Mastering Medial Clavicle Excision and SCJ Reconstruction

Key Takeaway
This masterclass provides an exhaustive, real-time guide to medial clavicle excision and sternoclavicular joint reconstruction. We cover comprehensive surgical anatomy, meticulous preoperative planning, and granular intraoperative steps, from incision to closure. Emphasis is placed on neurovascular protection, precise hardware application, and managing potential complications, ensuring fellows gain critical insights for successful patient care.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues, to this exhaustive exploration of one of the most anatomically unforgiving and technically demanding regions in orthopedic surgery: the sternoclavicular joint (SCJ). Today, we are undertaking a comprehensive analysis of medial clavicle excision for symptomatic, refractory osteoarthritis, seamlessly integrated with the intricate nuances of sternoclavicular joint reconstruction for chronic instability. The SCJ represents the sole true synovial articulation between the axial skeleton and the upper extremity. Because of this unique biomechanical role, it is subjected to immense, repetitive loads during almost all upper extremity kinematics, rendering it susceptible to both degenerative wear and traumatic disruption.
While degenerative joint disease of the SCJ is relatively common—frequently noted incidentally on chest radiographs or computed tomography (CT) scans of patients over the age of fifty—it is uncommonly symptomatic enough to warrant surgical intervention. However, when conservative modalities such as targeted physical therapy, non-steroidal anti-inflammatory drugs (NSAIDs), and intra-articular corticosteroid injections fail, surgical excision of the medial clavicle becomes a highly effective, albeit technically perilous, solution. Conversely, SCJ instability, whether resulting from high-energy anterior or posterior dislocations or insidious atraumatic laxity, presents a distinct set of surgical challenges. Posterior dislocations, in particular, are genuine orthopedic emergencies due to the immediate threat they pose to the retrosternal mediastinal structures.
The surgical management of this joint requires an unparalleled mastery of regional anatomy. The margin for error is virtually non-existent; a millimeter of over-penetration during drilling or a momentary lapse in retractor placement can result in catastrophic, life-threatening hemorrhage or airway compromise. Therefore, mastering these procedures is not merely about learning a sequence of surgical steps; it requires cultivating a profound, healthy respect for the vital structures that lie immediately deep to the operative field. It demands meticulous preoperative planning, rigorous intraoperative discipline, and the humility to involve multidisciplinary teams, including thoracic or vascular surgeons, when the pathology dictates.
In this definitive textbook chapter, we will dissect the patho-anatomy, outline stringent indications and contraindications, detail the preoperative workup, and provide a masterclass on the step-by-step execution of both medial clavicle excision and autograft reconstruction. We will also navigate the treacherous waters of potential complications, equipping you with the knowledge to either avoid them entirely or manage them decisively should they occur.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel ever touches the skin, the orthopedic surgeon must possess a three-dimensional, highly granular understanding of the SCJ and its surrounding topography. The SCJ is a true diarthrodial joint, specifically classified as a saddle-shaped (sellar) joint. This unique morphological design is what grants the shoulder girdle its extraordinary range of motion, allowing the clavicle to elevate up to 35 degrees, depress 10 degrees, protract and retract up to 35 degrees, and axially rotate up to 50 degrees during full overhead elevation. However, this vast mobility dictates that the bony architecture provides almost zero inherent stability.
Osteology and Articular Configuration
The articulation occurs between the bulbous, medial end of the clavicle, the superolateral clavicular notch of the manubrium sterni, and the superior aspect of the first costal cartilage. The articular surfaces are highly incongruent; less than half of the medial clavicle actually articulates with the manubrium at any given time. To mitigate this incongruence and absorb joint reactive forces, an intra-articular disc of dense fibrocartilage completely divides the joint space into two distinct synovial cavities. This disc is firmly attached to the superior and posterior margins of the clavicle and inferiorly to the first costal cartilage, essentially functioning as a dynamic hinge that prevents medial displacement of the clavicle over the manubrium.
Because the bony anatomy offers minimal constraint, the stability of the SCJ is entirely reliant on a robust, complex network of intrinsic and extrinsic ligamentous restraints. The anterior and posterior sternoclavicular ligaments are essentially focal thickenings of the joint capsule. Biomechanical studies have definitively proven that the posterior capsule is the most critical structure for AP stability. It is significantly thicker and stronger than its anterior counterpart, acting as the primary barrier preventing the clavicle from migrating posteriorly into the mediastinum. The anterior capsule, while less robust, acts as a secondary restraint to anterior translation and superior displacement.
