Adolescent Blount's Disease: Proximal Tibial Osteotomy with External Fixation – An Intraoperative Masterclass
Key Takeaway
This masterclass guides fellows through the surgical management of adolescent Blount's disease. We cover comprehensive preoperative planning, meticulous patient positioning, and the step-by-step intraoperative execution of a proximal tibial osteotomy with the EBI Multi-Axial Correction System. Emphasis is placed on detailed surgical anatomy, neurovascular protection, precise instrument use, and critical pearls for avoiding complications, ensuring optimal outcomes for patients with progressive tibia vara.
Comprehensive Introduction and Patho-Epidemiology
Adolescent Blount’s disease, historically termed late-onset idiopathic tibia vara or osteochondritis deformans tibiae, represents a profound disruption in the normal endochondral ossification of the proximal tibial physis. Unlike its infantile counterpart, which manifests in toddlers, the adolescent variant presents in patients aged eleven years and older, carrying with it a distinct set of biomechanical and demographic challenges. The fundamental pathology is rooted in the Hueter-Volkmann principle: excessive, repetitive compressive forces acting across the medial aspect of the proximal tibial physis inhibit normal chondrocyte proliferation and hypertrophy. This localized growth arrest leads to a progressive, multi-planar deformity characterized predominantly by varus angulation, often accompanied by internal tibial torsion and procurvatum or recurvatum.
The epidemiological profile of adolescent Blount’s disease is highly specific. It overwhelmingly affects African American males and is intrinsically linked to morbid obesity. The mechanical burden of excessive adipose tissue, combined with a potentially inherent genetic predisposition to physeal vulnerability, creates a perfect storm for mechanical failure of the medial growth plate. Unlike infantile cases where the chief complaint is visually alarming bowing of the lower extremities, the adolescent patient frequently presents with insidious, progressive medial joint line knee pain. This pain is a direct consequence of the mechanical axis shifting medially, drastically increasing the contact pressures within the medial compartment of the knee and setting the stage for premature, aggressive degenerative osteoarthritis if left untreated.
Histopathologically, the medial proximal tibial physis in these patients demonstrates chaotic architecture. Biopsy specimens typically reveal clefts within the physis, islands of densely packed fibrocartilage, and a complete loss of the normal columnar arrangement of chondrocytes. The zone of hypertrophy is often severely truncated or entirely absent, replaced by disorganized fibrous tissue that fails to undergo normal provisional calcification and subsequent ossification. This localized biological failure necessitates a robust surgical strategy, as the remaining open physis lacks the regenerative capacity to correct the deformity spontaneously or respond adequately to simple offloading braces.
Approximately fifty percent of adolescent Blount’s disease cases present bilaterally, though often with varying degrees of severity between the limbs. The deformity is not always confined strictly to the proximal tibia; compensatory or primary deformities may also exist in the distal femur, complicating the clinical picture. Our primary surgical objective is unambiguous: we must meticulously restore the normal anatomic orientation of the knee and ankle joints, re-establishing a physiological mechanical axis. In the adolescent population, where remaining growth potential is limited and the limbs are subjected to massive biomechanical loads, proximal tibial osteotomy combined with robust external fixation remains the gold standard for achieving precise, multi-planar correction.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy and the altered biomechanics of the lower extremity is non-negotiable when approaching adolescent Blount’s disease. The proximal tibia is a complex, three-dimensional structure. In the setting of Blount’s, the medial plateau is often depressed, and the physis assumes a serpiginous, irregular contour. The medial metaphyseal beak, a hallmark of the infantile form, may be less pronounced in adolescents, but the structural integrity of the medial cortical bone is often compromised. We must navigate this distorted anatomy while strictly respecting the critical neurovascular structures that traverse the region.
Biomechanically, the normal lower limb alignment places the mechanical axis—a line drawn from the center of the femoral head to the center of the ankle plafond—slightly medial to the center of the knee joint. In adolescent Blount’s disease, this axis is violently shifted medially, resulting in a severe Mechanical Axis Deviation (MAD). This deviation exponentially increases the adduction moment at the knee during the stance phase of gait. The medial collateral ligament and medial meniscus are subjected to chronic, pathological tension and shear forces, respectively, while the lateral collateral ligament may become attenuated due to chronic stretching. This altered kinematic chain often manifests clinically as a lateral thrust during gait, a dynamic sign of catastrophic medial compartment overload and lateral ligamentous incompetence.
The neurovascular anatomy dictates our surgical approach and pin placement strategy. The common peroneal nerve is the structure at highest risk during correction. It courses distally and laterally from the popliteal fossa, winding around the fibular neck before diving beneath the peroneus longus muscle and bifurcating into the deep and superficial branches. Any valgus-producing osteotomy of the proximal tibia, particularly when combined with fibular osteotomy and acute correction, places immense traction on this nerve. Similarly, the anterior tibial artery, which branches from the popliteal artery and passes anteriorly through the proximal hiatus of the interosseous membrane, is highly vulnerable during proximal tibial osteotomies and the insertion of transfixing wires or half-pins in the proximal segment.
