Open Fixation for Scapular Fractures: What You Need to Know
Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Open Fixation for Scapular Fractures: What You Need to Know. "Scapular fractures open" refers to a scapular bone break accompanied by an open wound, where the bone has penetrated the skin. These are typically high-energy trauma injuries. A thorough soft tissue examination is crucial, as such wounds indicate an open fracture and necessitate exploration, distinguishing them from most nonarticular scapular fractures treated nonoperatively.
Introduction and Epidemiology
Scapular fractures represent a relatively uncommon but highly significant orthopedic injury, accounting for approximately 1% of all fractures and 3% to 5% of all shoulder girdle injuries. Nonarticular scapular fractures encompass fractures of the glenoid neck, scapular spine and body, acromial process, and coracoid process. These extra-articular patterns account for the vast majority—up to 90%—of all scapular fractures.
Because the scapula is heavily protected by a robust muscular envelope and its natural mobility on the thoracic wall allows for energy dissipation, scapular fractures typically result from high-energy blunt trauma. Motor vehicle collisions, motorcycle accidents, and high-velocity falls are the most common mechanisms of injury. Consequently, the presence of a scapular fracture is a well-established marker for severe concomitant injuries. Up to 80% to 90% of patients present with associated trauma, including ipsilateral rib fractures, pulmonary contusions, pneumothorax, closed head injuries, spinal trauma, and brachial plexus injuries. The high incidence of these associated life-threatening injuries often dictates the initial trauma resuscitation priorities, occasionally delaying the definitive diagnosis and management of the scapular fracture itself.

While the natural history of nonoperative treatment for nonarticular scapular fractures is generally favorable due to the rich vascular supply and the compensatory motion of the glenohumeral and scapulothoracic joints, significant displacement can lead to chronic pain, weakness, and altered shoulder biomechanics. Scapulothoracic dyskinesia, impingement syndromes, and early fatigue of the rotator cuff are documented sequelae of malunited scapular fractures. Therefore, modern orthopedic traumatology has seen a paradigm shift toward open reduction and internal fixation (ORIF) for highly displaced extra-articular fractures, particularly those involving disruption of the superior shoulder suspensory complex.
Surgical Anatomy and Biomechanics
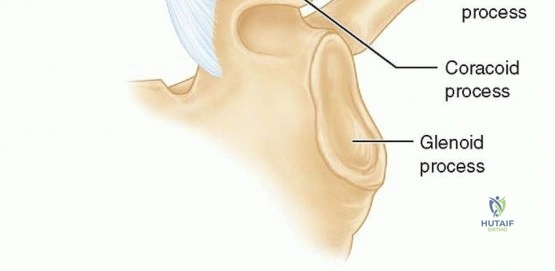
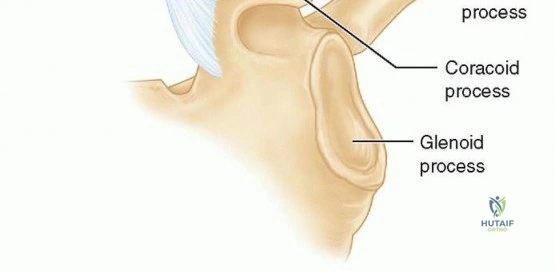
A profound understanding of scapular osteology, muscular attachments, and neurovascular relations is mandatory for safe surgical intervention. The scapula is a flat, triangular bone that serves as the foundational platform for the upper extremity. It features three distinct processes laterally: the glenoid process, the acromial process, and the coracoid process. The glenoid process is further subdivided into the glenoid fossa, the glenoid rim, and the glenoid neck.
Superior Shoulder Suspensory Complex
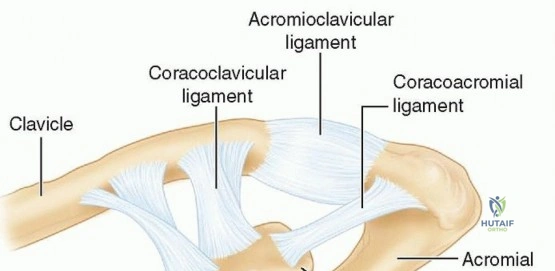
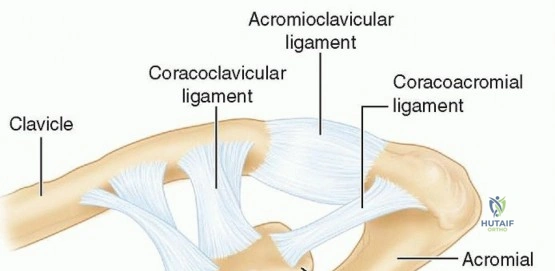
The biomechanical cornerstone of the shoulder girdle is the Superior Shoulder Suspensory Complex (SSSC), originally described by Goss. The SSSC is a continuous bone and soft-tissue ring positioned at the end of a superior and an inferior bony strut.
