Mastering the Management of Chronic Unreduced Shoulder Dislocations
Key Takeaway
Chronic unreduced shoulder dislocations present complex reconstructive challenges due to severe soft-tissue contractures, capsular bowstringing, and significant osteochondral defects. Management requires meticulous preoperative CT evaluation to quantify articular damage. Treatment ranges from benign neglect in low-demand patients to complex open reduction, subscapularis transfer (McLaughlin procedure), or arthroplasty. Successful surgical intervention demands precise neurovascular protection, particularly of the axillary artery and nerve, alongside rigid postoperative immobilization protocols.
Comprehensive Introduction and Patho-Epidemiology
Old, unreduced dislocations of the glenohumeral joint represent a formidable and technically demanding challenge to the orthopaedic surgeon. Typically defined in the literature as dislocations that have been present for greater than three to four weeks, these injuries most frequently occur in patients older than 50 years, though they can manifest in any demographic under specific clinical conditions. The primary clinical complaints upon presentation are chronic, debilitating pain and a profound, rigid limitation of glenohumeral motion. Pain is typically exacerbated by any attempt to move the shoulder beyond its newly restricted, pathological range, as the displaced humeral head impinges upon the surrounding neurovascular and myofascial structures. The chronicity of the dislocation allows for severe soft-tissue contractures and progressive osseous destruction, fundamentally altering the surgical approach required for successful management.
While the vast majority of these chronic dislocations are traumatic in origin, they are frequently precipitated by seemingly trivial injuries in the elderly population. This phenomenon is largely attributed to the age-related degeneration of the dynamic and static stabilizers of the shoulder, including the rotator cuff musculature, the subscapularis tendon, and the capsulolabral complex. In younger demographics, unreduced dislocations are highly correlated with specific, severe comorbidities. Notably, chronic alcoholism, poorly controlled seizure disorders, and high-energy polytrauma are the most common predisposing factors. In the setting of polytrauma, the initial shoulder injury is frequently overlooked during the acute resuscitation phase, as the trauma team rightfully prioritizes life-threatening craniocerebral, thoracic, or abdominal injuries.
Posterior dislocations are particularly notorious for delayed diagnosis. It is estimated that up to 50% of acute posterior shoulder dislocations are missed during the initial emergency department evaluation. This diagnostic failure is almost exclusively due to the reliance on standard, single-plane anteroposterior (AP) radiographs, which fail to adequately demonstrate the posterior displacement of the humeral head relative to the glenoid. In an AP projection, a posterior dislocation may only present as a subtle "lightbulb sign" due to fixed internal rotation, or a loss of the normal elliptical overlap between the humeral head and the glenoid (the "half-moon" sign). By the time the patient is referred to an orthopaedic specialist for persistent pain and inability to externally rotate the arm, weeks or months may have elapsed, cementing the diagnosis of a chronic unreduced dislocation.
According to extensive epidemiological studies by Schulz et al., more than 50% of chronic unreduced dislocations are complicated by concomitant fractures of the glenoid cavity, humeral tuberosities, or the proximal humeral shaft. Furthermore, over one-third of these patients present with established, chronic neurological deficits. The axillary nerve is most frequently compromised, followed by the suprascapular and musculocutaneous nerves. This high incidence of concomitant injury mandates a thorough, exhaustive preoperative clinical neurological assessment, often supplemented by electromyographic (EMG) and nerve conduction velocity (NCV) studies to establish a baseline prior to any surgical intervention.
Detailed Surgical Anatomy and Biomechanics
The chronicity of an unreduced shoulder dislocation induces profound, progressive pathological alterations in both the osseous architecture and the surrounding soft-tissue envelope. A masterful understanding of these distorted anatomical relationships is paramount for the operating surgeon to safely navigate the surgical planes, achieve a stable reduction, and avoid catastrophic iatrogenic neurovascular injury.