Furthermore, we must consider the multi-planar nature of the deformity. While varus is the dominant feature, sagittal and axial plane deformities frequently co-exist. Adolescent patients often present with a component of procurvatum (anterior bowing) or, less commonly, recurvatum. Internal tibial torsion, though less severe than in infantile cases, must be assessed. The external fixator system chosen must possess the biomechanical versatility to address these multi-planar deviations simultaneously. The use of a hexapod circular frame or a multi-axial unilateral system (such as the EBI MAC) allows for the precise, computer-assisted or mathematically derived manipulation of the bone segments in all six degrees of freedom, ensuring a truly anatomic restoration of the mechanical axis.
Exhaustive Indications and Contraindications
The decision to proceed with a proximal tibial osteotomy and external fixation in an adolescent with Blount’s disease is based on a careful calculus of the patient's remaining growth, the severity of the deformity, and the presence of symptoms. Conservative management, including bracing and observation, is universally ineffective in the adolescent population due to the magnitude of the mechanical forces and the advanced state of physeal dysfunction. Therefore, surgical intervention is the definitive standard of care.
The primary indication for osteotomy is a symptomatic varus deformity with significant mechanical axis deviation in a patient with insufficient remaining growth to achieve correction via hemiepiphysiodesis (guided growth). While tension-band plating (guided growth) has revolutionized the treatment of angular deformities in younger children, it relies on a healthy, active physis. In the adolescent Blount's patient, the medial physis is often irreversibly damaged, and the patient may be approaching skeletal maturity, rendering guided growth futile. Furthermore, osteotomy allows for the simultaneous correction of co-existing leg-length discrepancies, a common finding in unilateral or asymmetrical bilateral cases, which guided growth cannot address.
External fixation is specifically indicated over internal fixation (plates and screws) in this demographic for several compelling reasons. The massive soft tissue envelope associated with morbid obesity makes the surgical exposure required for large, load-bearing plates highly morbid, increasing the risk of wound dehiscence and deep infection. Internal fixation also lacks the capacity for postoperative adjustability; if the intraoperative correction is imperfect, the patient is committed to that alignment. External fixation, conversely, allows for gradual, precise correction of complex, multi-planar deformities, simultaneous lengthening, and immediate postoperative weight-bearing, which is crucial for bone healing and the prevention of disuse osteopenia.
Contraindications, while relatively few, must be strictly respected. Active local or systemic infection is an absolute contraindication to osteotomy and hardware placement. Severe psychiatric disorders or a documented history of profound non-compliance are strong relative contraindications, as the success of external fixation relies heavily on the patient's and family's ability to perform meticulous daily pin site care and adhere to a strict distraction schedule.
| Category | Indications for PTO with External Fixation | Contraindications |
|---|---|---|
| Clinical | Symptomatic medial knee pain; Lateral thrust during gait | Active systemic or local infection |
| Radiographic | Severe MAD; Multi-planar deformity (varus + torsion + procurvatum) | Open, healthy physis with >2 years growth remaining (favor guided growth) |
| Patient Factors | Morbid obesity precluding safe internal fixation; Leg-length discrepancy >2cm | Severe non-compliance; Uncontrolled psychiatric illness |
| Surgical | Need for postoperative adjustability; Need for simultaneous lengthening | Inadequate bone stock for pin purchase (rare in adolescents) |
Pre-Operative Planning, Templating, and Patient Positioning
The success of a complex deformity correction is dictated entirely by the rigor of the preoperative planning. Our surgical journey begins long before the patient enters the operating theater. The cornerstone of this process is the acquisition of pristine, standardized radiographic imaging. We require 51-inch, weight-bearing, anteroposterior (AP) long-leg radiographs. It is a critical, non-negotiable rule that the patella—not the foot—must be pointing directly forward (patella forward view). In patients with significant tibial torsion, the feet may need to be internally or externally rotated to achieve this. If the patella is not centralized, rotational artifact will severely distort our angular measurements in the coronal plane, leading to catastrophic miscalculations.
Once accurate radiographs are obtained, we perform a systematic deformity analysis based on the principles elucidated by Paley. We first quantify the overall Mechanical Axis Deviation (MAD). Next, we localize the source of the deformity by measuring the joint orientation angles: the mechanical Lateral Distal Femoral Angle (mLDFA) and the Medial Proximal Tibial Angle (MPTA). Normal mLDFA and MPTA values range from 85 to 90 degrees. In adolescent Blount's, the MPTA is drastically reduced, confirming the proximal tibia as the primary site of pathology. We also assess the Joint Line Convergence Angle (JLCA) to rule out intra-articular ligamentous laxity contributing to the varus thrust.

