Capsular Releases for Loss of Motion: Restore Your Shoulder

Key Takeaway
Discover the latest medical recommendations for Capsular Releases for Loss of Motion: Restore Your Shoulder. Arthroscopic capsular releases for loss of motion address shoulder stiffness or adhesive capsulitis, stemming from soft tissue scarring, contracture, or adhesions. This procedure involves releasing specific contracted capsular structures and adhesions, which can be intra-articular, subacromial, or subdeltoid. It aims to safely restore range of motion, treating both primary (idiopathic) and secondary forms of the condition.
Comprehensive Introduction and Patho-Epidemiology
Definition and Classification of Shoulder Stiffness
Shoulder stiffness is a profoundly debilitating clinical entity that can arise from a multitude of etiologies, fundamentally characterized by a restriction in both active and passive glenohumeral range of motion. This loss of motion is typically a function of soft tissue scarring, capsular contracture, or underlying osseous changes. When the stiffness is primarily due to capsular fibrosis and inflammation without an underlying structural or osseous cause, it is classically termed adhesive capsulitis or "frozen shoulder." The essential tenet of treating the stiff shoulder lies in accurately recognizing the anatomic region responsible for the stiffness and releasing the specific structures in this region in a controlled, systematic fashion.
Clinically, adhesive capsulitis is principally divided into two primary forms that result in a significant loss of range of motion and can be safely addressed via arthroscopic capsular releases. The first is primary (idiopathic) adhesive capsulitis, which occurs without a clear inciting event and is characterized by a spontaneous onset of progressive pain and stiffness. The second is secondary adhesive capsulitis, which develops in response to a known intrinsic or extrinsic trigger. Secondary adhesive capsulitis is further subclassified into three categories: metabolic (strongly associated with diabetes mellitus and thyroid disorders), posttraumatic (following fractures, dislocations, or significant soft tissue injuries), and postoperative (arising iatrogenically after procedures such as rotator cuff repair, labral repair, or historically, Putti-Platt and Magnuson-Stack procedures).


The distinction between these classifications is not merely academic; it profoundly influences the expected natural history, the response to nonoperative management, and the ultimate surgical strategy. For instance, adhesive capsulitis in diabetic patients tends to be significantly more protracted, more resistant to nonoperative treatment, and carries a higher risk of recurrence following surgical intervention compared to idiopathic cases. Furthermore, shoulder stiffness can result from a combination of intra-articular adhesions, capsular contracture, subacromial adhesions, and subdeltoid adhesions. A comprehensive understanding of this complex interplay is paramount for the orthopedic surgeon attempting to restore normal glenohumeral kinematics.
Pathogenesis and the Stages of Adhesive Capsulitis
The pathogenesis of primary adhesive capsulitis is characterized by a complex, cytokine-mediated inflammatory response that ultimately leads to dense fibroblastic proliferation and capsular contracture. At a cellular level, the condition is marked by an initial phase of severe synovitis, followed by the proliferation of myofibroblasts and a shift in collagen synthesis. Normal type I collagen of the joint capsule is progressively replaced by disorganized type III collagen, leading to a thickened, non-compliant capsuloligamentous complex. The release of cytokines such as transforming growth factor-beta (TGF-β), platelet-derived growth factor (PDGF), and various interleukins drives this aberrant fibrotic cascade, similar to the pathophysiology observed in Dupuytren's contracture.
Clinically, the pathogenesis of frozen shoulder has historically been divided into three distinct, albeit overlapping, stages that occur over a variable time course. The first is the "Freezing" or inflammatory stage, which typically lasts from 6 weeks to 9 months. During this phase, patients experience a slow, insidious onset of pain that progressively worsens, accompanied by a gradual loss of motion. The intense synovitis present during this stage makes the shoulder exquisitely painful, particularly at night and at the extremes of motion.

