Masterclass in Shoulder Instability: Anatomy, Biomechanics, and Surgical Reconstruction
Key Takeaway
The shoulder joint is inherently unstable, accounting for nearly 50% of all major joint dislocations. Recurrence rates are heavily influenced by patient age, athletic participation, and glenoid bone loss. This comprehensive guide details the functional anatomy, biomechanical stabilizers, and evidence-based surgical techniques—including sternoclavicular reconstruction and capsuloligamentous repair—essential for restoring glenohumeral stability and optimizing patient outcomes in orthopedic practice.
Comprehensive Introduction and Patho-Epidemiology
The shoulder, by virtue of its evolutionary design prioritizing extreme ranges of motion over inherent skeletal congruency, is undeniably one of the most unstable and frequently dislocated joints in the human body. This evolutionary trade-off accounts for nearly 50% of all major joint dislocations, presenting with an overall incidence of approximately 2% in the general population. The management of glenohumeral instability requires a profound, highly nuanced understanding of the biomechanical and anatomical factors that precipitate recurrent dislocations, as these variables strictly dictate both conservative and operative decision-making algorithms. The pathophysiology of instability is rarely an isolated capsular tear; rather, it is a complex cascade of osseous attrition, capsuloligamentous plastic deformation, and proprioceptive decoupling.
The probability of recurrent instability is multifactorial and heavily influenced by patient age at the time of the initial dislocation, return to contact or collision sports, inherent hyperlaxity (e.g., Ehlers-Danlos or Marfan syndromes), and the presence of significant bony defects in either the glenoid or the humeral head (Hill-Sachs lesions). Age is arguably the most critical prognosticator for recurrence following an acute primary dislocation. In landmark epidemiological studies evaluating acute dislocations, recurrence rates demonstrate a stark inverse relationship with age. For patients younger than 20 years old, recurrence develops in up to 90% of cases. For those 20 to 40 years old, recurrence occurs in approximately 60% of patients. In patients older than 40 years old, recurrence drops precipitously to only 10%, though this demographic bears a significantly higher concomitant risk of devastating rotator cuff tears and axillary nerve traction injuries.
Although high recurrence rates (up to 95%) have been historically reported in the adolescent and young adult demographic, long-term follow-up studies (averaging 25 years, such as those by Hovelius et al.) reveal a highly nuanced natural history. Approximately 50% of individuals who were younger than 20 years at the time of their initial dislocation report no significant instability problems in later adulthood, suggesting a natural stabilization or "stiffening" process over decades. However, this natural history must be weighed against the cumulative risk of progressive glenohumeral osteoarthritis (dislocation arthropathy) induced by repeated micro-trauma and shear forces on the articular cartilage during recurrent subluxation events.
The duration and position of post-reduction immobilization have been subjects of intense orthopedic debate, with contemporary evidence challenging traditional dogmas. Regarding duration, recent meta-analyses have definitively determined that there is no biomechanical, histological, or clinical benefit to conventional sling immobilization extending beyond one week for a primary anterior dislocation. Prolonged immobilization merely exacerbates muscular atrophy and joint stiffness without altering the biological healing of the Bankart lesion. Regarding positioning, immobilization in external rotation was hypothesized by Itoi and colleagues to better approximate the torn anteroinferior labrum to the glenoid rim, thereby decreasing recurrence rates by eliminating the sheer stress of the subscapularis. However, rigorous multi-center randomized controlled trials and subsequent meta-analyses have failed to prove a statistically significant benefit. While early studies noted a recurrence risk of 36% with traditional internal rotation immobilization compared to 25% with external rotation bracing, the sample sizes were underpowered, compliance with external rotation bracing was notoriously poor, and the long-term difference did not reach statistical significance.
