractures of the medial or lateral malleoli. An os subtibiale is present adjacent to the medial malleolus in approximately 20% of patients, while an os subfibulare is seen near the lateral malleolus in about 1% of patients. These accessory ossicles are frequently bilateral and characteristically feature smooth, well-corticated borders, distinguishing them from the jagged, irregular radiolucent lines of an acute fracture. However, localized point tenderness over these ossicles following acute trauma may indicate a symptomatic disruption of the synchondrosis, necessitating immobilization despite the absence of a true fracture.
Talar Anatomy and Vascularity
While pediatric foot fractures are exceedingly rare—talar fractures account for a mere 0.01% to 0.08% of all pediatric fractures—their anatomical complexity demands rigorous attention. The ossification center of the talus appears early, at approximately 8 months in utero. Uniquely, two-thirds of the talus is covered with articular cartilage, severely limiting the surface area available for vascular penetration. The body of the talus is covered superiorly by the trochlear articular surface, which is wider anteriorly than posteriorly, locking into the mortise during dorsiflexion to confer intrinsic osseous stability to the ankle.
The arterial supply to the talus is notoriously tenuous, rendering it highly susceptible to avascular necrosis (AVN) following displaced fractures, particularly those of the talar neck. The blood supply is derived from two main sources. The artery of the tarsal canal arises from the posterior tibial artery approximately 1 cm proximal to the bifurcation of the medial and lateral plantar arteries, giving off a vital deltoid branch that supplies the medial body. The artery of the sinus tarsi, formed by anastomoses from the perforating peroneal and dorsalis pedis arteries, supplies the lateral and inferior aspects. Disruption of these delicate anastomotic networks during high-energy trauma dictates the high morbidity associated with pediatric talus fractures.
Exhaustive Indications and Contraindications
The decision-making process for the management of pediatric ankle and foot fractures hinges on achieving an anatomic reduction of the articular surface, restoring the alignment of the physis to prevent growth arrest, and providing stable fixation to allow for early mobilization, such as short leg walking. The indications for operative versus non-operative management are strictly defined by the fracture pattern, the degree of displacement, and the remaining growth potential of the patient.
Non-operative management, typically consisting of closed reduction and immobilization in a well-molded cast, is indicated for the vast majority of Salter-Harris Type I and Type II fractures of both the distal tibia and fibula. In children under 10 years of age with significant remaining growth potential, minor residual angulation in the sagittal or coronal plane may be acceptable due to the robust remodeling capacity of the distal tibial physis. However, rotational deformities will not remodel and must be anatomically corrected. Contraindications to non-operative management include an inability to achieve or maintain an acceptable reduction, often due to the interposition of soft tissues such as the periosteum or neurovascular structures.
Operative intervention is unequivocally indicated for any intra-articular fracture (Salter-Harris Type III and IV, Tillaux, and Triplane fractures) demonstrating greater than 2 mm of articular step-off or gap. Left unreduced, these incongruities dramatically alter the contact biomechanics of the tibiotalar joint, leading to focal cartilage overload and early-onset post-traumatic osteoarthritis. Furthermore, operative exploration is indicated in Salter-Harris Type I or II fractures that are irreducible by closed means. The classic scenario involves a medial malleolar Salter-Harris Type II fracture where a flap of torn periosteum becomes incarcerated within the physeal gap, physically blocking reduction.
| Fracture Type | Non-Operative Indications | Operative Indications (ORIF / CRPP) | Absolute Contraindications to Immediate Surgery |
|---|---|---|---|
| Lateral Malleolus (SH I/II) | Nondisplaced or reducible; stable post-reduction. | Open fractures; irreducible fractures; vascular compromise. | Severe fracture blisters (hemorrhagic); active local infection. |
| Medial Malleolus (SH III/IV) | Truly nondisplaced (<2 mm gap/step-off); closely monitored. | >2 mm articular displacement; interposed periosteum blocking reduction. | Medically unstable polytrauma patient (requires damage control external fixation). |
| Juvenile Tillaux | <2 mm vertical step-off; <3 mm horizontal gap. | >2 mm vertical or >3-5 mm horizontal displacement; rotational instability. | Severe soft tissue compromise precluding safe anterolateral approach. |
| Triplane Fracture | Nondisplaced or reducible to <2 mm articular step-off. | >2 mm intra-articular displacement; failure of closed reduction. | Inadequate advanced imaging (CT) leading to poor preoperative planning. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical and Radiographic Evaluation
A meticulous clinical evaluation is the cornerstone of preoperative planning. Patients with displaced ankle fractures present with acute pain, gross deformity, and an absolute inability to bear weight. A rigorous neurovascular examination is mandatory, documenting the presence and quality of dorsalis pedis and posterior tibial pulses, capillary refill, and specific sensory and motor function of the deep peroneal, superficial peroneal, tibial, and sural nerves. Soft tissue assessment is critical; any dressings or splints placed in the field must be removed to evaluate for open wounds, tenting of the skin, or the presence of fracture blisters, which may necessitate delaying definitive surgical fixation or altering the surgical approach.