The most critical step in templating is identifying the Center of Rotation of Angulation (CORA). Because the deformity in Blount's disease is juxta-articular, we cannot simply draw two diaphyseal lines. We must extend the mechanical axis of the proximal segment (often derived by extending the femoral mechanical axis if the mLDFA is normal) and intersect it with the mechanical axis of the distal tibial segment. The intersection defines the CORA. We then plan our osteotomy rule and hinge placement. Placing the fixator hinge directly over the CORA (CORA-centric) allows for pure angular correction without translation. If simultaneous lengthening is required, we place the hinge on the convex side of the deformity along the bisector line (CORA-perpendicular).
In the operating room, meticulous patient positioning sets the stage for a smooth procedure. The patient is placed supine on a fully radiolucent table, preferably an OSI table with a Jackson imaging top, allowing completely unimpeded C-arm fluoroscopy from the hip to the ankle. A small bump is placed under the ipsilateral buttock to internally rotate the limb slightly, neutralizing the natural tendency for external rotation and ensuring the patella faces the ceiling. We strictly avoid the use of a tourniquet. The massive thigh circumference in these obese adolescents renders tourniquets ineffective and highly dangerous, risking severe crush injury to the soft tissues and neurovascular structures. The entire limb is prepped and draped free, crucially leaving the toes exposed to monitor for any motor twitching during pin placement, a vital real-time check against peroneal nerve irritation.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution is a highly orchestrated sequence of procedures, demanding absolute precision and an intimate knowledge of cross-sectional anatomy. We divide the operation into fibular osteotomy, prophylactic fasciotomies, external fixator application, and the proximal tibial osteotomy.
The Fibular Osteotomy and Fasciotomies
The fibula must be osteotomized; failure to do so creates a lateral tether that will relentlessly resist valgus correction, leading to incomplete correction, premature consolidation, or catastrophic proximal fibular migration.