The second stage is the "Frozen" or fibrotic stage, lasting approximately 4 to 9 months or more. In this phase, the intense inflammatory pain begins to slowly subside, but the stiffness becomes profound and rigid. The capsule becomes densely fibrotic and contracted, severely limiting both active and passive motion. The final stage is the "Thawing" phase, which can last anywhere from 5 to 26 months. During this period, shoulder motion gradually returns toward normal as the fibrotic tissue slowly remodels. However, it is critical to note that these stages coexist as a continuum, and individual patients may exhibit variable progression, with some never achieving complete resolution without intervention.
Natural History and Epidemiological Considerations
The natural history of adhesive capsulitis has long been a subject of debate within the orthopedic community. Historically, it was widely taught that frozen shoulder is a self-limiting condition that inevitably resolves over 1 to 3 years. However, contemporary longitudinal studies have challenged this benign view. While the natural history of secondary shoulder stiffness is generally accepted as protracted and often refractory to nonoperative treatment, the time course and end result of primary adhesive capsulitis are now understood to be far less predictable.
In the absence of operative intervention, recent reports have demonstrated measurable restrictions in range of motion at long-term follow-up in 39% to 76% of patients. Furthermore, persistent symptoms, including mild to moderate pain and functional limitations, are reported in up to 50% of patients with adhesive capsulitis. The condition can be exceedingly protracted, with the mean duration of symptoms in some cohorts lasting up to 30 months. This challenges the dogma of "benign neglect" and underscores the need for proactive management in patients who fail to progress.


Interestingly, there is often a weak correlation between the objectively measured restriction in range of motion and the patient's subjective experience of pain and disability. Some patients present with severe, debilitating pain but near-normal range of motion, particularly in the early freezing stage. Conversely, patients in the frozen stage may exhibit profoundly restricted motion but report minimal pain. The impact of restricted range of motion on an individual patient’s quality of life largely depends on their specific functional demands, occupational requirements, and recreational activities. Therefore, treatment decisions must be highly individualized, weighing the patient's functional deficit against the risks of surgical intervention.
Detailed Surgical Anatomy and Biomechanics
Glenohumeral Articulation and Capsuloligamentous Restraints
A profound and highly detailed appreciation of shoulder anatomy is the absolute prerequisite for restoring motion while avoiding catastrophic injury to accompanying nerves, tendons, and vascular structures. Normal shoulder motion occurs principally along two highly coordinated interfaces: the glenohumeral articulation and the scapulothoracic articulation. On average, the normal ratio of glenohumeral motion to scapulothoracic motion is approximately 2:1, with the vast majority of elevation occurring through the glenohumeral joint. When glenohumeral motion is restricted by capsular contracture, patients inevitably develop compensatory, exaggerated scapulothoracic motion, which often leads to secondary periscapular pain and muscle fatigue.
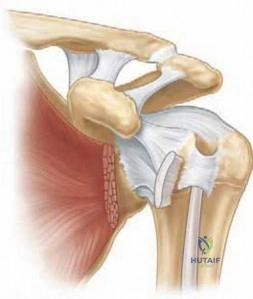
The capsuloligamentous structures of the shoulder contribute critically to the static stability of the joint and act as physiologic check reins at the extremes of motion in their nonpathologic condition. The shoulder capsule is not a uniform structure; rather, it contains distinct, thickened regions known as the glenohumeral ligaments. These include the superior glenohumeral ligament (SGHL), the middle glenohumeral ligament (MGHL), and the inferior glenohumeral ligament (IGHL) complex. The IGHL complex is further subdivided into the anterior band, the axillary fold (or pouch), and the posterior band.