Standard radiographic evaluation includes high-quality anteroposterior (AP), lateral, and mortise views of the ankle. The treating surgeon must maintain a high index of suspicion for concomitant injuries; tenderness over the proximal fibula mandates full-length tibia/fibula orthogonal radiographs to rule out a Maisonneuve-equivalent injury. Stress views, particularly gravity or manual external rotation stress radiographs, may be utilized to unmask occult instability or undisplaced transphyseal fractures, though these are often difficult to obtain in the acute setting due to patient guarding and pain.
For complex transitional fractures—specifically Juvenile Tillaux and Triplane fractures—Computed Tomography (CT) is the gold standard and is considered mandatory for preoperative planning. CT with multiplanar reconstructions (sagittal, coronal, and axial) and 3D rendering allows the surgeon to precisely map the fracture geometry, quantify the degree of articular displacement, and identify the exact location of the metaphyseal spike in triplane injuries. Magnetic Resonance Imaging (MRI) is less commonly used in the acute fracture setting but is invaluable for delineating associated osteochondral lesions of the talus, occult ligamentous avulsions, or assessing the viability of the talar dome in cases of severe trauma.
Patient Positioning and Operating Room Setup
Proper patient positioning is essential for facilitating both the surgical approach and intraoperative fluoroscopy. The patient is typically positioned supine on a radiolucent operating table. A bump is placed under the ipsilateral hip to internally rotate the leg, bringing the foot and ankle into a neutral, forward-facing position, which is particularly helpful for visualizing the lateral malleolus and the anterolateral distal tibia. A non-sterile tourniquet is applied to the proximal thigh to provide a bloodless surgical field.
The fluoroscopy unit (C-arm) should be positioned on the contralateral side of the table, allowing the monitor to be placed in the surgeon's direct line of sight. The surgeon must ensure that perfect AP, lateral, and mortise views can be obtained without obstruction before the patient is draped. Preoperative templating using the CT scan is crucial for determining screw trajectory. In younger patients with significant remaining growth, the surgeon must template the use of smooth Kirschner wires or plan screw trajectories that remain strictly within the epiphysis or metaphysis, avoiding transphyseal compression. In older adolescents with transitional fractures, the physis is already closing, allowing for the safe use of transphyseal lag screws to achieve absolute stability.
Step-by-Step Surgical Approach and Fixation Technique
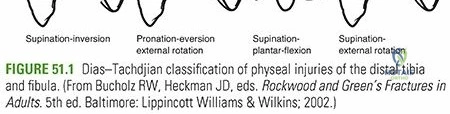
The Dias-Tachdjian Classification and Closed Reduction Maneuvers
Surgical intervention and closed reduction maneuvers are heavily guided by the Dias-Tachdjian classification, which adapts the adult Lauge-Hansen principles to the pediatric skeleton, incorporating the Salter-Harris classification. This typology simplifies complex injury vectors by noting the direction of physeal displacement, the Salter-Harris type, and the location of the metaphyseal fragment.
Supination-External Rotation (SER): This pattern typically results in a Salter-Harris Type II fracture of the distal tibia combined with a Stage II spiral fracture of the fibula. Reduction involves internal rotation and pronation of the foot while applying direct pressure over the displaced metaphyseal fragment.
Pronation-Eversion-External Rotation (PEER): Comprising 15% to 20% of pediatric ankle fractures, this mechanism produces a marked valgus deformity. It typically involves a Salter-Harris Type II tibial fracture with a laterally based metaphyseal fragment, accompanied by a short oblique fibular fracture 4 to 7 cm proximal to the tip. Reduction requires internal rotation and supination.
Supination-Plantar Flexion (SPF): This results in a Salter-Harris Type II tibial fracture with a posterior metaphyseal fragment. Fibular fractures are rare. Reduction is achieved by dorsiflexion and anterior translation of the foot.
Supination-Inversion (SI): The most common mechanism, often presenting as a Salter-Harris Type I or II of the distal fibula. If force continues, it progresses to a Stage II Salter-Harris III/IV of the medial tibia. This pattern carries the highest incidence of complications, particularly premature physeal arrest leading to varus deformity.
Operative Fixation of Medial and Lateral Malleolar Fractures
For Salter-Harris Type III and IV fractures of the medial malleolus with >2 mm of displacement, anatomic reduction is non-negotiable. An anteromedial approach is utilized. The incision is made carefully to avoid the saphenous vein and nerve. The fracture site is exposed, and the joint is inspected. Frequently, a flap of torn periosteum is found inverted into the fracture site; this must be meticulously extracted using a dental pick or freer elevator to allow for anatomic reduction. Once reduced, the fracture is provisionally held with smooth K-wires. Definitive fixation is achieved using partially threaded cancellous screws (typically 3.5 mm or 4.0 mm) placed parallel to the physis, either entirely within the epiphysis or entirely within the metaphysis, to avoid tethering the growth plate.