Soft-Tissue Contractures and the Bowstringing Phenomenon
Within weeks of the initial dislocation, severe fibrous and capsular contractures develop across the base of the empty glenoid. The rotator cuff muscles, deprived of their normal resting tension and excursion, undergo rapid adaptive shortening, atrophy, and dense fibrosis. This fibrotic cascade frequently engulfs adjacent critical structures. The axillary nerve, which normally traverses inferior to the capsule through the quadrangular space, becomes densely tethered to the inferior capsule and the subscapularis muscle belly. Similarly, the axillary artery can become encased in scar tissue, severely distorting normal surgical planes and significantly elevating the risk of intraoperative vascular injury, particularly in elderly patients with atherosclerotic vessels.
Neviaser classically described the capsular "bowstringing" phenomenon, which is the defining soft-tissue obstacle in chronic unreduced dislocations. In this pathological state, the redundant, torn joint capsule falls across the empty glenoid fossa and becomes densely, tenaciously adherent to the articular cartilage. This fibrotic obliteration of the joint space acts as an absolute mechanical block. It renders closed manipulative reduction physically impossible, as the humeral head cannot re-enter a fossa that is completely filled with mature scar tissue. Consequently, meticulous open surgical release and excision of this fibrotic tissue are absolute prerequisites for joint reduction.
Progressive Osseous Pathology
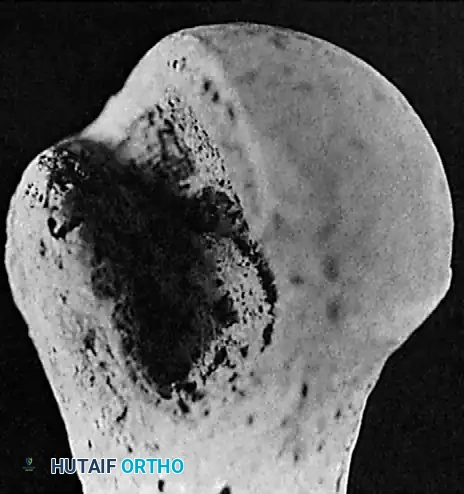
The bony architecture of the glenohumeral joint is progressively destroyed by the persistent abnormal articulation. Because the patient repeatedly attempts to mobilize the joint for activities of daily living, the displaced humeral head continuously grinds against the sharp cortical rim of the glenoid, leading to massive, expansile osteochondral defects.
In chronic anterior dislocations, the posterolateral aspect of the humeral head is driven against the sharp anterior rim of the glenoid. This constant, forceful impingement produces a massive compression fracture. Unlike the classic, relatively shallow Hill-Sachs lesion seen in recurrent, acute anterior instability, the defect in a chronic unreduced dislocation is typically much larger, deeper, and more medially extended.
Concurrently, the anterior glenoid rim suffers severe compression fractures and progressive erosive wear. In long-standing, neglected cases, the body attempts to adapt to the new biomechanical environment by forming a false joint or "pseudoarticulation" between the displaced humeral head and the anterior aspect of the scapular neck. This pseudoarticulation is characterized by reactive sclerosis, osteophyte formation, and a pseudo-capsule.

Chronic posterior dislocations produce a reverse Hill-Sachs lesion—a massive compression fracture on the anteromedial aspect of the humeral head caused by impingement against the posterior glenoid rim. Similar to anterior variants, these defects enlarge significantly over time due to the patient's continual, forceful attempts to increase their range of motion, particularly in external rotation. If the anteromedial defect exceeds 20% to 25% of the articular surface, it will mechanically engage the posterior glenoid rim upon reduction, rendering the joint inherently unstable and necessitating complex structural bone grafting or tendon transfer procedures to restore stability.