Contracture of these specific capsular regions and ligaments correlates precisely with specific clinical losses of range of motion. This anatomic-biomechanical relationship must be determined preoperatively through rigorous physical examination to guide the arthroscopic release. For instance, the middle glenohumeral ligament primarily restricts external rotation at the midranges of abduction (approximately 45 degrees). The anterior band of the inferior glenohumeral ligament is the primary restraint to external rotation at 90 degrees of abduction. The inferior capsule (axillary pouch) restricts global abduction and forward flexion, while the posterior capsule and the posterior band of the IGHL restrict internal rotation, particularly in abduction and cross-body adduction.
The Rotator Interval and Anterior Capsular Structures
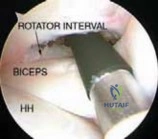
The rotator interval is a critical, complex triangular anatomic region situated between the anterior border of the supraspinatus tendon and the superior border of the subscapularis tendon. The apex of this triangle is at the transverse humeral ligament, and its base is the coracoid process. The rotator interval contains several vital structures, most notably the superior glenohumeral ligament (SGHL), the coracohumeral ligament (CHL), and the intra-articular portion of the long head of the biceps tendon.
In the setting of adhesive capsulitis, the rotator interval is frequently the epicenter of intense inflammation and subsequent fibrotic contracture. The coracohumeral ligament, which originates on the base of the coracoid and inserts onto the greater and lesser tuberosities, becomes severely thickened and contracted. Biomechanically, the structures of the rotator interval (specifically the SGHL and CHL) are the primary restraints to external rotation with the shoulder adducted at the patient's side. Therefore, a profound loss of external rotation with the arm at the side is the hallmark clinical sign of rotator interval contracture.



During normal shoulder motion, the tightening and loosening of the glenohumeral ligaments and capsule are intimately accompanied by the lengthening and shortening of the rotator cuff and deltoid muscles. Several critical tissue planes exist that facilitate this smooth excursion. A plane between the deltoid and humerus (the subdeltoid space) exists that, when scarred from trauma or previous surgery, can severely limit glenohumeral motion. Similarly, a plane between the rotator cuff and the acromion exists, normally occupied by the subacromial bursa. Scar tissue and dense adhesions in this interface can tether the rotator cuff, limiting its excursion and thus profoundly restricting both active and passive glenohumeral joint motion.
Neurovascular Proximity and Surgical Danger Zones
Arthroscopic capsular release is a highly effective procedure, but it is fraught with potential hazards due to the intimate proximity of major neurovascular structures to the capsule. An exacting knowledge of these "danger zones" is non-negotiable. The most critical structure at risk during a global capsular release is the axillary nerve. The axillary nerve branches from the posterior cord of the brachial plexus, runs across the superficial (anterior) surface of the subscapularis, and then dives posteriorly adjacent to the inferior border of the subscapularis.
As the axillary nerve exits the quadrangular space, it is closely juxtaposed to the inferior glenohumeral ligament and the inferior capsule. At the 6 o'clock position (the direct inferior capsule), the axillary nerve lies mere millimeters (often 10-15 mm, but sometimes closer in a contracted state) from the capsular insertion on the humerus. Therefore, anterior and inferior capsular releases must proceed with extreme caution. The release can proceed safely as long as the muscle belly of the subscapularis is visualized superiorly and the release is kept strictly adjacent to the glenoid rim rather than the humeral insertion.