Detailed Surgical Anatomy and Biomechanics
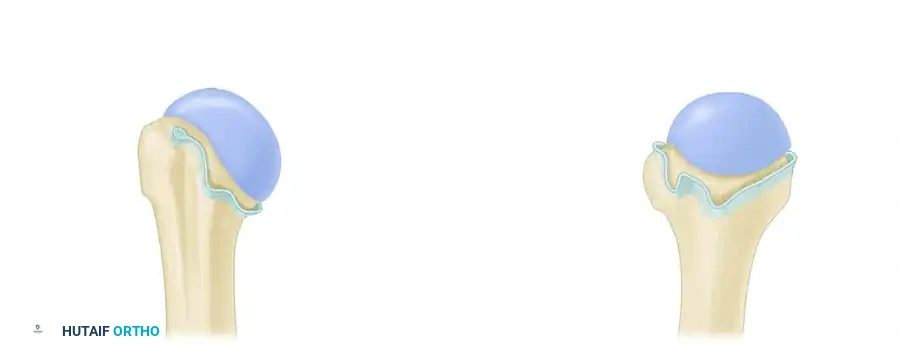
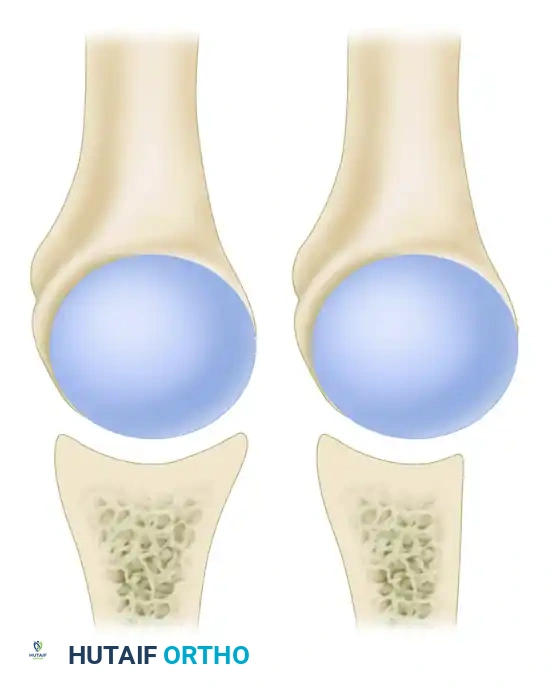
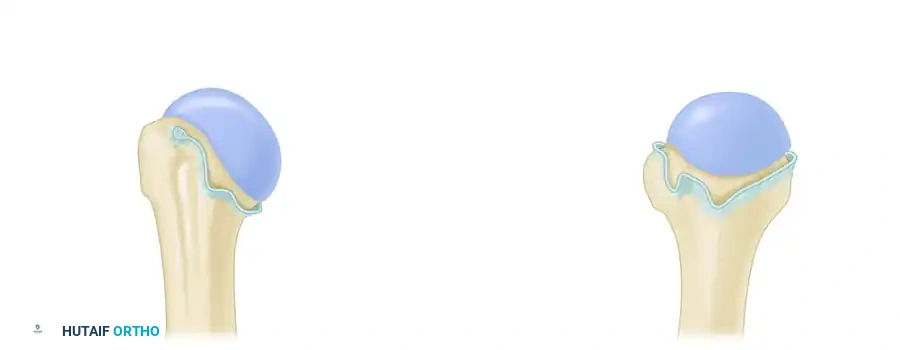
A masterful grasp of the normal functional anatomy of the shoulder is the absolute foundation upon which all stabilization procedures are built. The stability of the glenohumeral joint relies on a delicate, highly integrated interplay between static (osseous and capsuloligamentous) and dynamic (musculotendinous and proprioceptive) restraints. The bony architecture of the shoulder joint provides negligible inherent stability. The glenoid fossa is a flattened, dish-like structure, often likened to a golf tee supporting a golf ball. At any given moment, only one-fourth (25%) of the large humeral head articulates with the glenoid surface. Unlike the deep, highly congruent acetabulum of the hip, this small, flat glenoid relies heavily on soft tissue augmentation. The glenoid concavity is deepened by 50% due to the presence of the fibrocartilaginous glenoid labrum. This critical structure acts as a bumper, increasing the humeral head contact area to 75% and contributing significantly to the concavity-compression mechanism of the joint, wherein the rotator cuff dynamically compresses the humeral head into the deepened glenoid socket.