Exhaustive Indications and Contraindications
The management of chronic unreduced dislocations is highly individualized and fraught with complex decision-making. The surgeon must carefully weigh the patient's physiological age, functional demands, medical comorbidities, the duration of the dislocation, and the precise extent of osseous destruction. Options range from benign neglect to complex total joint arthroplasty.
| Treatment Modality | Primary Indications | Absolute and Relative Contraindications |
|---|---|---|
| Benign Neglect | Elderly, low-demand patients; severe medical comorbidities precluding anesthesia; painless fixed posterior dislocations with acceptable hand-to-mouth function. | Young, active patients; severe, intractable pain; progressive neurological deficit; significant vascular compromise. |
| Closed Reduction | Dislocation present for less than 3-4 weeks; minimal articular surface defect (<20%); physiologically robust patient. | Dislocation >4 weeks; humeral head defect >20%; severe osteoporosis; elderly patients with severe atherosclerosis (risk of axillary artery rupture). |
| Open Reduction (Joint Preservation) | Dislocation present for <6 months; articular surface defect <45%; active patient with good bone stock; failed closed reduction. | Articular defect >45%; dislocation >6-12 months; severe avascular necrosis (AVN) of the humeral head; profound glenoid bone loss. |
| McLaughlin Procedure (or Neer Modification) | Chronic posterior dislocation; anteromedial humeral head defect between 20% and 45%; engages posterior glenoid upon reduction. | Defect >45% (requires arthroplasty); anterior dislocations; severe degenerative joint disease of the remaining articular surface. |
| Arthroplasty (Hemi, TSA, or RTSA) | Articular defect >45%; dislocation >6 months; severe AVN; elderly patients with non-reconstructible proximal humerus fractures. | Active systemic infection; profound deltoid or axillary nerve paralysis (relative contraindication for RTSA, absolute for TSA); non-compliant patient. |
Not all patients require surgical intervention. In elderly, low-demand patients with severe, life-limiting medical comorbidities, the physiological stress and risks of complex shoulder surgery may far outweigh the potential functional benefits. Hawkins et al. documented a cohort of patients with persistent locked posterior dislocations who underwent no treatment; over a 3 to 8-year longitudinal follow-up, their pain did not progress and remained highly tolerable. It is a critical surgical pearl to recognize that patients with untreated posterior dislocations generally exhibit significantly higher functional scores than those with untreated anterior dislocations. The internally rotated position of a posterior dislocation preserves essential hand-to-mouth and hand-to-torso function, whereas the fixed external rotation of an anterior dislocation severely limits basic activities of daily living.
Manipulative closed reduction is fraught with catastrophic complications in the chronic setting and should only be attempted after exhaustive consideration of the patient's bone density, vascular status, and the precise duration of the dislocation. If attempted, it must be performed in the operating room under general anesthesia with complete neuromuscular blockade to eliminate muscular resistance. Traction must be minimal, sustained, and strictly in-line; forceful leverage maneuvers (such as the Kocher technique) are strictly forbidden. In elderly patients with atherosclerotic disease, forceful reduction carries a devastating risk of axillary artery rupture, a life-threatening emergency.
Open reduction is generally indicated for dislocations present for less than 6 months with an articular surface defect of less than 45%. The surgical obstacles are twofold: first, achieving reduction, which is severely hindered by the dense fibrosis, muscle shortening, and capsular bowstringing; and second, maintaining the reduction, which is compromised by the large osteochondral defect and inherent soft-tissue incompetence. As established by Hawkins and Neer, open reduction uniformly fails and results in immediate re-dislocation or severe secondary osteoarthritis if the articular defect exceeds 45% or if the dislocation has been present for over a year. In such advanced cases, prosthetic arthroplasty is the definitive treatment of choice.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful management for chronic unreduced dislocations. The clinical evaluation must be exhaustive. Loss of motion is the hallmark clinical finding, and the specific pattern of restriction is highly diagnostic. In old anterior dislocations, there is severe restriction in abduction and internal rotation. The arm is typically held away from the body in fixed external rotation, making it exceedingly difficult for the patient to reach their face and physically impossible to reach their back. Conversely, old posterior dislocations present with severe restriction in abduction and external rotation. The arm rests closely at the side in fixed internal rotation. Interestingly, this position allows the patient to reach their face, head, and torso, which often masks the functional deficit from the patient and the initial evaluating physician, leading to significant delays in diagnosis.