Furthermore, the posterior capsule presents its own unique anatomic challenges. The posterior capsule overlies a distinct layer of rotator cuff muscle (infraspinatus and teres minor) posteriorly adjacent to the glenoid. However, moving more laterally toward the humeral insertion, the posterior rotator cuff tendons and the capsule become intimately juxtaposed and are virtually indistinguishable. Consequently, to avoid catastrophic iatrogenic disruption of the posterior rotator cuff musculature and tendinous insertions, the release of the posterior capsule must be performed meticulously adjacent to the posterior glenoid labrum.
Exhaustive Indications and Contraindications
Clinical Evaluation and Diagnostic Modalities
The evaluation of a patient presenting with shoulder stiffness demands a meticulous history and a comprehensive, structured physical examination. Patients with idiopathic adhesive capsulitis often deny any traumatic event, instead complaining of an insidious onset of vague, deltoid-radiating pain that predates the loss of motion and is notoriously refractory to physical therapy and oral analgesics. Conversely, patients with secondary adhesive capsulitis often present with a clear history of trauma, previous surgery, or significant medical comorbidities. A thorough history must elicit any prior fractures, extended periods of immobilization, or previous surgical interventions (e.g., rotator cuff repair, capsular shift, Bristow-Latarjet, or open reduction and internal fixation).
The physical examination must systematically isolate and assess the various capsuloligamentous constraints. A global loss of both active and passive range of motion is the sine qua non of adhesive capsulitis. Assessing range of motion in a supine position is highly recommended, as it stabilizes the scapula, controls compensatory scapulothoracic motion and lumbar tilt, and yields a far more accurate assessment of true glenohumeral excursion. Passive range of motion must be meticulously compared to the contralateral, unaffected shoulder. A loss of passive external rotation with the arm at the side strongly suggests contracture of the anterosuperior capsule and rotator interval. A loss of passive external rotation in 90 degrees of abduction implicates the anteroinferior capsule. A loss of passive flexion and abduction points to inferior capsular contracture, while a loss of passive internal rotation (measured via cross-chest adduction angle) suggests posterior capsular tightness.


Diagnostic injections are invaluable adjuncts in the clinical evaluation. The Lidocaine injection test involves recording passive and active ROM before and after a subacromial or intra-articular injection of local anesthetic. The post-injection increase in ROM indicates the extent to which the loss of motion is attributable to pain and muscle guarding versus true capsular contracture and adhesions. If motion remains profoundly restricted despite complete pain relief, true structural stiffness is confirmed. Furthermore, intra-articular corticosteroid injections can be both diagnostic and highly therapeutic, particularly in the early inflammatory (freezing) stage of the disease, often halting the fibroblastic cascade if administered promptly.
Indications for Arthroscopic Capsular Release
Arthroscopic capsular release is a highly successful intervention, but it is generally reserved for patients who have failed a rigorous, well-documented course of nonoperative management. Nonoperative treatment—consisting of physical therapy focused on gentle, progressive stretching, NSAIDs, and intra-articular corticosteroid injections—is typically attempted for a minimum of 4 to 6 months. Surgical intervention is indicated in patients with primary or secondary adhesive capsulitis who continue to experience unacceptable pain and functional limitation (such as inability to perform activities of daily living, reach overhead, or sleep on the affected side) despite this conservative regimen.
The threshold for surgical intervention may be adjusted based on the etiology of the stiffness. For instance, patients with postoperative stiffness (e.g., following a prolonged immobilization for a complex proximal humerus fracture) may be offered surgical release earlier if they plateau in therapy, as dense intra-articular and subdeltoid adhesions are unlikely to resolve with stretching alone. Similarly, diabetic patients, who notoriously present with severe, recalcitrant adhesive capsulitis, may require surgical intervention if they show no improvement after several months of dedicated therapy and glycemic control.


