Find Relief from Shoulder DJD: Arthroscopic Débridement and Glenoidplasty

Key Takeaway
Looking for accurate information on Find Relief from Shoulder DJD: Arthroscopic Débridement and Glenoidplasty? Arthroscopic débridement and glenoidplasty are surgical options for shoulder degenerative joint disease when conservative treatments fail or joint replacement is not desired. These procedures address coexisting pathologies like loose bodies, osteophytes, and cartilage defects. The goal of arthroscopic débridement and glenoidplasty is to provide symptomatic relief, particularly for patients with early or severe arthritis who may be younger or highly active.
Introduction and Epidemiology
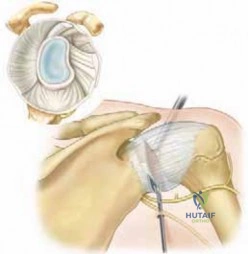
Osteoarthritis of the glenohumeral joint is a progressive, degenerative disorder of synovial joints characterized by focal defects in the articular cartilage, accompanied by reactive involvement in the subchondral and marginal bone, synovium, and para-articular structures. Patients presenting with degenerative joint disease of the shoulder frequently exhibit a constellation of coexisting intra-articular and extra-articular pathology. This includes chronic bursitis, hypertrophic synovitis, osteochondral loose bodies, degenerative labral tears, peripheral osteophytes, and variable grades of articular cartilage defects.
The management of glenohumeral degenerative joint disease in young, active, or high-demand patients remains a complex and unresolved clinical problem in orthopedic surgery. While total shoulder arthroplasty provides excellent pain relief and functional restoration in older, low-demand populations, its application in younger demographics is limited by concerns regarding premature component wear, aseptic loosening, and the eventual need for complex revision arthroplasty. Consequently, joint-preserving techniques are highly sought after for this specific patient cohort.
Arthroscopic management, encompassing joint débridement, capsular release, subacromial decompression, and glenoidplasty, serves as a viable, minimally invasive surgical alternative. The primary objective of these arthroscopic interventions is not to halt or reverse the biological progression of osteoarthritis, but rather to provide a substantial period of symptomatic relief, improve range of motion, and delay the necessity of arthroplasty.
Pathogenesis of Glenohumeral Osteoarthritis
Osteoarthritis can be classified as primary, wherein no obvious underlying etiology is identified, or secondary, which is preceded by a predisposing disorder such as trauma, chronic instability, avascular necrosis, or inflammatory arthropathy. The disease process in the shoulder parallels that of weight-bearing joints. Degenerative alterations typically initiate within the articular cartilage, driven by either excessive biomechanical loading of a healthy joint or normal physiological loading across a previously disturbed joint interface.
At the cellular and biochemical level, progressive asymmetric narrowing of the joint space and fibrillation of the articular cartilage occur secondary to increased cartilage degradation and diminished proteoglycan and collagen synthesis. Matrix metalloproteinases and pro-inflammatory cytokines such as Interleukin-1 and Tumor Necrosis Factor-alpha play critical roles in this catabolic cascade. As the articular cartilage is denuded, subchondral sclerosis develops in regions of elevated contact pressure. When mechanical stresses exceed the yield strength of the subchondral bone, it responds with vascular invasion, increased cellularity, and the formation of peripheral osteophytes, which further restrict joint kinematics and exacerbate capsular contracture.
Surgical Anatomy and Biomechanics
A profound understanding of the osseous architecture and capsuloligamentous stabilizers of the glenohumeral joint is imperative for executing a safe and effective arthroscopic débridement and glenoidplasty.
Osseous Architecture
The normal proximal humeral anatomy is characterized by a head-shaft angle of approximately 130 degrees, with an average of 30 degrees of retroversion relative to the transepicondylar axis of the distal humerus. The articular surface area of the humeral head is significantly larger than that of the glenoid fossa, a geometric mismatch that permits a massive global range of motion at the expense of inherent osseous stability.

The glenoid fossa provides a relatively shallow, pear-shaped socket for humeral articulation. Glenoid version, defined as the angle formed between the center of the glenoid articular surface and the longitudinal axis of the scapular body, averages roughly 3 degrees of retroversion. Maintenance of this version is critical for dynamic stability. In the osteoarthritic shoulder, asymmetric wear patterns, particularly posterior erosion seen in Walch B2 glenoids, can significantly alter this version, leading to static posterior subluxation of the humeral head.
Capsuloligamentous Stabilizers
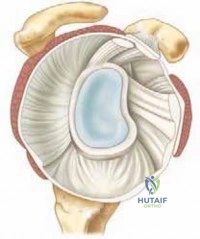
The glenoid labrum is a vital fibrocartilaginous structure that circumferentially surrounds the periphery of the glenoid. By functioning as a bumper, the labrum increases the depth of the glenoid concavity by approximately 50%, thereby greatly enhancing the static stability of the glenohumeral joint through the concavity-compression mechanism.