In the setting of recurrent anterior instability, repetitive trauma invariably leads to attrition, impaction, or overt fracture of the anterior glenoid rim. Pioneering work by Burkhart and DeBeer, Sugaya et al., and Itoi et al. has established critical thresholds for bone loss. They demonstrated that glenoid bone loss exceeding 20% of the inferior glenoid width (creating the classic "inverted pear" appearance) results in profound bony instability and unacceptably high recurrence rates (up to 67%) if treated with soft-tissue stabilization alone. This instability occurs because the "safe arc" of motion—the arc through which the glenoid can effectively resist axial forces and humeral rotation—is critically diminished. When the deficient anterior edge is loaded at extremes of motion (abduction and external rotation), the humeral head easily translates over the compromised rim, bypassing the concavity-compression mechanism entirely.
The shoulder joint capsule is inherently lax and thin, allowing for the joint's massive excursion. By itself, the capsule offers little resistance. However, anteriorly, the capsule is reinforced by three distinct capsular thickenings—the glenohumeral ligaments—which are intimately fused with the labral attachment to the glenoid rim. The Superior Glenohumeral Ligament (SGHL) attaches to the superior glenoid rim near the apex of the labrum, conjoined with the origin of the long head of the biceps tendon. It is the primary restraint to inferior humeral subluxation when the arm is in 0 degrees of abduction. The Middle Glenohumeral Ligament (MGHL) limits external rotation when the arm is in the lower and middle ranges of abduction (45 degrees).
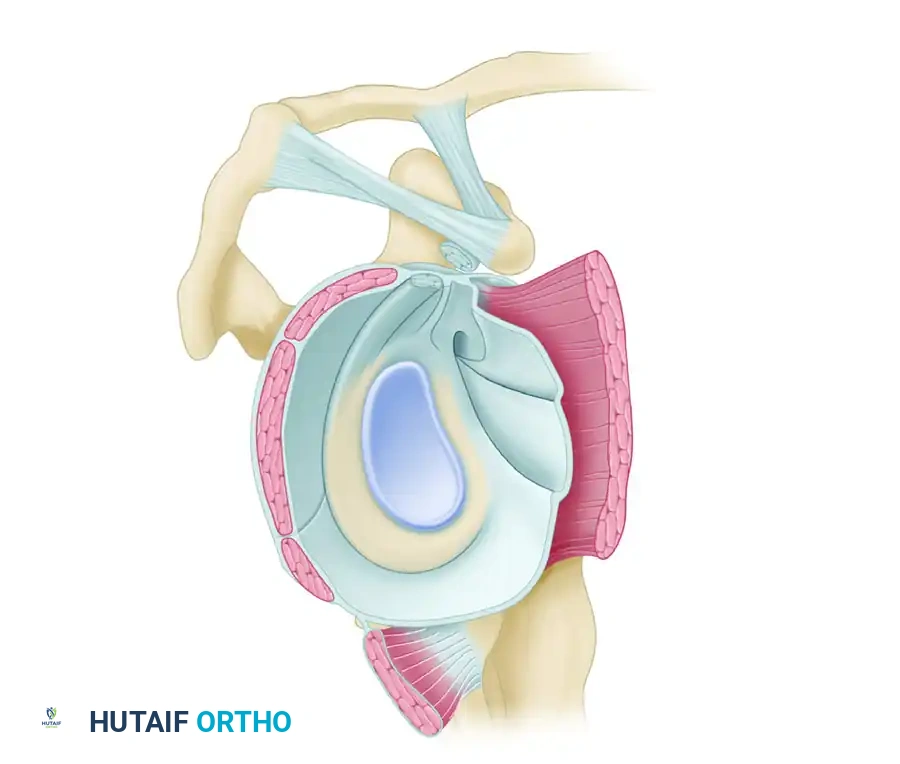
The Inferior Glenohumeral Ligament (IGHL) Complex is the most robust and critical stabilizer against anterior dislocation. It attaches to the glenoid margin from the 2- to 3-o’clock position anteriorly, extending to the 8- to 9-o’clock position posteriorly. It functions as a hammock-type sling, consisting of a thickened anterior band, a thickened posterior band, and an intervening axillary pouch. During abduction and external rotation, the anterior band tightens to prevent anterior translation. Conversely, during internal rotation, the posterior band tightens to prevent posterior subluxation.