I begin with a 5-7 cm longitudinal incision over the lateral aspect of the fibula, at the junction of the middle and distal thirds. This distal location deliberately separates the fibular osteotomy from the proximal tibial osteotomy, minimizing the risk of a cross-union. Dissection is carried down to the deep fascia. At this juncture, we perform a prophylactic subcutaneous lateral compartment fasciotomy.
SURGICAL WARNING: The superficial peroneal nerve exits the deep fascia in this exact vicinity. It must be visually identified and meticulously protected using blunt retractors.

We identify the interval between the peroneus longus and brevis, retracting them to expose the fibular periosteum. A subperiosteal dissection is performed using a Cobb elevator. We place Hohmann retractors circumferentially around the fibula to protect the peroneal artery lying immediately medial. Using an oscillating saw with copious saline irrigation to prevent thermal necrosis, a 1-cm oblique segment of the fibula is resected.

Proximal Tibial Exposure and Pin Placement
Attention is then turned to the proximal tibia. A 5 cm longitudinal incision is made just lateral to the tibial crest, centered over the planned osteotomy site (typically just distal to the tibial tubercle to avoid the patellar tendon insertion). We perform a prophylactic anterior compartment fasciotomy through this incision, as the massive soft tissue swelling inherent to this surgery in obese patients carries a high risk of compartment syndrome.


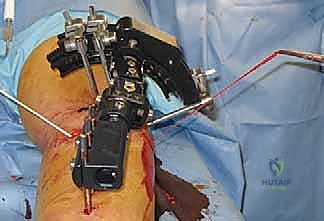
Before completing the tibial osteotomy, we apply the external fixator to maintain control of the bone segments. For the EBI Multi-Axial Correction (MAC) system or a hexapod frame, pin placement must be biologically sound and mechanically rigid. We utilize hydroxyapatite-coated half-pins to maximize the bone-pin interface and reduce the risk of aseptic loosening.


In the proximal segment, pins are placed from anterior to posterior and anteromedial to posterolateral, strictly avoiding the intra-articular space and the posterolateral neurovascular bundle. We pre-drill all pin tracts using a sharp drill bit and a tissue-protecting sleeve, clearing the drill flutes frequently to prevent thermal injury to the bone, which is the leading cause of pin tract osteomyelitis. Bicortical purchase is mandatory for every pin. The distal segment is similarly instrumented, ensuring the pins are spread far apart to maximize the mechanical working length and stability of the frame.

The Proximal Tibial Osteotomy
Once the fixator is provisionally applied and alignment checked fluoroscopically, we proceed with the tibial osteotomy. The periosteum is incised longitudinally and elevated medially and laterally. We pass a curved Crego or right-angle clamp extra-periosteally around the posterior aspect of the tibia, staying directly on the bone to protect the popliteal artery and tibial nerve.


We utilize a multiple drill-hole technique followed by an osteotome, or alternatively, a Gigli saw, to perform a low-energy, corticotomy-style osteotomy. This preserves the endosteal blood supply and the osteogenic potential of the marrow elements.


Once the bone is completely divided, the osteotomy is mobilized. We confirm complete freedom of the segments. Depending on the preoperative plan and the tension on the soft tissues, we may perform an acute correction on the table, locking the fixator into the neutral anatomical position, or we may leave the frame in the deformed position to begin gradual distraction osteogenesis postoperatively.

