Pediatric Forearm Fractures: Your Guide to Long Arm Casts
Key Takeaway
Learn more about Pediatric Forearm Fractures: Your Guide to Long Arm Casts and how to manage it. Pediatric forearm fractures represent 40% of all childhood fractures, frequently affecting children over five years old during rapid growth periods. These injuries often occur in the distal metaphyses of the radius or ulna, areas of active bone growth. Effective management typically involves immobilization, with a long arm cast often used to stabilize the arm from above the elbow to the wrist for optimal healing.
Introduction and Epidemiology
Pediatric forearm fractures represent a significant portion of the trauma burden managed by orthopedic surgeons, necessitating a profound understanding of both non-operative and operative management strategies. These injuries are exceedingly common, constituting approximately 40% of all pediatric fractures. Despite this high prevalence, only 4% of these injuries are true diaphyseal fractures, with the vast majority occurring in the metaphyseal regions. There is a well-documented 3:1 male predominance, particularly in distal radius fractures.
The demographic distribution reveals that 80% of these fractures occur in children over the age of 5 years. The peak incidence directly corresponds to the peak velocity of skeletal growth. During this rapid growth phase, the bone is transiently weaker due to a physiological dissociation between bone growth (matrix formation) and subsequent mineralization, creating a window of vulnerability to mechanical failure under axial and bending loads.
Associated injuries must be actively excluded during the initial trauma evaluation. Approximately 15% of pediatric forearm fractures present with an ipsilateral supracondylar humerus fracture, creating a "floating elbow" scenario that drastically alters management algorithms and increases the risk of compartment syndrome. Neurologic injury is present in approximately 1% of cases, with the median nerve being the most commonly compromised, particularly in severely displaced distal third fractures or those with significant volar angulation.

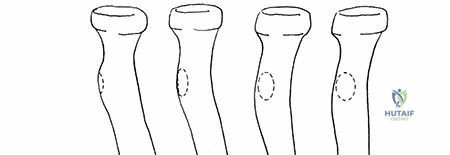
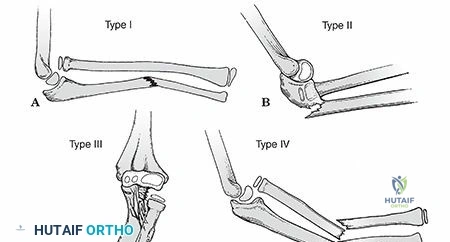
Topographically, 60% of pediatric forearm fractures occur in the distal metaphyses of the radius or ulna, 20% in the diaphyseal shaft, 14% involve the distal physis, and fewer than 4% occur in the proximal third. Understanding this epidemiological distribution is critical for anticipating fracture patterns and preparing appropriate reduction maneuvers and immobilization strategies.
Surgical Anatomy and Biomechanics
Ossification and Osteology
The embryological development and subsequent ossification of the forearm dictate its biomechanical properties throughout childhood. The radial and ulnar shafts begin to ossify early, during the eighth week of gestation. Postnatally, the distal radial epiphysis appears at age 1 year, frequently arising from two distinct ossification centers. The distal ulnar epiphysis appears later, at age 5 years. Proximally, the radial head ossifies between ages 5 and 7 years, while the olecranon apophysis appears between ages 9 and 10 years. Complete physeal closure for all these centers typically occurs between the ages of 16 and 18 years.

The distal physes are the primary engines of longitudinal growth for the forearm, accounting for 80% of its total length. As skeletal age advances, there is a documented tendency for fractures to occur in an increasingly distal location. This phenomenon is attributed to the distal recession of the transitional zone between the wider, more vulnerable, and less dense metaphysis and the narrower, thicker-corticed, and stronger diaphysis.
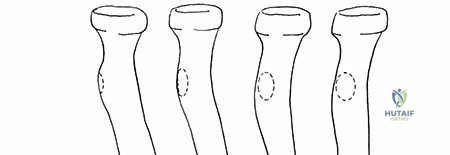
The osteology of the forearm is complex and integral to its function. The radius is a dynamically curved bone; it is cylindric in its proximal third, transitions to a triangular cross-section in the middle third, and flattens distally. Crucially, it possesses an apex lateral bow that must be maintained or restored to preserve pronosupination. The ulna maintains a triangular shape throughout its length and features an apex posterior bow in its proximal third.

Joint Stability and Ligamentous Anatomy
The proximal radioulnar joint is most stable in supination. In this position, the broadest articular surface of the radial head optimally contacts the radial notch of the ulna, and the interosseous membrane achieves maximum tension. The annular ligament serves as the primary soft tissue stabilizer of this joint.