A complete, high-quality radiographic trauma series is absolutely mandatory. This must include a true anteroposterior (Grashey) view, a scapular Y view, and an axillary lateral view. The axillary view is the undisputed gold standard for confirming the exact direction of the dislocation, identifying the presence of a locked joint, and visualizing the engagement of the glenoid rim within the humeral head defect.

While plain radiographs are essential for initial diagnosis, they are insufficient for comprehensive surgical planning. As heavily emphasized by Kirtland et al., computed tomography (CT) with three-dimensional (3D) reconstruction is the definitive imaging modality for evaluating the complex bony injuries associated with chronic dislocations. CT accurately quantifies the exact volume and percentage of articular surface damage on the humeral head (the Hill-Sachs or reverse Hill-Sachs lesion) and assesses the degree of glenoid bone loss. The precise quantification of the humeral head defect is the single most critical determining factor in selecting the appropriate surgical intervention (e.g., joint preservation versus arthroplasty).

Preoperative templating must be performed on the CT scans if arthroplasty is being considered. The surgeon must anticipate severe glenoid retroversion or anterior wear, which may require eccentric reaming or augmented glenoid baseplates in the setting of reverse total shoulder arthroplasty (RTSA). Furthermore, a thorough preoperative electromyographic (EMG) and nerve conduction study is highly recommended to document any pre-existing axillary or brachial plexus neurapraxia, which is vital for both surgical planning and medicolegal protection.
Patient positioning is typically performed in the modified beach-chair position, with the head securely stabilized and the operative arm draped entirely free to allow for unrestricted manipulation. A lateral decubitus position is rarely utilized for open management of chronic dislocations, as it restricts the extensile anterior exposures frequently required. General anesthesia is mandatory, often supplemented by an interscalene regional nerve block for optimal postoperative pain control.
Step-by-Step Surgical Approach and Fixation Technique
Open Reduction of Anterior Dislocations (Rowe and Zarins Technique)
The surgical approach to a chronic anterior dislocation is a masterclass in navigating distorted anatomy. Place the patient in the beach-chair position. An extensile anterior approach via the deltopectoral interval is the absolute standard. Make a 10 to 12.5 cm incision extending inferiorly from the lateral third of the clavicle, following the contour of the deltopectoral groove.
Develop the deltopectoral interval meticulously. The cephalic vein is typically retracted laterally with the deltoid muscle to preserve its venous drainage, though medial retraction is acceptable depending on surgeon preference and venous anatomy. Deepen the dissection by retracting the conjoined tendon (short head of the biceps and coracobrachialis) medially. In a chronic anterior dislocation, the displaced, deformed humeral head will be immediately palpable or visible inferior and medial to the coracoid process, often encased in a dense bursa and scar tissue.
Before any attempt at reduction is made, the contracted capsule must be widely opened, and the coracohumeral ligament completely divided. The glenoid cavity must be visualized and meticulously cleared of all adherent fibrous tissue. This addresses Neviaser's bowstringing phenomenon; failure to completely excise this fibrotic plug from the glenoid fossa will make reduction impossible.