The capsuloligamentous structures provide the primary static stabilization for the shoulder joint. Within this capsular envelope exist three distinct, biomechanically significant thickenings:
1. Superior glenohumeral ligament
2. Middle glenohumeral ligament
3. Inferior glenohumeral ligament complex
The rotator interval, a triangular anatomic space bordered by the supraspinatus superiorly, the subscapularis inferiorly, and the coracoid process medially, contains the coracohumeral ligament and the superior glenohumeral ligament. In degenerative joint disease, profound contracture of these capsular structures, particularly the rotator interval and the inferior capsular pouch, is the primary driver of the severe range of motion deficits observed clinically.
Indications and Contraindications
Patient selection is the single most critical determinant of success in the arthroscopic management of shoulder degenerative joint disease. Historically, ideal candidates are those with early osteoarthritis in whom concentric glenohumeral articulation is maintained, evidenced by a visible joint space on a true axillary radiograph.

Young or middle-aged patients, laborers, and athletes who subject their shoulders to high loads or repetitive impacts are prime candidates, provided conservative modalities such as physical therapy, non-steroidal anti-inflammatory drugs, and intra-articular corticosteroid injections have been exhausted.
Patient Selection Criteria
The decision matrix for proceeding with arthroscopic débridement versus arthroplasty relies heavily on the Walch classification of glenoid morphology and the patient's physiological age and functional demands.
| Clinical Scenario | Operative Indications for Arthroscopy | Non-Operative or Arthroplasty Indications |
|---|---|---|
| Patient Age and Demand | Age < 55, high physical demand, heavy manual laborer, overhead athlete. | Age > 65, low physical demand, sedentary lifestyle (favor Arthroplasty). |
| Glenoid Morphology | Walch A1, A2, or early B1 (concentric wear, maintained version). | Walch B2 (biconcave), B3, or C (severe dysplastic retroversion) (favor Arthroplasty). |
| Joint Space | Maintained joint space (>2mm) on axillary radiograph, or focal chondral defects. | Complete bone-on-bone articulation with massive osteophytosis. |
| Symptoms | Mechanical symptoms (catching, locking from loose bodies), stiffness secondary to capsular contracture. | Refractory rest pain, severe night pain unresponsive to all conservative measures. |
| Cuff Integrity | Intact rotator cuff, or reparable tears without significant fatty infiltration. | Massive, irreparable rotator cuff tears with cuff tear arthropathy (favor rTSA). |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning begins with a comprehensive radiographic evaluation. A standard shoulder series must include a true anteroposterior view (Grashey view), a scapular Y view, and a true axillary view. The axillary view is paramount for assessing joint space narrowing, glenoid version, and posterior humeral head subluxation.

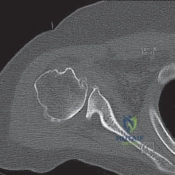
Imaging Modalities
Advanced imaging is frequently required. Computed Tomography without contrast is the gold standard for evaluating glenoid bone stock, quantifying retroversion, and assessing the size and location of humeral and glenoid osteophytes. Magnetic Resonance Imaging is utilized to evaluate the integrity of the rotator cuff musculature, the long head of the biceps tendon, and the presence of subchondral cysts or marrow edema, which may influence the surgical approach regarding biceps tenodesis or concomitant cuff repair.
Operating Room Setup
Arthroscopic shoulder surgery for degenerative joint disease can be performed in either the beach chair or the lateral decubitus position, depending on surgeon preference.