Finally, the wounds are copiously irrigated and closed in layers without tension. Sterile dressings and compressive sponges are applied around the pin sites to minimize skin tethering and hematoma formation.
Complications, Incidence Rates, and Salvage Management
The surgical management of adolescent Blount’s disease is fraught with potential complications, largely driven by the extreme biomechanical forces and the patient's body habitus. A proactive, highly vigilant approach is required to mitigate these risks.
Pin tract infection is the most ubiquitous complication, occurring to some degree in nearly 80% of patients undergoing external fixation. These are classified using the Checketts-MacKenzie system. The vast majority are superficial (Grades 1-2) and respond rapidly to local wound care and oral antibiotics (typically targeting Staphylococcus aureus). Deep infections (Grades 3-6) involving the bone or causing pin loosening require immediate return to the operating room for pin removal, debridement, and potentially the placement of a new pin in a different location to salvage the frame's stability.
Neurologic injury, specifically to the common peroneal nerve, is a catastrophic complication that must be avoided at all costs. The incidence ranges from 3% to 10% in large series. It is most commonly a traction neuropraxia resulting from acute valgus correction and simultaneous lengthening. If a patient develops a post-operative foot drop or paresthesia in the first web space, the correction must be immediately reversed (the "back-off" protocol) until symptoms resolve. If gradual correction is being utilized, the rate of distraction is halted or reversed. Prophylactic peroneal nerve decompression at the fibular neck is advocated by some surgeons in extreme deformities, though it is not universally practiced.
Delayed union or nonunion of the tibial osteotomy site is elevated in this population due to the inherent metabolic challenges of obesity and the large gap created by the correction. If the regenerate bone fails to consolidate within the expected timeframe (typically 1 month per centimeter of correction, plus 1-2 months for consolidation), intervention is required. This may involve "accordion" maneuvers (alternating compression and distraction of the frame to stimulate osteogenesis), percutaneous drilling of the nonunion site, or the application of autologous bone graft or orthobiologics (e.g., BMP-2, bone marrow aspirate concentrate).
| Complication | Estimated Incidence | Prevention & Salvage Management |
|---|---|---|
| Pin Tract Infection | 60% - 80% | Prevention: Hydroxyapatite pins, pre-drilling, meticulous daily cleaning. Salvage: Oral antibiotics; IV antibiotics and pin exchange for deep osteomyelitis. |
| Peroneal Nerve Palsy | 3% - 10% | Prevention: Avoid acute extreme valgus, prophylactic fasciotomy. Salvage: Immediate reversal of correction; surgical decompression if unresponsive. |
| Delayed Union / Nonunion | 5% - 15% | Prevention: Low-energy corticotomy, rigid frame construct, early weight-bearing. Salvage: Accordion maneuver, autologous bone grafting, orthobiologics. |
| Compartment Syndrome | < 2% | Prevention: Prophylactic anterior and lateral fasciotomies intraoperatively. Salvage: Emergent 4-compartment fasciotomy. |
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation protocol is as critical to the final outcome as the surgical execution itself. The protocol is divided into distinct phases: the latency phase, the distraction/correction phase, and the consolidation phase.
The latency phase encompasses the first 7 to 10 days post-operatively. During this period, no correction or lengthening is performed. The focus is entirely on acute pain management, aggressive deep vein thrombosis (DVT) prophylaxis (mandatory in these obese adolescents), and the initiation of meticulous pin site care. We utilize a protocol of daily cleansing with half-strength hydrogen peroxide or chlorhexidine, followed by the application of sterile gauze. Early mobilization is encouraged, and patients are typically allowed touch-down weight-bearing with crutches or a walker.
If gradual correction is planned, the distraction phase begins after the latency period. The patient and their family are instructed to adjust the struts or hinges of the external fixator according to a highly specific, computer-generated prescription. The standard rate is 1 millimeter per day, divided into four increments (0.25 mm every 6 hours). During this phase, intensive physical therapy is paramount. The physical therapist must aggressively work on maintaining knee and ankle range of motion, as the distraction forces will naturally cause the muscles and tendons to tighten, risking knee flexion contractures and equinus deformities of the ankle. Splinting of the foot in a neutral position at night is strongly recommended.
Once the desired anatomical alignment and length are achieved, the frame is locked, and the patient enters the consolidation phase. The regenerate bone must mature and corticate before the frame can be safely removed. This phase often takes twice as long as the distraction phase. We encourage progressive, full weight-bearing during this time, as the axial loading stimulates osteoblastic activity and accelerates corticalization according to Wolff's Law. Serial radiographs are obtained every 3-4 weeks to assess the healing of three out of four cortices. Once sufficient consolidation is confirmed, the frame is removed under brief sedation. Post-removal, the limb is protected in a hinged knee brace or a short leg cast for an additional 4 to 6 weeks to prevent catastrophic fracture through the pin sites or the immature regenerate bone.
Summary of Landmark Literature and Clinical Guidelines
The evolution of our understanding and surgical management of adolescent Blount's disease is built upon a foundation of landmark orthopedic literature. Langenskiöld's original classifications, while initially focused on the infantile form, provided the fundamental morphological framework for understanding physeal depression and medial metaphyseal beaking. Subsequent modifications by authors such as Thompson and Carter helped delineate the distinct clinical entity of the adolescent, late-onset variant, emphasizing its unique association with massive obesity and the absence of spontaneous resolution.
The modern era of multi-planar deformity correction was ushered in by the seminal work of Dror Paley and his comprehensive principles of deformity analysis. Paley's codification of the Mechanical Axis Deviation (MAD) and the precise mathematical determination of the Center of Rotation of Angulation (CORA) transformed osteotomy from an art based on visual estimation into an exact science. His guidelines mandate that any corrective osteotomy must respect the CORA to avoid iatrogenic translation, a principle that dictates our use of sophisticated external fixators in these complex cases.
Recent comparative literature heavily favors external fixation over internal plating in the morbidly obese adolescent population. Studies by Gordon et al. and Feldman et al. have demonstrated that while internal fixation with locking plates can achieve acute correction, the complication rates