Ligamentous Stabilizers and Muscular Intervals
Beyond the capsular ligaments, the extrinsic ligaments are paramount. The costoclavicular ligament (also known as the rhomboid ligament) is a short, incredibly strong, bipartite structure consisting of an anterior (conoid-like) and posterior (trapezoid-like) fasciculus. It originates from the superior aspect of the first rib and inserts onto the inferior surface of the medial clavicle, approximately 1 to 1.5 centimeters lateral to the joint line. This ligament is the absolute primary stabilizer of the SCJ, serving as the fulcrum for all clavicular motion. During a medial clavicle excision, it is a strict surgical imperative to resect no more than 10 to 15 millimeters of bone to preserve the insertion of the costoclavicular ligament; violating this rule will result in iatrogenic, intractable instability of the remaining clavicle.
The muscular anatomy surrounding the SCJ dictates our surgical approach and provides vital landmarks. The platysma is a thin, superficial muscle layer that must be incised to access the deeper fascia. Deep to the platysma lies the sternocleidomastoid (SCM) muscle. The sternal head of the SCM originates via a rounded, tendinous fasciculus from the anterior surface of the manubrium, while the clavicular head originates from the superior border of the medial third of the clavicle. The interval between these heads, or deep to the sternal head, forms our primary working window. It is crucial to mobilize rather than transect the sternal head of the SCM to prevent postoperative cosmetic deformity and functional weakness in cervical rotation.
Inferiorly, the clavicular origin of the pectoralis major muscle attaches to the anterior surface of the medial half of the clavicle. While usually out of the direct zone of a simple excision, its superior fibers may need to be mobilized during complex reconstructions or when addressing inferiorly displaced fractures. Understanding these muscular attachments is vital for achieving adequate exposure while minimizing collateral soft tissue damage that could compromise postoperative rehabilitation.
Neurovascular Proximity and the Retrosternal Danger Zone
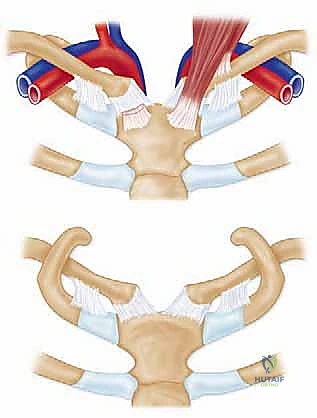
The most terrifying and critical aspect of SCJ surgery is the immediate posterior proximity of the mediastinal "Danger Zone." The retrosternal space houses some of the most vital vascular and visceral structures in the human body. Directly posterior to the manubrium and the right SCJ lies the brachiocephalic (innominate) artery and the confluence of the internal jugular and subclavian veins forming the brachiocephalic vein. On the left side, the left common carotid artery and left subclavian artery ascend in perilous proximity to the joint.
Furthermore, the internal mammary (internal thoracic) artery and vein run vertically approximately 1 to 2 centimeters lateral to the sternal border, passing directly deep to the first costal cartilage. Any dissection, drilling, or retractor placement inferior or deep to the first rib puts these vessels at extreme risk. Laceration of these major vessels in this confined space leads to massive, rapidly fatal hemorrhage that is incredibly difficult to control without an immediate sternotomy.
Beyond the vasculature, the trachea and esophagus lie slightly medial and posterior, vulnerable during severe posterior dislocations. The neural network is equally complex; the vagus nerve, phrenic nerve, and the recurrent laryngeal nerves (particularly the left, which loops under the aortic arch) transit through this thoracic inlet. Iatrogenic injury can result in vocal cord paralysis or diaphragmatic hemiparesis. Finally, the apical pleura of the lungs extends superiorly into the base of the neck, making pneumothorax a very real complication of aggressive deep dissection. This anatomical reality dictates that all posterior work must be performed with blunt instruments, subperiosteal dissection, and the mandatory use of protective retractors (like a malleable ribbon or a specialized sternal retractor) placed between the bone and the mediastinum.
Exhaustive Indications and Contraindications
Patient selection is the cornerstone of successful SCJ surgery. The decision to proceed with either a medial clavicle excision or a complex joint reconstruction must be based on a rigorous clinical evaluation, advanced imaging, and a documented failure of exhaustive conservative management. The pathologies affecting this joint are diverse, and applying the wrong procedure to a specific pathology (e.g., performing an isolated excision on an unstable joint) will inevitably lead to disastrous clinical outcomes.
For degenerative conditions, osteoarthritis is the most common indication for medial clavicle excision. This is frequently seen in post-menopausal women, heavy manual laborers, or patients with a history of prior neck dissections that altered shoulder girdle biomechanics. Systemic inflammatory arthropathies, such as rheumatoid arthritis, ankylosing spondylitis, and psoriatic arthritis, can also severely destroy the SCJ, often bilaterally. In these cases, excision provides excellent pain relief. Rare conditions like condensing osteitis of the clavicle, Friedrich's disease (avascular necrosis of the medial clavicle), and sternoclavicular hyperostosis may also necessitate surgical resection when non-operative measures are exhausted.