Dynamic stabilizers are equally critical. Integral to the superior glenoid labrum is the insertion of the tendon of the long head of the biceps, which blends seamlessly into the posterior glenoid labrum. This complex serves as a dynamic "chock block," preventing excessive humeral head rollback and superior migration during sudden force application. Furthermore, the stability of the shoulder is not purely mechanical. The demonstration of Ruffini end organs and pacinian corpuscles within the shoulder capsule solidifies the concept that proprioceptive neuromuscular feedback is paramount. These mechanoreceptors trigger dynamic muscle contraction to center the humeral head. Scapulothoracic kinematics also play a vital role; scapular dyskinesis (the SICK scapula syndrome) alters the glenoid version dynamically, predisposing the joint to mechanical failure.
Exhaustive Indications and Contraindications
The decision matrix for surgical intervention in shoulder instability is complex, relying heavily on the precise quantification of bone loss, patient demographics, athletic demands, and the chronicity of the instability. The Instability Severity Index Score (ISIS) developed by Balg and Boileau remains a cornerstone in preoperative decision-making. An ISIS score of 6 or greater strongly correlates with an unacceptable failure rate for isolated arthroscopic soft-tissue repair, thereby mandating a bony augmentation procedure. Indications for an arthroscopic Bankart repair include recurrent anterior instability in a patient with a discrete capsulolabral avulsion, minimal to no glenoid bone loss (<15%), an off-track Hill-Sachs lesion that does not engage, and a failure of comprehensive non-operative rehabilitation.
Conversely, absolute indications for open or arthroscopic bony augmentation (e.g., Latarjet procedure, iliac crest bone graft, or distal tibial allograft) include critical glenoid bone loss exceeding 20% of the inferior glenoid diameter, chronic engaging Hill-Sachs lesions (bipolar bone loss), and revision scenarios where prior soft-tissue stabilization has failed. The Latarjet procedure transfers the coracoid process, along with the attached conjoined tendon, to the anteroinferior glenoid neck. This provides a triple-blocking effect: an osseous block extending the glenoid articular arc, a dynamic sling effect from the conjoined tendon tensioning the inferior subscapularis during abduction/external rotation, and a capsular repair effect via the coracoacromial ligament stump.
Sternoclavicular (SC) joint instability presents a distinct set of indications. Recurrent anterior SC joint dislocations are generally well-tolerated and should initially be treated non-operatively with periscapular strengthening. Surgery is indicated strictly for patients with severe, recalcitrant symptoms that limit activities of daily living, or for posterior SC joint dislocations that fail closed reduction and pose an imminent threat to retrosternal structures (trachea, esophagus, great vessels). Contraindications for SC joint reconstruction include asymptomatic anterior subluxation, generalized multidirectional hyperlaxity without a discrete traumatic event, and active local or systemic infection.
| Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Arthroscopic Bankart Repair | First-time dislocation in high-risk athlete; Recurrent instability with <15% glenoid bone loss; Non-engaging Hill-Sachs lesion. | Critical glenoid bone loss (>20%); Engaging Hill-Sachs lesion (without Remplissage); Active infection. | High ISIS Score (>6); Uncontrolled seizure disorder; Severe multidirectional instability (MDI) requiring massive capsular shift. |
| Latarjet Procedure (Coracoid Transfer) | Glenoid bone loss >20%; Failed prior soft-tissue repair; High-demand contact athletes (rugby, martial arts) with bipolar bone loss. | Coracoid hypoplasia/prior resection; Advanced glenohumeral osteoarthritis; Active infection. | Elderly patients with low functional demand; Severe subscapularis dysfunction or irreparable tear. |
| SC Joint Figure-of-8 Reconstruction | Symptomatic, chronic anterior SC dislocation failing conservative care; Acute/chronic posterior SC dislocation threatening mediastinal structures. | Asymptomatic anterior subluxation; Voluntary habitual dislocation; Active infection. | Poor soft-tissue envelope; Uncooperative patient incapable of adhering to strict post-op immobilization. |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning is the most critical phase in the surgical management of shoulder instability. A meticulously executed physical examination, documenting the apprehension, relocation, and surprise tests, must be corroborated with advanced imaging. Standard radiographic evaluation includes a True AP (Grashey), Scapular Y, and Axillary lateral view. The West Point axillary view is particularly useful for identifying anteroinferior glenoid rim fractures (bony Bankart lesions), while the Stryker Notch view is optimal for delineating the size and depth of a Hill-Sachs defect. However, plain radiographs are insufficient for precise surgical planning in recurrent cases.
Advanced imaging with a non-contrast Computed Tomography (CT) scan with 3D sagittal en face reconstructions is the gold standard for quantifying glenoid bone loss. The "Pico method" or the "best-fit circle" technique is utilized on the en face view of the glenoid. A circle is drawn matching the intact inferior and posterior margins of the glenoid; the missing anterior surface area is then calculated as a percentage of the total circle area. Additionally, Magnetic Resonance Imaging (MRI) or MR Arthrography is indispensable for evaluating the integrity of the capsuloligamentous complex, identifying concomitant rotator cuff pathology, and assessing the quality of the labral tissue (e.g., differentiating a classic Bankart from an ALPSA or Perthes lesion).
Patient positioning dictates the flow, safety, and ultimate success of the surgical intervention. For arthroscopic procedures, surgeons must choose between the beach-chair and lateral decubitus positions. The lateral decubitus position offers superior visualization of the anteroinferior glenoid and facilitates easier capsular plication due to longitudinal and lateral traction (typically 10-15 lbs). However, it carries risks of traction neuropraxia to the brachial plexus and requires meticulous padding of all bony prominences. The beach-chair position provides a more anatomic orientation, allows for dynamic examination of the joint under anesthesia, and permits seamless conversion to an open approach (e.g., open Latarjet) if necessary. The primary risk in the beach-chair position is cerebral hypoperfusion; thus, meticulous mean arterial pressure (MAP) monitoring by the anesthesia team is mandatory.
For Sternoclavicular (SC) joint reconstruction, the patient is placed in the beach-chair position with a bump between the scapulae to allow the shoulders to fall posteriorly, naturally reducing an anterior SC joint dislocation. A pre-operative CT angiogram of the chest is an absolute requirement for any SC joint surgery to map the exact proximity of the brachiocephalic vein, subclavian artery, and aortic arch relative to the posterior cortex of the medial clavicle and manubrium. The surgical team must ensure the immediate availability of a thoracic or vascular surgeon on standby, given the catastrophic potential of retrosternal vascular injury during drilling.
Step-by-Step Surgical Approach and Fixation Technique
Surgical execution in shoulder instability requires uncompromising precision. For an arthroscopic Bankart repair, standard posterior, anterosuperior, and anteroinferior portals are established. The anteroinferior portal should be placed as low as possible, typically just superior to the subscapularis tendon, to allow for optimal trajectory when placing anchors at the 5:30 position. The labrum and capsule must be aggressively mobilized from the glenoid neck using an elevator or radiofrequency wand until the subscapularis muscle belly is clearly visualized. The glenoid rim is decorticated to bleeding subchondral bone using a high-speed burr to optimize biological healing. Suture anchors are placed on the articular margin, starting inferiorly at the 5:30 position and progressing superiorly to the 3:00 position. The sutures are passed through the capsulolabral complex, shifting the tissue superiorly and laterally to recreate the anatomic bumper and restore the tension of the IGHL.