The beach chair position offers the advantage of an upright anatomical orientation, facilitating easier conversion to an open arthroplasty if deemed necessary intraoperatively. It also allows for dynamic examination of shoulder range of motion during the capsular release. Conversely, the lateral decubitus position with longitudinal and lateral traction provides superior joint distraction, which can be highly beneficial when navigating a tight, contracted osteoarthritic joint space. Regardless of positioning, a regional interscalene nerve block is strongly recommended to minimize intraoperative anesthetic requirements and optimize immediate postoperative pain control.
Detailed Surgical Approach and Technique
There are four fundamental pillars of arthroscopic treatment in a patient with degenerative joint disease of the shoulder: glenohumeral joint débridement, capsular release, subacromial decompression, and glenoidplasty. The Comprehensive Arthroscopic Management approach systematically addresses each of these components to maximize postoperative functional gains.
Portal Placement and Diagnostic Arthroscopy
Standard posterior, anterior, and lateral portals are utilized. The posterior portal is established first, typically 2 centimeters inferior and 1 centimeter medial to the posterolateral corner of the acromion. Due to severe capsular contracture and osteophyte formation, initial entry into the glenohumeral joint can be challenging. A spinal needle is used to localize the ideal trajectory, aiming for the coracoid process.
Once the arthroscope is introduced, a thorough diagnostic sweep is performed. An anterior portal is established via an outside-in technique through the rotator interval, utilizing a clear cannula to facilitate instrument passage.
Glenohumeral Joint Debridement and Synovectomy
The initial step involves a comprehensive synovectomy and removal of all osteochondral loose bodies. Hypertrophic synovitis is a major pain generator in osteoarthritis; therefore, an aggressive mechanized shaver and radiofrequency ablation wand are used to clear the synovium, particularly in the rotator interval and axillary pouch.
Chondroplasty is performed to débride unstable, fibrillated articular cartilage flaps to a stable rim. Care must be taken not to aggressively penetrate the subchondral bone during this phase, as the goal is to remove mechanical irritants, not to strip remaining viable cartilage. Degenerative, unstable portions of the labrum are carefully trimmed back to a stable base, preserving as much of the labral bumper as possible to maintain concavity-compression.
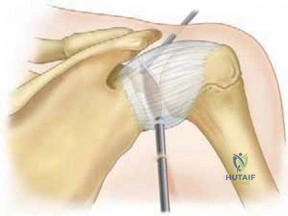
Global Capsular Release
Capsular release is arguably the most critical step for restoring range of motion. The release typically begins anteriorly at the rotator interval. The coracohumeral ligament and superior capsule are resected to restore external rotation with the arm at the side.
The release is then carried inferiorly through the middle and inferior glenohumeral ligaments. When performing the inferior capsulotomy at the 6 o'clock position, meticulous care is required to avoid iatrogenic injury to the axillary nerve, which lies in close proximity (often within 10 to 15 millimeters) to the inferior capsule. Using a radiofrequency device with the active tip directed superiorly toward the glenoid, rather than inferiorly toward the axillary recess, mitigates this risk. The release is completed posteriorly to restore internal rotation, effectively creating a 360-degree capsulotomy.
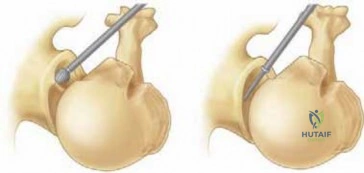
Glenoidplasty and Osteophyte Resection
Glenoidplasty involves the recontouring of the glenoid articular surface and the resection of impinging peripheral osteophytes. A motorized burr is introduced to smooth eburnated subchondral bone and resect large, mechanically obstructive osteophytes.
The "goat's beard" osteophyte, a large exostosis frequently found on the inferior aspect of the humeral head, stretches the axillary pouch and physically blocks adduction and rotation. Resection of this inferior humeral osteophyte is essential for restoring the axillary recess volume. Additionally, posterior glenoid osteophytes are contoured to reduce mechanical impingement during external rotation and abduction. In cases of focal full-thickness chondral defects, microfracture may be performed to stimulate fibrocartilage in-growth, though its efficacy in diffuse osteoarthritis is limited.
Subacromial Decompression and Biceps Management
The long head of the biceps tendon is frequently degenerative, flattened, and inflamed in the setting of shoulder osteoarthritis. If significant pathology is noted, an arthroscopic biceps tenotomy or tenodesis is performed, as the biceps is a well-documented pain generator.
Finally, the arthroscope is redirected into the subacromial space. A thorough bursectomy is performed to evaluate the bursal surface of the rotator cuff. If there is evidence of subacromial impingement or a type III hooked acromion contributing to the patient's symptomology, an acromioplasty is executed using a motorized burr to smooth the anteroinferior acromial surface and resect the coracoacromial ligament.
Complications and Management
While arthroscopic management of shoulder degenerative joint disease is generally safe and minimally invasive, specific intraoperative and postoperative complications can occur. Thorough preoperative counseling regarding the palliative nature of the procedure is essential to align patient expectations with surgical realities.

Failure to achieve lasting pain relief is the most common "complication," ultimately representing the natural progression of the underlying osteoarthritic disease process rather than a true surgical failure.
| Complication | Incidence / Risk Factors | Prevention and Salvage Strategy |
|---|---|---|
| Axillary Nerve Injury | < 1%. Highest risk during inferior capsular release at the 6 o'clock position. | Prevention: Direct radiofrequency ablation tip toward the glenoid. Stay intra-articular. Salvage: Observation for neurapraxia; nerve exploration/grafting if no recovery by 3-6 months. |
| Postoperative Stiffness | 5-10%. Risk increased with inadequate capsular release or poor postoperative compliance. | Prevention: Ensure complete 360-degree release and immediate postoperative motion. Salvage: Aggressive physical therapy, intra-articular corticosteroids, revision arthroscopic release. |
| Chondrolysis | Rare. Historically associated with continuous intra-articular pain pumps (bupivacaine). | Prevention: Avoid intra-articular local anesthetic pumps. Limit thermal energy usage on articular cartilage. Salvage: Progression to total shoulder arthroplasty. |
| Progression of Osteoarthritis | 100% over time. This is a palliative, not curative, procedure. | Prevention: Appropriate patient selection (avoid Walch B2/B3). Salvage: Transition to anatomic or reverse total shoulder arthroplasty when symptoms become refractory. |
| Infection | < 0.5%. | Prevention: Strict sterile technique, preoperative prophylactic antibiotics. Salvage: Arthroscopic irrigation and débridement, culture-specific intravenous antibiotics. |
Post Operative Rehabilitation Protocols
The success of an arthroscopic capsular release and débridement is heavily dependent on the postoperative rehabilitation protocol. Because the primary goal is the restoration and maintenance of range of motion, prolonged immobilization is strictly contraindicated.
Phased Recovery Strategy
Phase I: Immediate Motion (Weeks 0-2)
Patients are placed in a simple clinical sling purely for comfort and are encouraged
Clinical & Radiographic Imaging