It is crucial to differentiate adhesive capsulitis from other pathologies that cause stiffness. The differential diagnosis includes glenohumeral arthritis, acromioclavicular arthritis, large rotator cuff tears (which typically present with a loss of active motion but preserved passive motion), subacromial bursitis, calcific tendinitis, and, importantly, septic arthritis. An equal loss of passive and active range of motion strongly suggests adhesive capsulitis, whereas a significantly greater loss of active than passive motion points toward a structural rotator cuff or neurologic deficit.
Absolute and Relative Contraindications
| Contraindication Type | Specific Condition | Rationale / Clinical Consideration |
|---|---|---|
| Absolute | Active Joint Infection (Septic Arthritis) | Introduction of instruments and fluid can disseminate infection; requires immediate I&D, not a capsular release. |
| Absolute | Severe Glenohumeral Osteoarthritis | Motion loss is due to osseous deformity, osteophytes, and joint incongruity, not solely soft tissue contracture. Capsular release will not restore motion and may exacerbate pain. |
| Absolute | Unstable Proximal Humerus Fracture | Aggressive manipulation and release can displace fracture fragments or hardware. |
| Relative | Early "Freezing" Stage of Adhesive Capsulitis | Intense synovitis and inflammation; surgery may trigger a massive inflammatory flare. Better managed with intra-articular corticosteroids and gentle therapy. |
| Relative | Poor Patient Compliance | Postoperative rehabilitation is grueling and painful. Patients unwilling or unable to participate in aggressive daily PT will predictably fail and re-stiffen. |
| Relative | Uncontrolled Diabetes Mellitus | High risk of recurrent stiffness, poor wound healing, and infection. Glycemic control should be optimized prior to elective release. |
Careful patient selection is the cornerstone of a successful outcome. Operating on a patient in the early, highly inflammatory freezing stage is generally discouraged, as the surgical trauma can exacerbate the cytokine cascade, leading to a severe postoperative flare and recurrent, intractable stiffness. Furthermore, patients with a low pain tolerance or those who demonstrate a lack of commitment to the mandatory, intensive postoperative rehabilitation protocol are poor candidates. The surgeon must have a frank discussion with the patient, emphasizing that the surgery merely "unlocks" the joint, but the patient's dedication to physical therapy is what maintains the newly acquired motion.
Pre-Operative Planning, Templating, and Patient Positioning
Diagnostic Imaging and Templating Considerations
While the diagnosis of adhesive capsulitis is primarily clinical, a meticulous radiographic evaluation is mandatory to rule out underlying osseous pathology that would preclude a soft-tissue capsular release. Routine radiographic evaluation must include a true anteroposterior (AP) view of the glenohumeral joint (Grashey view) in neutral, internal, and external rotation, as well as a scapular-Y and an axillary lateral view. The axillary view is particularly critical for identifying subtle posterior subluxations, joint space narrowing, or large inferior humeral osteophytes that physically block motion.
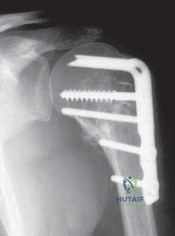
In patients with primary adhesive capsulitis, radiographs are typically normal, though profound disuse osteopenia is frequently noted due to prolonged limb immobilization. In cases of secondary stiffness, concomitant findings may include mild osteoarthrosis, calcific tendinitis, or retained hardware signifying a previous surgical procedure. The presence of hardware (e.g., a blade plate or locking plate for a proximal humerus fracture) is a critical preoperative finding, as it alerts the surgeon to expect dense, unyielding adhesions in the subdeltoid and subacromial spaces, necessitating a planned, extensive extra-articular adhesiolysis.


Advanced imaging, such as Magnetic Resonance Imaging (MRI), is not routinely required to confirm the diagnosis of adhesive capsulitis. However, an MRI is highly indicated if a concomitant rotator cuff tear, labral pathology, or other soft tissue derangement is clinically suspected. In classic frozen shoulder, MRI often demonstrates a thickened coracohumeral ligament, soft tissue obliteration of the rotator interval fat triangle, and a thickened inferior glenohumeral ligament capsule (frequently >4 mm) with reduced axillary pouch volume. We do not typically order an arthrogram or laboratory studies to confirm the diagnosis, unless there is a clinical suspicion of an inflammatory arthropathy or infection.
Anesthesia, Nerve Blocks, and Examination Under Anesthesia
The anesthetic plan is a critical component of the overall surgical strategy. A general anesthetic is typically employed to ensure complete muscle relaxation, which is essential for both the Examination Under Anesthesia (EUA) and the subsequent arthroscopic release. Additionally, a preoperative interscalene regional nerve block is strongly recommended. The block provides profound preemptive analgesia, reduces intraoperative volatile anesthetic requirements, and, most importantly, facilitates immediate, pain-free passive range of motion in the recovery room, which is vital for preventing the early recurrence of adhesions.
Once the patient is anesthetized and fully relaxed, a rigorous Examination Under Anesthesia must be performed and meticulously documented. The surgeon systematically assesses forward elevation, abduction, and internal/external rotation at varying degrees of abduction. The EUA serves two primary purposes: first, it confirms the diagnosis of true capsular contracture (as opposed to conscious muscle guarding); second, it establishes a baseline of restricted motion against which the success of the intraoperative release can be immediately judged.