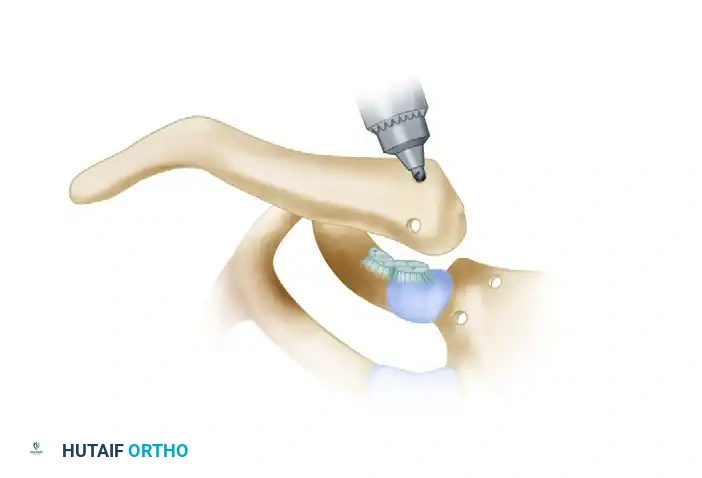
When surgical intervention is absolutely indicated for chronic, symptomatic anterior SC instability, a robust soft-tissue reconstruction is required. Primary capsular repair is universally insufficient due to the extreme biomechanical forces across the SC joint. A strong semitendinosus autograft (harvested from the ipsilateral knee) or a robust allograft is the gold standard for reconstructing the anterior and posterior sternoclavicular ligaments. Biomechanical testing has definitively demonstrated that a figure-of-eight configuration, passed through precise drill holes in the manubrium and medial clavicle, produces a highly stable construct that restores native joint stiffness far better than resection arthroplasty alone.
The procedure begins with a transverse incision over the medial clavicle, extending over the SC joint to the manubrium. The periosteum is carefully elevated. A crucial safety step involves placing a blunt retractor (e.g., a malleable ribbon or a specialized sternal retractor) posterior to the manubrium and clavicle. This physical barrier is non-negotiable; it protects the great vessels from inadvertent plunging of the drill bit. Using a 4.0 mm or 4.5 mm drill bit, two holes are passed anterior to posterior through the medial aspect of the clavicle, and two corresponding holes are drilled through the manubrium.
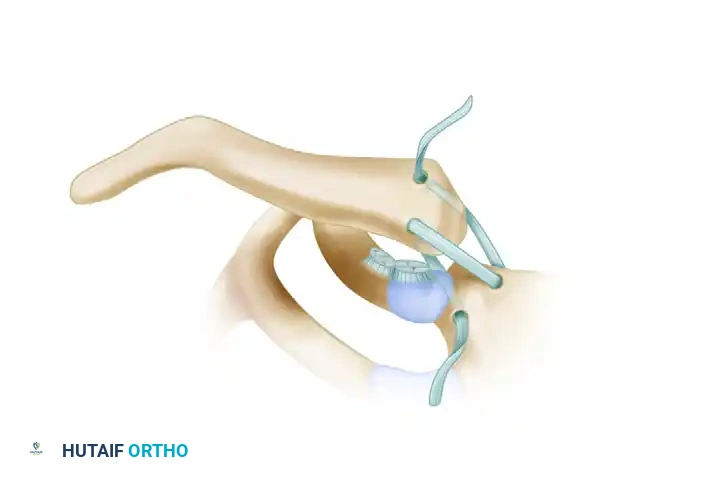
Once the osseous tunnels are prepared, the free semitendinosus tendon graft is meticulously woven through the drill holes in a figure-of-eight pattern. To prevent catastrophic compression of the retrosternal structures, the tendon strands must run parallel to each other posterior to the joint, while crossing each other anterior to the joint.