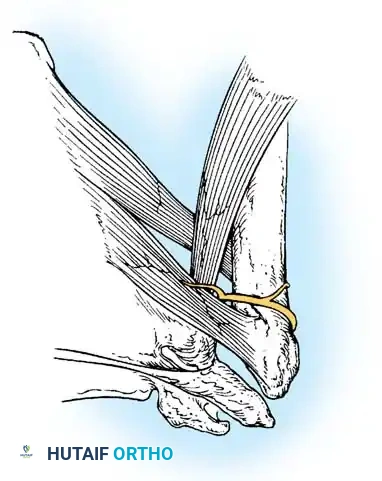
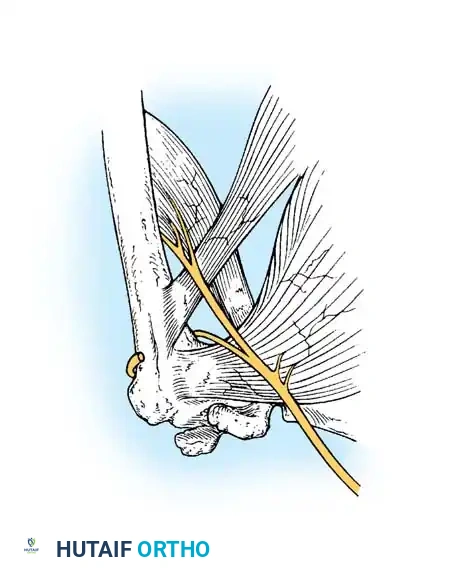
Release of the subscapularis tendon is mandatory. This can be achieved via a formal tenotomy, a lesser tuberosity osteotomy, or a subscapularis peel, depending on the anticipated need for subsequent tendon transfer or arthroplasty. Crucial Step: The axillary nerve is highly vulnerable during this step. In chronic anterior dislocations, the subscapularis and inferior capsule are displaced anteriorly and medially, creating a chronic traction injury on the axillary nerve. The nerve is tethered at the brachial plexus above and the quadrangular space below, pulling it directly across the inferior aspect of the surgical field. The surgeon must actively identify and protect the axillary nerve before releasing the inferior capsule.
Once the glenoid is cleared and the soft tissues are fully mobilized, gently lever the humeral head back into the glenoid cavity. The surgeon must avoid excessive mechanical force with retractors, bone levers, or elevators. The chronically dislocated humeral head is invariably osteoporotic, and forceful leverage will result in catastrophic iatrogenic fractures of the humeral head or the glenoid rim. Once reduced, gently manipulate the shoulder through a range of motion to stretch the contracted soft tissues until a near-normal, stable arc of motion is achieved. The capsule is typically too contracted to permit primary closure; therefore, it is left open. Carefully repair the subscapularis tendon or osteotomy, maintaining strict awareness of the axillary nerve's proximity.
Management of Posterior Dislocations and Bony Defects
For chronic posterior dislocations, the surgical approach may vary. While historical texts by Neviaser and Rowe recommended a superior approach, an anteromedial approach (deltopectoral) is modernly preferred. It provides excellent access to the reverse Hill-Sachs defect on the anteromedial humeral head and allows for simultaneous management of the subscapularis.
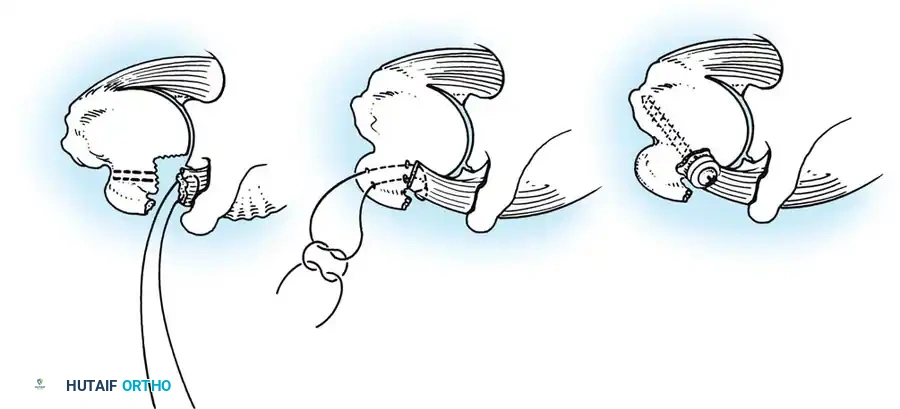
The McLaughlin Procedure and Neer Modification:
When the anteromedial humeral head defect is between 20% and 45% of the articular surface, it will engage the posterior glenoid rim upon internal rotation, causing recurrent posterior instability. McLaughlin originally described a technique to fill this defect by detaching the subscapularis tendon from the lesser tuberosity and transferring it directly into the defect. Neer later modified this by performing a lesser tuberosity osteotomy, transferring the bone plug with the attached subscapularis into the defect, and securing it with cancellous screws. This effectively converts an unstable intra-articular defect into a stable extra-articular one, preventing glenoid engagement.