The ring itself is composed of:
* The glenoid process
* The coracoid process
* The coracoclavicular ligaments
* The distal clavicle
* The acromioclavicular joint
* The acromial process
The struts supporting this ring are:
* Superior Strut: The middle third of the clavicle.
* Inferior Strut: The junction of the most lateral portion of the scapular body and the most medial portion of the glenoid neck.
Single disruptions of the SSSC (e.g., an isolated nondisplaced scapular body fracture) are biomechanically stable and heal predictably with nonoperative management. Double disruptions (e.g., a displaced glenoid neck fracture combined with an ipsilateral clavicle fracture, historically termed a "floating shoulder") create an unstable biomechanical environment. The weight of the arm and the pull of the regional musculature displace the glenohumeral joint inferiorly and medially, often necessitating surgical stabilization of one or both lesions to restore the functional integrity of the suspensory complex.
Neurovascular Considerations
The surgical approaches to the scapula are fraught with neurovascular hazards. The suprascapular nerve and artery course through the suprascapular notch (medial to the coracoid base) and travel posteriorly to innervate the supraspinatus. The nerve then winds around the base of the scapular spine through the spinoglenoid notch to innervate the infraspinatus. The suprascapular nerve lies approximately 1.5 to 2.0 cm medial to the posterior glenoid rim; hardware placement or aggressive medial retraction in this zone risks iatrogenic denervation of the infraspinatus.
The axillary nerve and the posterior humeral circumflex artery exit the axilla through the quadrangular space, coursing in close proximity to the inferior glenoid neck and the lateral border of the scapula. Dissection along the lateral border of the scapula must respect the teres minor and the inferior capsule to avoid axillary nerve injury.
Indications and Contraindications
The majority of scapular fractures (over 90%) are historically treated nonoperatively. This includes isolated scapular body and spine fractures with minimal displacement. However, significant displacement at one or more sites, alone or in conjunction with ligamentous disruptions of the SSSC, requires rigorous evaluation for surgical intervention.
The decision to operate is multifactorial, depending on the fracture pattern, the degree of displacement, the patient's physiological age, functional demands, hand dominance, and the presence of polytrauma. A thorough neurovascular examination must be performed preoperatively; any deficits should be evaluated with angiography or electromyography as indicated. Soft tissue integrity is paramount, as severe abrasions, fracture blisters, or open wounds may delay surgical intervention or alter the chosen approach.
Operative Versus Non Operative Decision Matrix
| Parameter | Non-Operative Indications | Operative Indications |
|---|---|---|
| Glenoid Intra-articular | Step-off < 4 mm, minimal gap | Step-off > 4-5 mm, > 25% anterior involvement, > 33% posterior involvement, subluxation of humeral head |
| Glenoid Neck | Angulation < 40 degrees, translation < 1 cm | Angulation > 40 degrees (coronal/sagittal), medial translation > 1-1.5 cm |
| Scapular Body | Minimal displacement, intact lateral border | Medial/lateral translation > 20 mm, angular deformity > 45 degrees, severe lateral border step-off |
| SSSC Double Disruption | Minimal displacement, stable construct | "Floating shoulder" with > 1 cm translation, highly displaced clavicle + glenoid neck |
| Acromion / Coracoid | Nondisplaced, intact subacromial space | Displaced fractures causing subacromial impingement, symptomatic nonunions |
Contraindications
Absolute contraindications to operative fixation include medically unstable polytrauma patients who cannot tolerate prolonged anesthesia, severe traumatic brain injury where functional recovery is highly improbable, and active localized infection over the surgical site. Relative contraindications include a severely compromised soft tissue envelope (e.g., extensive Morel-Lavallée lesions or severe fracture blisters), severe osteopenia precluding secure hardware purchase, and non-ambulatory baseline status with low functional demands.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is critical due to the complex, three-dimensional anatomy of the scapula. Routine shoulder trauma series radiographs—a true anteroposterior (AP) view of the shoulder (Grashey view), a true axillary view, and a scapular Y view—are the initial standard. However, plain radiography often underestimates the degree of displacement and articular involvement due to overlapping thoracic structures.