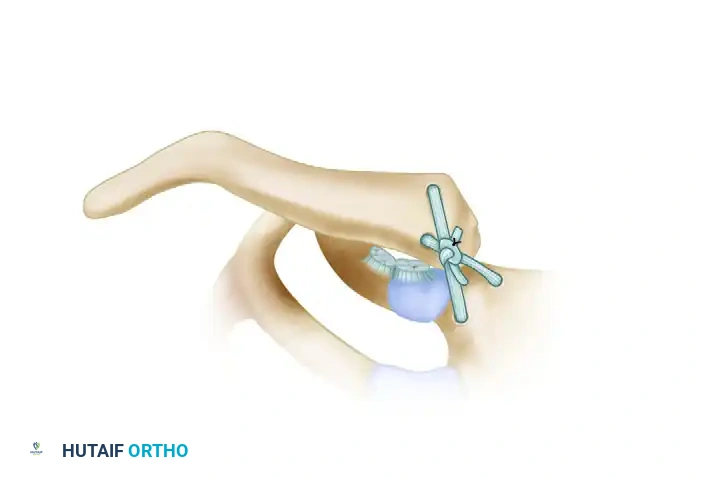
Following graft passage, the SC joint is manually reduced and held in strict anatomical alignment by an assistant. The tendon ends are symmetrically tensioned to eliminate creep, tied in a secure square knot anteriorly, and further secured with multiple passes of heavy non-absorbable sutures (e.g., #2 FiberWire). This secondary fixation is critical to prevent graft slippage during the early phases of biological incorporation.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following shoulder instability surgery can be profound and life-altering. Recurrent instability is the most common complication following soft-tissue repair, occurring in 5% to 15% of appropriately selected patients, but skyrocketing to over 60% if critical bone loss is missed. Stiffness, particularly a loss of external rotation, is the second most common complication, often resulting from over-tensioning the anterior capsule, placing anchors too medially on the glenoid neck, or prolonged post-operative immobilization.
Neurologic injuries, while less common, are devastating. The axillary nerve is at highest risk during the inferior capsular release in a Bankart repair or during the Latarjet procedure as it courses inferior to the glenoid. The musculocutaneous nerve is highly susceptible to traction injury during the coracoid mobilization and transfer in the Latarjet procedure. Hardware complications include prominent suture knots causing chondral abrasion, anchor pullout, or screw breakage/migration in bony procedures. In SC joint reconstruction, the most feared complication is retrosternal vascular injury, which carries a high mortality rate if not immediately managed by a vascular surgeon.
Salvage management requires a precise diagnostic workup to identify the mode of failure. A failed arthroscopic Bankart in the presence of unrecognized bone loss mandates a Latarjet procedure. A failed Latarjet procedure (due to graft osteolysis or non-union) represents a complex salvage scenario, typically requiring an Eden-Hybinette procedure (iliac crest bone grafting) or a fresh distal tibial allograft to restore the glenoid articular arc.
| Complication | Incidence Rate | Prevention Strategy | Salvage Management |
|---|---|---|---|
| Recurrent Instability (Post-Bankart) | 5% - 15% | Pre-op 3D CT to rule out >20% bone loss; accurate anchor placement on articular margin. | Revision to Latarjet or Iliac Crest Bone Graft (Eden-Hybinette). |
| Loss of External Rotation | 10% - 20% | Avoid over-plication of the capsule; early passive ROM in Phase I rehab. | Aggressive physical therapy; Arthroscopic capsular release if refractory >6 months. |
| Coracoid Graft Non-Union / Osteolysis | 5% - 10% (Latarjet) | Meticulous decortication of glenoid neck and coracoid; rigid two-screw compression fixation. | Revision bone grafting (Distal tibial allograft or Iliac crest); hardware removal if symptomatic. |
| Axillary / Musculocutaneous Neuropraxia | 1% - 3% | Avoid medial plunging during inferior capsular release; limit medial retraction of conjoined tendon. | Observation and EMG at 6 weeks; surgical neurolysis if no recovery by 3-6 months. |
| Retrosternal Vascular Injury (SC Joint) | <1% (but catastrophic) | Mandatory pre-op CT Angio; strict use of posterior malleable retractor during drilling. | Immediate packing; emergent sternotomy and repair by thoracic/vascular surgery. |
Phased Post-Operative Rehabilitation Protocols
Meticulous post-operative care is just as critical as the surgical execution to protect the healing graft while preventing debilitating arthrofibrosis. The rehabilitation protocol must be tailored to the specific procedure performed, the quality of the tissue, and the patient's ultimate functional goals.