Conversely, surgical reconstruction is indicated for chronic, symptomatic instability. Acute anterior dislocations are often treated non-operatively with a sling, as they are generally well-tolerated and rarely cause functional deficits, despite a persistent cosmetic bump. However, if an anterior dislocation remains painfully unstable and limits function, reconstruction is warranted. Acute posterior dislocations are medical emergencies requiring immediate closed reduction under general anesthesia in the operating room, with thoracic surgery on standby. If closed reduction fails, or if the joint remains grossly unstable post-reduction, open reduction and ligamentous reconstruction are mandatory to protect the retrosternal structures.
| Clinical Pathology | Primary Indication | Recommended Procedure | Absolute Contraindications |
|---|---|---|---|
| Primary Osteoarthritis | Refractory pain, failed conservative Tx | Medial Clavicle Excision (<15mm) | Concomitant SCJ Instability |
| Rheumatoid Arthritis | Severe joint destruction, intractable pain | Medial Clavicle Excision | Active systemic infection |
| Acute Posterior Dislocation | Failed closed reduction, vascular compromise | Open Reduction + Reconstruction | Lack of thoracic surgery backup |
| Chronic Anterior Instability | Painful popping, severe functional limitation | Figure-of-8 Autograft Reconstruction | Asymptomatic cosmetic deformity |
| Atraumatic/Voluntary Instability | Extreme pain despite extensive physical therapy | Capsular Plication / Reconstruction | Isolated Medial Clavicle Excision |
| Septic Arthritis | Purulent effusion, systemic sepsis | Urgent I&D, possible delayed excision | Corticosteroid injection |
It is critical to emphasize the contraindications. Performing an isolated medial clavicle excision in the setting of underlying traumatic or atraumatic instability is an absolute contraindication. Removing the medial clavicle eliminates the bony buttress, and if the costoclavicular ligaments are already incompetent, the remaining clavicle will become wildly unstable, leading to severe pain and dysfunction. Furthermore, surgery for purely cosmetic reasons (e.g., a painless bump from a chronic anterior dislocation) is strongly discouraged given the significant surgical risks involved.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the vanguard against intraoperative disasters in SCJ surgery. The standard radiographic workup begins with specialized plain films, including the Serendipity view (a 40-degree cephalic tilt view), which is excellent for assessing superior/inferior displacement. However, plain radiographs are notoriously difficult to interpret due to overlapping mediastinal and thoracic shadows. Therefore, a fine-cut Computed Tomography (CT) scan with 3D reconstructions is the absolute gold standard and is mandatory for all SCJ cases.
Diagnostic Imaging and Workup
The CT scan allows for precise visualization of the articular wear pattern, the presence of subchondral cysts or osteophytes in osteoarthritis, and the exact direction and magnitude of displacement in instability cases. Crucially, a CT angiogram (CTA) should be obtained if there is any suspicion of a posterior dislocation compressing the great vessels, or if the patient has a history of vascular anatomical variants. If the diagnosis of SCJ pain is equivocal, an image-guided (ultrasound or fluoroscopy) intra-articular injection of a local anesthetic (e.g., lidocaine or bupivacaine) can serve as a powerful diagnostic tool. Complete, albeit temporary, relief of symptoms confirms the SCJ as the pain generator.
When planning for a reconstruction, graft selection must be finalized preoperatively. The semitendinosus autograft is the workhorse for SCJ reconstruction due to its superior tensile strength and adequate length to complete a figure-of-8 construct. The patient must be examined preoperatively to ensure the presence of the hamstring tendons, and the ipsilateral leg must be prepped. Alternatively, a palmaris longus autograft can be used for smaller reconstructions or augmentations, though it is absent in approximately 15% of the population. Allograft tissue (e.g., gracilis or semitendinosus) is a viable alternative to eliminate donor site morbidity, though it carries a theoretically higher risk of incorporation failure or infection.
Patient Setup and Operating Room Configuration
The operating room setup requires specific attention. The patient is positioned supine on a standard radiolucent operating table. A crucial step is the placement of a small rolled towel or a dedicated shoulder bump vertically between the scapulae. This maneuver gently extends the upper thoracic spine and allows the shoulders to fall posteriorly, thereby thrusting the sternum and medial clavicles anteriorly. This subtle postural adjustment significantly opens the surgical field and makes the SCJ more accessible. The head should be stabilized in a neutral position, avoiding extreme rotation that could distort the cervical anatomy.