Computed tomography (CT) with two-dimensional multiplanar reformats and three-dimensional (3D) surface-rendered reconstructions is the gold standard for preoperative planning. 3D CT allows the surgeon to conceptualize the fracture lines, identify the primary structural pillars (specifically the lateral border and the scapular spine), and template plate placement. The bony relationships must also be scrutinized for evidence of ligamentous disruption, such as acromioclavicular or coracoclavicular widening.
Patient Positioning
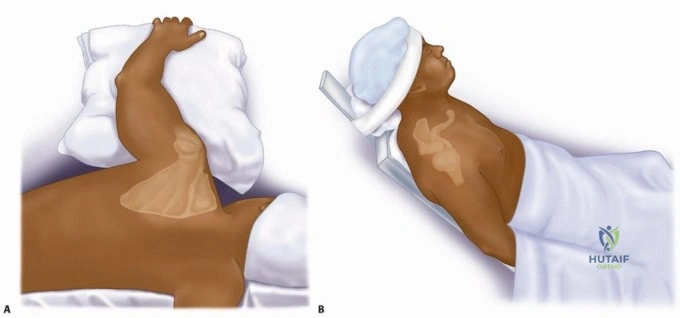
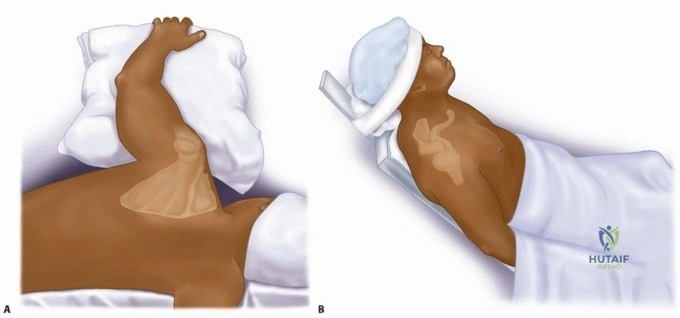
Surgical stabilization of the scapula is typically performed with the patient in either the lateral decubitus or prone position, depending on the specific fracture pattern and surgeon preference.
For the prone position, the patient is placed on a radiolucent Jackson table with chest rolls to ensure adequate pulmonary excursion. The operative arm is draped free and rested on a radiolucent arm board or Mayo stand, allowing for intraoperative manipulation. This position provides excellent bilateral access if required and simplifies orientation for the posterior approach.
Alternatively, the lateral decubitus position allows for simultaneous access to the anterior shoulder or clavicle if a combined approach is necessary for a floating shoulder. A beanbag is utilized to secure the torso, and the arm is draped free. Careful padding of all bony prominences and the axilla (axillary roll) is mandatory to prevent perioperative neuropraxia. Fluoroscopy is brought in from the contralateral side, and baseline images must be obtained prior to incision to ensure adequate visualization of the glenohumeral joint and scapular body without interference from the table or positioning devices.

Detailed Surgical Approach and Technique
The classic surgical exposure for complex scapular body and glenoid neck fractures is the Judet approach. However, the traditional Judet approach requires extensive elevation of the posterior deltoid and infraspinatus, which can lead to significant postoperative morbidity, deltoid weakness, and devascularization of the fracture fragments. Consequently, the modified Judet approach and various muscle-sparing intermuscular approaches have become the modern standard of care.
The Modified Judet Approach
The modified Judet approach provides extensive access to the posterior scapula while minimizing muscular detachment.
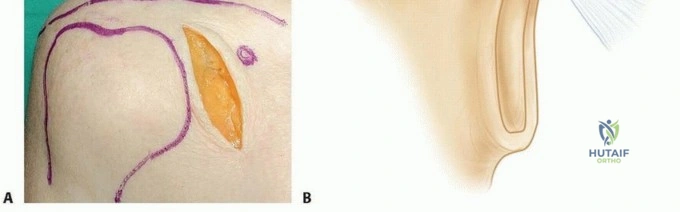
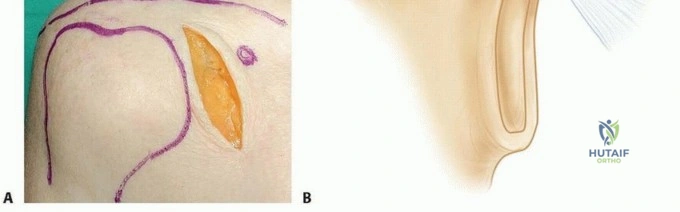
- Incision: A curvilinear or L-shaped incision is made starting at the posterolateral corner of the acromion, extending medially along the scapular spine to the medial border of the scapula, and then curving inferiorly along the medial border toward the inferior angle.