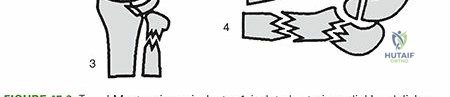
Distally, the distal radioulnar joint is stabilized by a complex network including the ulnar collateral ligament, the anterior and posterior radioulnar ligaments, and the dynamic stabilizing force of the pronator quadratus muscle. Approximately 3% of distal radius fractures feature concomitant distal radioulnar joint disruption, which must be identified to prevent chronic instability.
The triangular fibrocartilage complex is a critical structure comprising an articular disc joined by volar and dorsal radiocarpal ligaments, as well as fibers from the ulnar collateral ligament. It originates at the ulnar margin of the distal radius and its apex inserts at the base of the ulnar styloid, extending distally to the base of the fifth metacarpal.
A defining characteristic of pediatric bone is the thick, highly osteogenic periosteum. During a fracture, the periosteum is generally disrupted on the convex side of the deformity, whereas an intact, robust periosteal hinge remains on the concave side. This intact hinge is the most critical anatomical consideration when attempting closed reduction, as it provides a tension band against which the fracture can be reduced and stabilized.
Biomechanical Principles and Deforming Forces
Forearm kinematics rely on the complex interplay between the radius, ulna, and their ligamentous constraints. The posterior distal radioulnar ligament is taut in pronation, whereas the anterior ligament becomes taut in supination. Functionally, the radius effectively shortens with pronation and lengthens with supination.
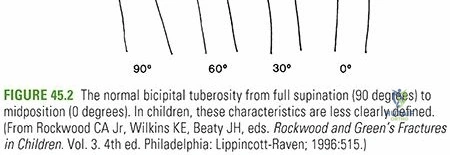
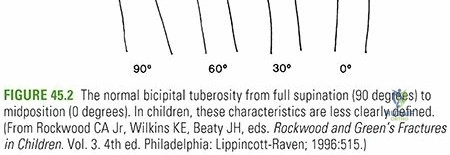
The interosseous space, which must be preserved to allow the radius to rotate around the ulna, is narrowest in full pronation and widest in neutral to 30 degrees of supination. Extreme supination or pronation relaxes the interosseous membrane. The average physiological range of pronation and supination is 90 degrees in each direction, though only 50 degrees of pronation and 50 degrees of supination are strictly necessary for most activities of daily living.

Deformity location dictates functional loss. Middle third deformities have a profoundly greater negative effect on supination, whereas distal third deformities predominantly restrict pronation. A malreduction of just 10 degrees in the middle third of the forearm can limit rotational arc by 20 to 30 degrees. Interestingly, pure bayonet apposition (overlapping) of the radius and ulna, provided the interosseous space is maintained and angular deformity is corrected, does not significantly reduce forearm rotation in the pediatric patient due to remodeling potential.
Understanding deforming muscle forces is paramount for successful reduction and casting.
Proximal third fractures are heavily influenced by the biceps and supinator. These muscles function to flex and supinate the proximal fragment. Consequently, the proximal fragment assumes a flexed and supinated posture, necessitating the distal fragment to be brought into supination during reduction to align with the proximal segment.
In middle third fractures, the pronator teres inserts on the proximal fragment, counteracting the supinator and biceps, leaving the proximal fragment in a neutral rotation. The distal fragment is pronated by the pronator quadratus. Therefore, midshaft fractures are typically immobilized in neutral rotation.
For distal third fractures, both the pronator teres and supinator exert their forces on the proximal fragment, maintaining it in neutral. The distal fragment remains subject to the pronating force of the pronator quadratus and the deforming pull of the brachioradialis, often requiring reduction and immobilization in pronation to achieve anatomic alignment.
Indications and Contraindications
The management of pediatric forearm fractures is heavily dictated by the patient's age, remodeling potential, and the specific characteristics of the fracture. The primary goal is the restoration of functional pronosupination, which relies on restoring the radial bow and maintaining the interosseous space.
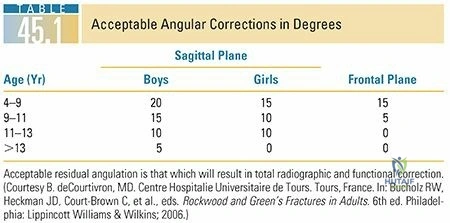
Acceptable Alignment Criteria
Remodeling potential is robust in children under the age of 8 to 10 years, particularly in the plane of joint motion (sagittal plane) and closer to the rapidly growing distal physis.
For children under 8 years of age:
* Up to 15-20 degrees of angulation is acceptable.
* Up to 45 degrees of malrotation can be tolerated.
* Complete displacement with bayonet apposition is acceptable provided angular and rotational parameters are met, and the interosseous space is preserved.
For children over 8 years of age (approaching skeletal maturity):
* Maximum of 10 degrees of angulation is acceptable.