The ipsilateral arm is placed on a padded arm board, allowing the surgeon to manipulate the arm intraoperatively to assess joint kinematics and stability. The surgical prep must be extensive. We prep and drape the patient from the mandible superiorly to the umbilicus inferiorly, and laterally to the mid-axillary lines bilaterally. This "hemi-clamshell" prep is non-negotiable; in the event of a catastrophic vascular injury requiring an emergent median sternotomy or thoracotomy, the thoracic surgeon must have immediate, unobstructed access to the entire chest without breaking scrub to re-prep.
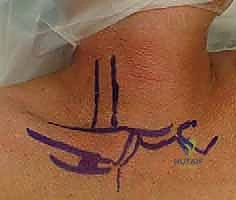
Prior to draping, precise anatomical landmarks are marked with a surgical pen. We outline the medial third of the clavicle, the sternoclavicular joint line, the manubrium, and the sternal notch. The planned incision is marked following Langer's lines—a curvilinear, necklace-type incision approximately 5 to 7 centimeters long, centered over the SCJ. This incision heals with a superior cosmetic result compared to a straight transverse or longitudinal incision, minimizing the risk of hypertrophic scarring in this highly visible area.
Step-by-Step Surgical Approach and Fixation Technique
With the patient prepped, the thoracic surgeon notified and available, and the surgical team briefed on the critical steps and potential hazards, we proceed with the operation. The following details the masterclass execution of both medial clavicle excision and the subsequent steps for a figure-of-8 SCJ reconstruction.
Superficial Dissection and Exposure
- Skin and Subcutaneous Incision: Utilizing a #15 scalpel, the skin is incised sharply along the pre-marked curvilinear Langer's line over the medial clavicle and manubrium. Hemostasis of the dermal and subcutaneous vessels is achieved meticulously with bipolar or monopolar electrocautery.
- Platysma Division: Subcutaneous flaps are developed superiorly and inferiorly using sharp dissection and Metzenbaum scissors to expose the underlying platysma muscle. The platysma is then incised in line with the skin incision. It is vital to maintain the integrity of the platysma flaps for a robust, layered closure later, which prevents adherence of the skin to the underlying bone.