Lateral malleolar fractures (Salter-Harris III/IV) requiring open reduction are approached via a direct lateral incision. Care is taken to protect the superficial peroneal nerve proximally and the sural nerve distally. If periosteum is interposed, it is removed, and the fracture is reduced. Fixation often involves smooth intramedullary Kirschner wires driven perpendicular to the physis, or epiphyseal lag screws if the fragment is of sufficient size.
Fixation of Transitional Fractures (Tillaux and Triplane)
Juvenile Tillaux fractures (Salter-Harris Type III of the anterolateral epiphysis) occur when the central and medial physes are closed, but the lateral physis remains open. Closed reduction is attempted via internal rotation and direct anterolateral pressure. If displacement remains >2 mm, an anterolateral approach is employed. The superficial peroneal nerve is protected. The fracture is cleared of hematoma, reduced anatomically under direct vision of the articular surface, and fixed with one or two 3.5 mm or 4.0 mm cannulated cancellous lag screws directed from lateral to medial, parallel to the joint surface.


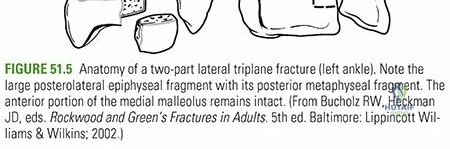
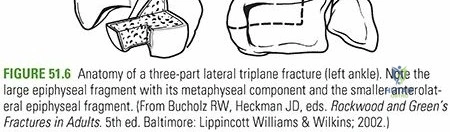
Triplane fractures are complex injuries occurring in three planes: transverse (through the physis), coronal (through the posterior metaphysis), and sagittal (through the epiphysis). They can present as two-part, three-part, or even four-part fractures. The peak incidence is 13 to 15 years in males and 12 to 14 years in females. If closed reduction fails to achieve <2 mm articular step-off, operative fixation is required. The surgical strategy depends on the fragment geometry identified on CT. Often, the epiphyseal (Tillaux-like) fragment is reduced first and provisionally pinned. Then, the metaphyseal fragment is reduced. Fixation is typically achieved with a combination of AP screws for the coronal metaphyseal fracture and lateral-to-medial epiphyseal screws for the sagittal epiphyseal fracture. Because the physis is actively closing in these patients, transphyseal hardware is generally well-tolerated and carries a low risk of clinically significant growth arrest.


Complications, Incidence Rates, and Salvage Management
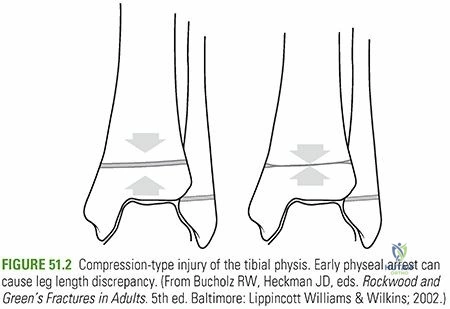
The management of pediatric ankle fractures is fraught with potential complications, primarily stemming from the disruption of the delicate physeal architecture. The most dreaded complication is premature physeal arrest, which can lead to progressive angular deformity and leg length discrepancy. The incidence of complications is directly correlated with the energy of the injury, the Salter-Harris classification, and the adequacy of the initial reduction.
Angular deformity occurs when a localized osseous bridge (physeal bar) forms across the growth plate, tethering growth asymmetrically. This is most commonly seen following high-energy Salter-Harris Type III and IV injuries, particularly the Supination-Inversion mechanism. A varus deformity is the classic sequela of a medial tibial physeal arrest, while a valgus deformity typically results from a distal fibular physeal arrest or a lateral tibial arrest. The development of Harris growth lines (radiodense lines parallel to the physis) seen on radiographs 6 to 12 weeks post-injury serves as a critical biological marker; if these lines remain parallel to the physis, uniform growth is occurring. If they converge toward the physis, a localized arrest is imminent.
Leg length discrepancy (LLD) complicates up to 10% to 30% of pediatric ankle fractures, depending heavily on the age of the patient at the time of injury. For discrepancies projected to be between 2 to 5 cm at skeletal maturity, a contralateral distal tibial and fibular epiphysiodesis is the treatment of choice. For larger discrepancies or in patients who present near skeletal maturity with an established deformity, complex salvage procedures such as supramalleolar corrective osteotomies or distraction osteogenesis using circular external fixators (Ilizarov or Taylor Spatial Frame) may be required.
| Complication | Estimated Incidence | Pathophysiology & Risk Factors | Salvage Management & Treatment |
|---|---|---|---|
Clinical & Radiographic Imaging Archive