Phase I: Maximal Protection Phase (0-4 weeks)
For both glenohumeral and SC joint reconstructions, the upper extremity is strictly immobilized in a sling. Active elbow, wrist, and hand range of motion (ROM) are encouraged to prevent distal stiffness and promote venous return. For Bankart repairs, passive forward elevation is typically limited to 90 degrees, and external rotation is limited to neutral or 20 degrees to protect the anterior capsulolabral repair. For SC joint reconstructions, shoulder ROM is strictly limited to pendulum exercises. Elevation above 90 degrees and any cross-body adduction are unequivocally prohibited to prevent levering stress on the medial clavicle.
Phase II: Moderate Protection and ROM Phase (4-8 weeks)
The sling is discontinued. Gradual progression of passive to active-assisted ROM begins. The goal is to restore full forward elevation and gradually increase external rotation. Scapular retraction exercises are initiated to combat the SICK scapula syndrome. Closed kinetic chain exercises, such as wall slides, are utilized to stimulate proprioceptive mechanoreceptors without placing undue shear stress across the glenohumeral joint.
Phase III: Early Strengthening Phase (8-12 weeks)
Active ROM should be normalized by the end of this phase. Isotonic strengthening of the rotator cuff and periscapular musculature commences. Exercises focus on the concavity-compression mechanism, utilizing rhythmic stabilization and perturbation training. For SC joint patients, light resistance bands can be introduced, but heavy pushing or pulling remains restricted.
Phase IV: Advanced Strengthening and Return to Play (3-6 months)
Return to heavy lifting, overhead throwing, and contact sports is delayed until at least 6 months postoperatively. Clearance is strictly contingent upon the restoration of full, painless ROM, symmetric strength (at least 90% of the contralateral limb on isokinetic testing), and psychological readiness. Proprioceptive neuromuscular facilitation (PNF) patterns are heavily emphasized to prevent recurrent dyskinesis. Athletes must pass functional testing specific to their sport before full clearance is granted.
Summary of Landmark Literature and Clinical Guidelines
The evolution of shoulder instability management is deeply rooted in several landmark publications that have shaped modern clinical guidelines. Rowe et al. initially defined the criteria for successful outcomes following Bankart repairs, emphasizing stability, motion, and function. However, it was the seminal work by Burkhart and DeBeer in 2000 that revolutionized the field. Their publication in Arthroscopy identified the "inverted pear" glenoid and the engaging Hill-Sachs lesion, definitively proving that arthroscopic soft-tissue repair in the presence of significant bone loss yields an unacceptable 67% recurrence rate.
Subsequently, Itoi and colleagues advanced our understanding of the glenoid track concept, providing a biomechanical framework to determine whether a Hill-Sachs lesion will engage the anterior glenoid rim during functional arcs of motion. This concept dictates whether a concomitant Remplissage procedure (insetting the infraspinatus into the humeral defect) is required alongside a Bankart repair.
Balg and Boileau's introduction of the Instability Severity Index Score (ISIS) in the Journal of Bone and Joint Surgery (Br) provided a validated, objective scoring system to predict failure after arthroscopic stabilization. By assigning point values to age, sports participation, hyperlaxity, and radiographic bone loss, the ISIS score remains an indispensable tool for surgical triaging. Finally, the long-term natural history studies by Hovelius et al. provide critical perspective, reminding the orthopedic community that while recurrent instability is common in the young, a significant cohort will achieve spontaneous stabilization over decades, a fact that must be integrated into the informed consent process for first-time dislocators.