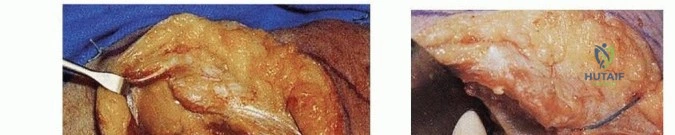
- Superficial Dissection: Thick fasciocutaneous flaps are developed to expose the underlying deep fascia overlying the deltoid, trapezius, and infraspinatus muscles.
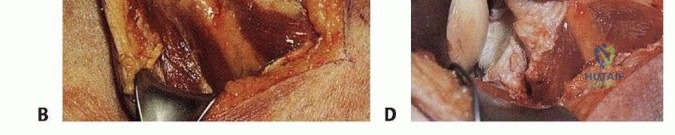
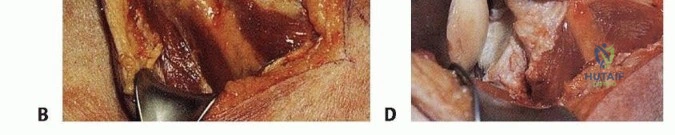
- Muscular Windows: Instead of detaching the deltoid, the surgeon utilizes internervous and intermuscular planes. The primary window for accessing the lateral border and glenoid neck is the interval between the infraspinatus (suprascapular nerve) and the teres minor (axillary nerve).
- Infraspinatus Elevation: If access to the central scapular body or medial glenoid neck is required, the infraspinatus can be elevated from medial to lateral off the scapular fossa. The muscle is retracted laterally, acting as a cushion to protect the suprascapular neurovascular bundle at the spinoglenoid notch.

Fracture Reduction Techniques
Reduction of the scapula can be exceptionally challenging due to the powerful pull of the rotator cuff and periscapular musculature.
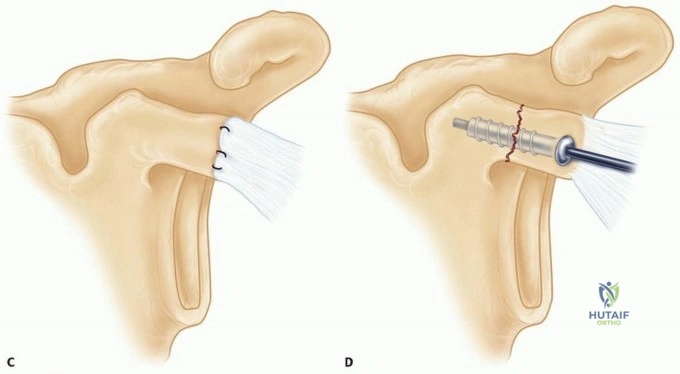
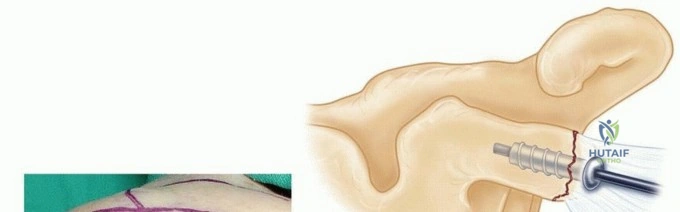
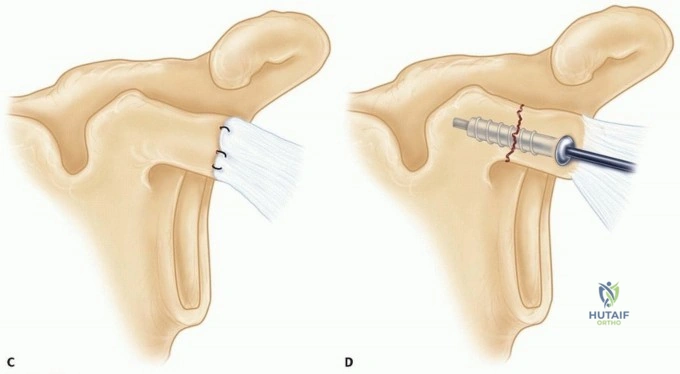
* Schanz Pins: A 4.0 mm or 5.0 mm Schanz pin can be placed into the thick bone of the glenoid neck or the posterolateral acromion to serve as a "joystick" for manipulating the articular segment.