Historically, closed manipulation under anesthesia (MUA) was the primary treatment for frozen shoulder. However, aggressive closed manipulation carries significant risks, including iatrogenic proximal humerus fractures, labral tears, and rotator cuff avulsions. While a very gentle manipulation can be performed to rupture some of the thinner adhesions and facilitate initial arthroscope insertion, forceful, uncontrolled manipulation is discouraged. The modern gold standard is a controlled, visually directed arthroscopic capsular release, which allows for precise division of the contracted tissues without subjecting the joint to dangerous torsional forces.
Patient Positioning and Operating Room Setup
Arthroscopic capsular release can be performed with the patient in either the beach-chair or the lateral decubitus position, largely depending on the surgeon's preference and training. The beach-chair position offers several distinct advantages for this specific procedure. It allows for a more anatomic orientation, facilitating the transition between intra-articular and subacromial work. More importantly, it permits the surgeon to freely manipulate the arm through a full, unencumbered range of motion intraoperatively, allowing for real-time assessment of the capsular release's efficacy.
If the beach-chair position is selected, the patient's head must be securely stabilized, and the non-operative arm padded and protected. The operative arm is typically placed in a hydraulic or mechanical arm holder, which assists in maintaining specific degrees of abduction and rotation during the release. Care must be taken to ensure the posterior shoulder is brought far enough off the edge of the table to allow unobstructed access for the posterior portal.


Alternatively, the lateral decubitus position provides excellent joint distraction and visualization, particularly of the inferior capsule and axillary pouch. The arm is suspended with 10 to 15 pounds of longitudinal traction. However, assessing true, dynamic range of motion during the procedure is slightly more cumbersome in the lateral position. Regardless of the position chosen, standard arthroscopic equipment is utilized, including a 30-degree arthroscope, dedicated arthroscopic scissors, basket punches, and radiofrequency ablation wands. A fluid management system with a pump is essential to maintain joint distension, control bleeding from the hyperemic synovium, and ensure clear visualization throughout the meticulous release.
Step-by-Step Surgical Approach and Fixation Technique
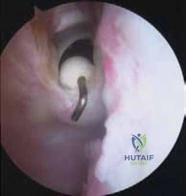
Portal Placement and Diagnostic Arthroscopy
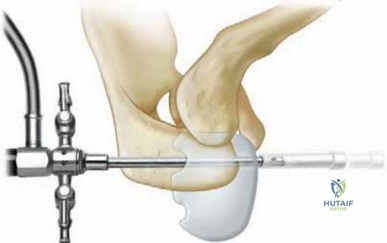
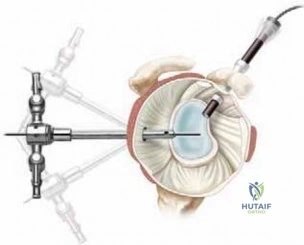
The surgical approach begins with the establishment of the standard posterior viewing portal. In a severely contracted shoulder, joint entry can be challenging due to the obliterated joint space. The surgeon must rely on precise anatomic landmarks—typically 2 cm inferior and 1 cm medial to the posterolateral corner of the acromion. A blunt trocar is used to carefully enter the joint, aiming toward the coracoid process, to avoid iatrogenic scuffing of the articular cartilage. Once intra-articular placement is confirmed, the joint is distended with saline.
An anterior portal is then established under direct intra-articular visualization using an outside-in spinal needle localization technique. The anterior portal is typically placed in the rotator interval, just superior to the subscapularis tendon and lateral to the middle glenohumeral
Clinical & Radiographic Imaging Archive