- Identifying the SCM and Capsule: Deep to the platysma, the deep cervical fascia is encountered. The sternal and clavicular heads of the sternocleidomastoid (SCM) muscle are identified. The anterior capsule of the SCJ lies directly deep to the interval between the SCM and the medial clavicle. We carefully mobilize the sternal head of the SCM laterally and superiorly using a combination of blunt dissection and careful electrocautery, preserving its tendinous origin on the manubrium as much as possible.

Medial Clavicle Excision Technique
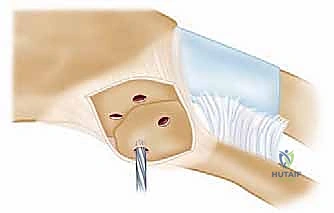
- Capsulotomy and Subperiosteal Dissection: An H-shaped or longitudinal incision is made through the anterior capsule of the SCJ. Using a sharp Cobb elevator or a Freer elevator, the capsule and periosteum are elevated off the anterior, superior, and inferior aspects of the medial clavicle.
- The Posterior Danger Zone: This is the most critical step of the excision. Dissection along the posterior aspect of the medial clavicle must be strictly subperiosteal. We utilize a curved elevator (such as a Darrach or a specialized rib elevator) to carefully strip the posterior capsule and periosteum, staying intimately on the bone. Once the posterior space is created, a malleable ribbon retractor or a blunt Crego elevator is meticulously placed behind the medial clavicle to physically shield the brachiocephalic vessels and pleura from our cutting instruments.

- Osteotomy: The extent of resection is marked precisely using a sterile ruler. We strictly adhere to resecting no more than 10 to 15 millimeters of the medial clavicle to ensure the costoclavicular ligaments remain entirely intact. Using a narrow, fine-toothed oscillating saw or a high-speed cutting burr, the osteotomy is performed from anterior to posterior. The blade must be directed slightly laterally to match the natural contour of the joint. The protective retractor behind the bone must be visualized at all times during the cut.


- Fragment Removal and Debridement: Once the osteotomy is complete, the medial fragment is grasped with a towel clip or strong tenaculum and carefully enucleated from its remaining soft tissue attachments. The intra-articular disc, which is often degenerative and shredded in osteoarthritic patients, is excised using a rongeur and scalpel. The remaining lateral clavicular stump is then smoothed with a rasp or burr to prevent soft tissue irritation.



Sternoclavicular Joint Reconstruction Strategies
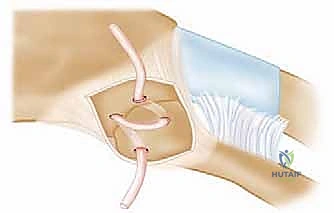
If the procedure is being performed for instability, or if iatrogenic instability is noted following an excision, a reconstruction must be performed. We favor the figure-of-8 autograft reconstruction using a semitendinosus tendon, as popularized by Spencer and Kuhn, due to its biomechanical superiority.
- Drill Hole Preparation: After the joint is reduced, drill holes must be created in both the manubrium and the medial clavicle. For the clavicle, two 4.5mm drill holes are placed superior to inferior, approximately 1cm and 2cm lateral to the joint line. For the manubrium, two corresponding holes are drilled anterior to posterior. Crucial Safety Step: When drilling the manubrium, a protective retractor MUST be placed deep to the sternum to prevent the drill bit from plunging into the mediastinum.


- Graft Passage: A suture shuttle (e.g., a Hewson slider or a looped passing wire) is used to navigate the drill holes. The harvested semitendinosus autograft is whip-stitched at both ends with high-strength non-absorbable suture. The graft is passed through the manubrial holes and then crossed in a figure-of-8 configuration before being passed through the clavicular holes.



- Tensioning and Fixation: The joint is held in an anatomically reduced position. The graft limbs are tensioned maximally. Fixation
Clinical & Radiographic Imaging Archive