* Direct Reduction: Pointed reduction forceps (Weber clamps) are used to provisionalize the reduction. The lateral border of the scapula (the inferior strut of the SSSC) is the thickest and most structurally sound bone of the scapular body; restoring the lateral border is the critical first step in reconstructing the scapula.
* Articular Surface: If there is an intra-articular glenoid component, this must be reduced anatomically under direct vision or fluoroscopic guidance prior to addressing the extra-articular body fractures. Subchondral lag screws (usually 2.7 mm or 3.5 mm) are utilized for articular compression.

Internal Fixation Strategy
The osteology of the scapula dictates the fixation strategy. The central body of the scapula is exceptionally thin and translucent, making it entirely unsuitable for screw purchase. Fixation must be anchored to the robust bony pillars:
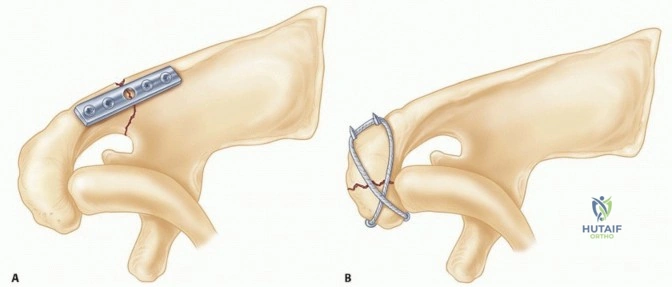
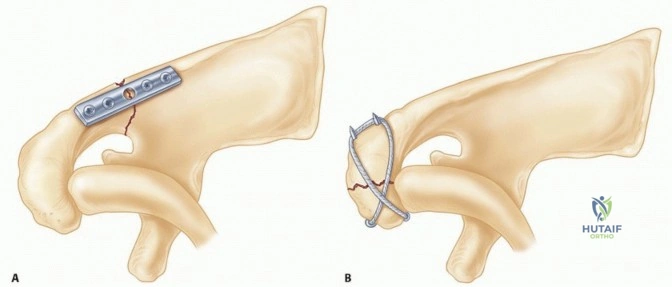
1. The Lateral Border: This is the primary column. A pre-contoured 2.7 mm or 3.5 mm reconstruction plate is applied along the lateral border, extending from the inferior angle up to the inferior glenoid neck. Locking screws may be utilized if bone quality is poor, but standard cortical screws are often sufficient for the thick lateral border.
2. The Scapular Spine: A second plate (often a 2.7 mm or 3.5 mm dynamic compression or reconstruction plate) is placed along the scapular spine to control rotation and provide superior stability.
3. The Medial Border: In severely comminuted patterns, a third, lower-profile plate (e.g., 2.4 mm or 2.7 mm) can be applied along the medial border.
Care must be taken when placing screws into the superior glenoid neck to avoid joint penetration and to protect the suprascapular nerve. Intraoperative fluoroscopy is critical to confirm that screws do not breach the glenohumeral articulation.
Wound Closure
Meticulous hemostasis is achieved. The muscular intervals are approximated loosely to prevent compartmental swelling. The thick fasciocutaneous flaps are closed in layers over a deep subfascial closed-suction drain to prevent postoperative hematoma formation, which is a known risk factor for infection and delayed wound healing.

Complications and Management
Surgical management of scapular fractures is technically demanding and carries a distinct complication profile. Proper preoperative planning and meticulous surgical technique are required to minimize these risks.