* Maximum of 30 degrees of malrotation is tolerated.
* Bayonet apposition is generally not acceptable due to diminished remodeling potential and high risk of functional deficit.
| Management Strategy | Primary Indications | Relative Contraindications |
|---|---|---|
| Closed Reduction and Long Arm Cast | Acceptable alignment achievable; Age < 10 years; Intact periosteal hinge; Isolated forearm fracture | Open fractures; Polytrauma; Floating elbow; Unacceptable alignment post-reduction; Compartment syndrome |
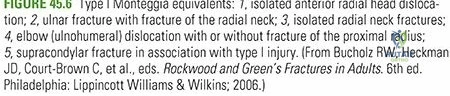
| Elastic Stable Intramedullary Nailing | Failure of closed reduction; Age > 10 years with displacement; Unstable patterns (e.g., Monteggia variants); Re-fractures | Active medullary infection; Extremely distal or proximal metaphyseal fractures (relative) |
| Open Reduction Internal Fixation | Irreducible fractures (soft tissue interposition); Approaching skeletal maturity; Non-unions; Pathologic fractures | Severe soft tissue compromise over proposed surgical incisions |
Pre Operative Planning and Patient Positioning
Closed Reduction Preparation
Meticulous pre-operative planning is required even for non-operative management. The surgeon must review orthogonal radiographs to determine the apex of the deformity, the suspected location of the intact periosteal hinge, and the rotational profile of the fracture fragments.
Adequate analgesia and muscle relaxation are non-negotiable for a successful closed reduction. This can be achieved via conscious sedation in the emergency department, regional anesthesia (such as a hematoma block or supraclavicular block), or general anesthesia in the operating room.

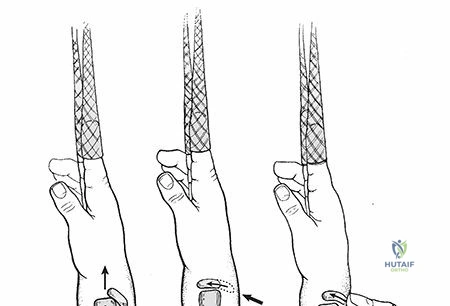
The patient is positioned supine. Finger traps are highly recommended to provide sustained, counter-weighted longitudinal traction. Typically, 5 to 10 pounds of weight are suspended from the distal humerus with the elbow flexed to 90 degrees. This traction overcomes muscle spasm, disimpacts the fracture fragments, and utilizes ligamentotaxis to assist in preliminary alignment.
Operative Intervention Preparation
If operative intervention (such as Elastic Stable Intramedullary Nailing) is anticipated, pre-operative planning includes measuring the narrowest diameter of the medullary canal on the AP and lateral radiographs to select the appropriate nail diameter. The nail diameter should be approximately 40% of the narrowest canal diameter to ensure adequate canal fill and three-point fixation without causing iatrogenic comminution.
The patient is positioned supine on a radiolucent hand table. The C-arm fluoroscopy unit is positioned parallel to the table, coming in from the head or the foot, allowing for unhindered orthogonal imaging of the entire forearm without moving the fracture site. A sterile tourniquet is applied to the proximal arm.
Detailed Surgical Approach and Technique
Principles of Closed Reduction
The cornerstone of pediatric forearm fracture management is the closed reduction and application of a well-molded long arm cast. The reduction maneuver must be deliberate and respect the soft tissue envelope.
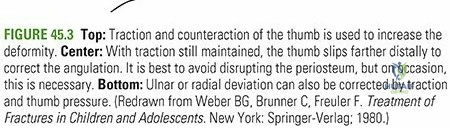
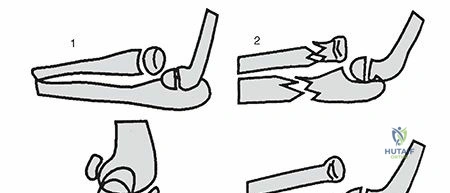
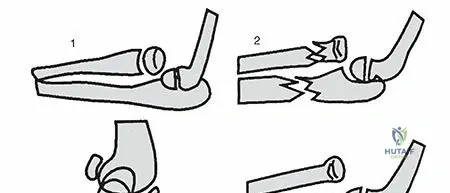
- Recreation of Deformity: Counterintuitively, the first step is often to exaggerate the existing deformity. This unlocks the cortical edges and relaxes the intact periosteal hinge on the concave side.
- Traction and Translation: While maintaining the exaggerated angulation, longitudinal traction is applied, and the distal fragment is translated to achieve cortical apposition.
- Correction of Angulation: The intact periosteal hinge is then utilized as a tension band. The distal fragment is rotated into alignment with the proximal fragment (supination for proximal fractures, neutral for midshaft, pronation for distal), and the angular deformity is corrected. The periosteal hinge prevents over-reduction.