Overview of Surgical Complications
| Complication | Estimated Incidence | Etiology and Risk Factors | Management and Salvage Strategy |
|---|---|---|---|
| Suprascapular Nerve Palsy | 3% - 8% | Iatrogenic traction, hardware impingement near spinoglenoid notch, aggressive medial retraction. | Observation for neuropraxia (EMG at 6 weeks). Hardware removal if impingement is confirmed on CT. |
| Infection | 2% - 5% | Poor soft tissue envelope, hematoma formation, prolonged operative time. | Early aggressive surgical debridement, targeted intravenous antibiotics. Hardware retention if stable. |
| Hardware Prominence | 10% - 15% | Thin soft tissue coverage over the scapular spine, bulky plates. | Symptomatic hardware removal after definitive clinical and radiographic union (typically > 9-12 months). |
| Post-Traumatic Stiffness | 15% - 25% | Prolonged immobilization, capsular contracture, intra-articular adhesions. | Aggressive physical therapy. Arthroscopic capsular release for refractory cases > 6 months post-op. |
| Nonunion | < 1% | Extremely rare due to robust vascularity; associated with severe infection or massive bone loss. | Revision ORIF with autologous bone grafting (iliac crest) and optimization of biologic factors. |
Neurologic Injury Management
Neurologic compromise is arguably the most feared complication. The suprascapular nerve is particularly vulnerable during dissection of the suprascapular and spinoglenoid notches. If a postoperative deficit is noted (weakness in external rotation and abduction), immediate evaluation is required. If the surgical report indicates the nerve was protected, observation is warranted. Electromyography (EMG) and nerve conduction studies (NCS) should be obtained at 6 to 8 weeks to establish a baseline and monitor for reinnervation. Axillary nerve injury is less common with modern intermuscular approaches but can occur during inferior glenoid neck dissection.
Malunion and Scapulothoracic Dyskinesia
While nonunion is exceedingly rare due to the rich muscular blood supply, malunion is a frequent consequence of nonoperative management of highly displaced fractures. Severe medialization of the glenoid or angular deformity of the scapular body alters the resting length and tension of the rotator cuff musculature. This can lead to chronic impingement, early fatigue, and scapulothoracic dyskinesia. In severe, highly symptomatic cases of malunion, corrective osteotomy may be considered, though it is technically arduous and carries a high complication rate. This underscores the importance of appropriate initial surgical indications.

Post Operative Rehabilitation Protocols
The ultimate functional outcome following scapular fracture fixation is heavily dependent on a structured, phased rehabilitation protocol. The goals of rehabilitation are to protect the surgical fixation while preventing adhesive capsulitis and restoring dynamic periscapular stability.
Phase 1: Immediate Post Operative (Weeks 0 to 2)
The patient is placed in a standard shoulder immobilizer or sling. The primary focus is on wound healing and pain control. Gentle passive range of motion (PROM) exercises, including pendulum exercises, are initiated immediately. Active range of motion (AROM) of the elbow, wrist, and hand is encouraged to prevent distal stiffness. Active shoulder motion is strictly prohibited to protect the soft tissue repairs and early bony consolidation.
Phase 2: Early Motion (Weeks 2 to 6)
Once the surgical incisions are well-healed, the sling is gradually weaned. Active-assisted range of motion (AAROM) using pulleys and wand exercises is introduced. If a posterior approach was utilized with elevation of the infraspinatus, active external rotation against resistance must be avoided to protect the muscle repair. The goal by the end of week 6 is to achieve 90 degrees of forward elevation and 30 degrees of external rotation.
Phase 3: Active Motion and Early Strengthening (Weeks 6 to 12)
Radiographic evaluation is performed at 6 weeks to confirm the maintenance of hardware position and early callus formation. Upon radiographic confirmation of healing, full AROM is permitted in all planes. Isometric strengthening of the rotator cuff and periscapular stabilizers (rhomboids, serratus anterior, trapezius) is initiated. Scapular retraction and depression exercises are emphasized to prevent dyskinesia.
Phase 4: Advanced Strengthening and Return to Activity (Months 3 to 6)
Isotonic strengthening is progressed. Plyometric exercises and sport-specific or work-specific functional training are integrated. Return to heavy manual labor or contact sports is typically permitted between 4 and 6 months postoperatively, contingent upon symmetric strength (at least 85% of the contralateral side), full painless range of motion, and definitive radiographic union.
Summary of Key Literature and Guidelines
The evolution of scapular fracture management is deeply rooted in several foundational academic works and modern consensus guidelines.
The concept of the Superior Shoulder Suspensory Complex (SSSC), introduced by Goss in 1993, remains the biomechanical framework for understanding shoulder girdle stability. Goss's work established that double disruptions of this ring necessitate surgical stabilization to prevent late functional deficits.
The seminal
Clinical & Radiographic Imaging