Long Arm Cast Application Technique
A poorly applied cast will inevitably lead to loss of reduction. The cast must be viewed as a definitive orthosis, not merely a protective shell.
A stockinette is applied smoothly over the arm, extending from the proximal humerus to the metacarpophalangeal joints. Wrinkles must be meticulously avoided, particularly in the antecubital fossa, to prevent pressure necrosis.
Cast padding (Webril or cotton) is applied with a 50% overlap. Two to three layers are standard. Extra padding is critical over bony prominences: the olecranon, the radial styloid, the ulnar styloid, and the epicondyles. However, excessive padding globally will increase the padding index, leading to a loose cast and subsequent loss of reduction.
Plaster or fiberglass is then applied. Plaster allows for superior molding but is heavier and radiopaque. A common hybrid technique involves a plaster base layer for molding, overwrapped with fiberglass for durability. The water temperature should be tepid; hot water accelerates the exothermic reaction of plaster and fiberglass, risking thermal burns to the pediatric skin.
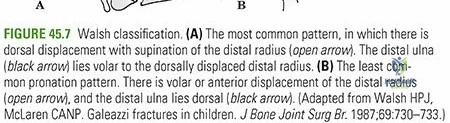
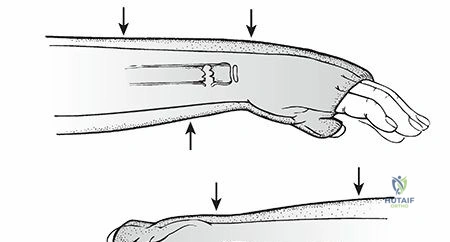
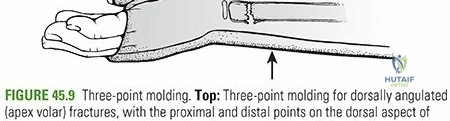
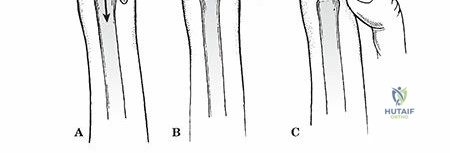
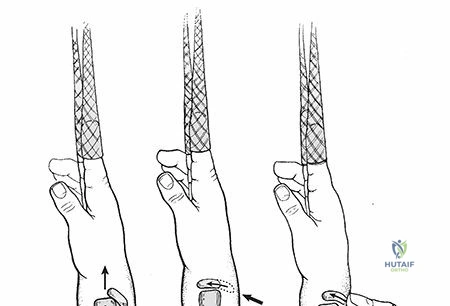
The molding technique is the most critical phase. The surgeon must apply a three-point mold to counteract the deforming forces.
* For an apex volar fracture, pressure is applied volarly directly over the apex of the fracture, with counter-pressure applied dorsally at the proximal and distal extents of the cast.
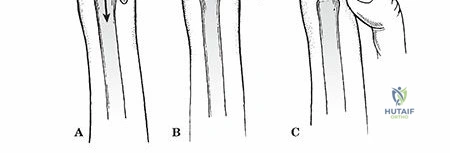
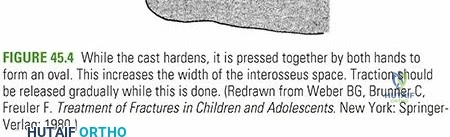
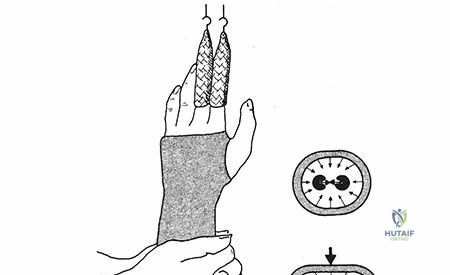
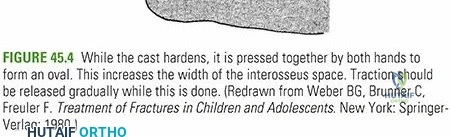
* An interosseous mold is essential. The surgeon uses the thenar eminences to compress the cast gently between the radius and ulna in the AP plane. This maintains the interosseous space, prevents synostosis, and helps restore the radial bow.
The cast must be extended proximally to the axillary crease to control forearm rotation, with the elbow flexed to 90 degrees. Distally, the cast should end proximal to the metacarpophalangeal joints dorsally and at the distal palmar crease volarly to allow full metacarpophalangeal flexion.
To objectively evaluate cast quality, the Cast Index and Canterbury Index are utilized. The Cast Index is the ratio of the sagittal width to the coronal width of the cast at the fracture site measured on radiographs. A Cast Index of less than 0.9 is associated with a significantly lower risk of redisplacement.