Advanced Reconstruction and Arthroplasty
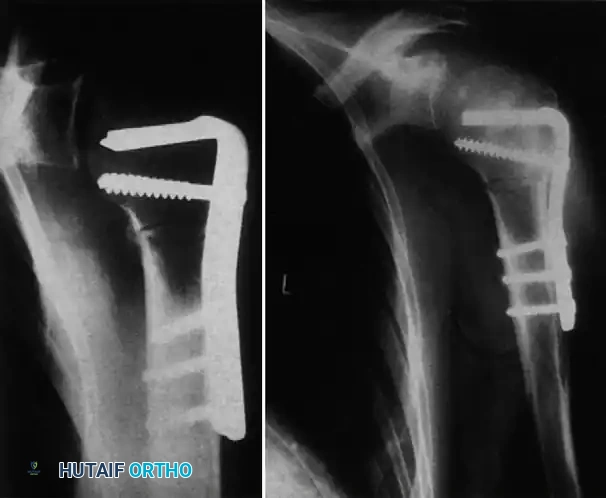
In cases where the humeral head is deemed non-salvageable—defined by an articular defect exceeding 45%, a dislocation duration greater than 6 to 12 months, or the presence of severe avascular necrosis—prosthetic joint replacement is absolutely required. Depending on the patient's age, rotator cuff integrity, and glenoid bone stock, this may involve a hemiarthroplasty, a total shoulder arthroplasty (TSA), or a reverse total shoulder arthroplasty (RTSA). In modern practice, RTSA has become the workhorse for elderly patients with chronic dislocations, as it bypasses the invariably compromised rotator cuff and provides excellent inherent stability. In cases complicated by severe proximal humerus fractures or nonunions associated with the dislocation, rigid internal fixation with locking plates may be required as a salvage procedure before or in conjunction with joint reconstruction.
Methods of Postoperative Fixation and Immobilization
Maintaining the reduction postoperatively is just as critical, and often as difficult, as the reduction itself. Due to the massive capsular stretching and bony defects, the joint is highly prone to immediate re-dislocation in the recovery room. Several techniques have been described to prevent this:
1. Transarticular Fixation:
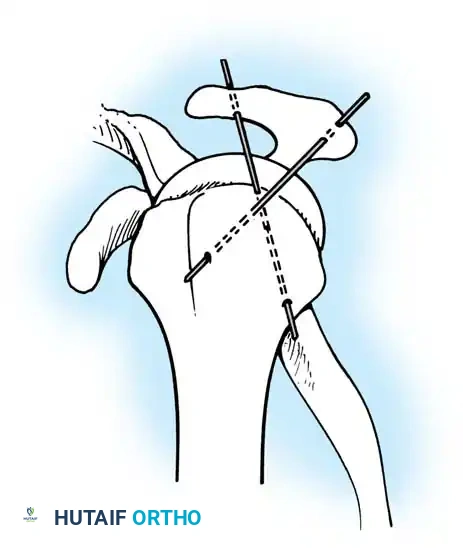
Neviaser historically recommended transfixing the glenohumeral joint to provide rigid temporary stability. This involves driving a large threaded Steinmann pin or a Swiss screw from the lateral humerus directly into the glenoid vault.

Alternatively, Wilson and McKeever described the use of heavy, crossed Kirschner wires driven superiorly through the acromion directly into the humeral head. While effective at preventing re-dislocation, transarticular hardware carries a high risk of hardware breakage, articular cartilage damage, and pin-tract infections, and is generally reserved for extreme salvage cases today.
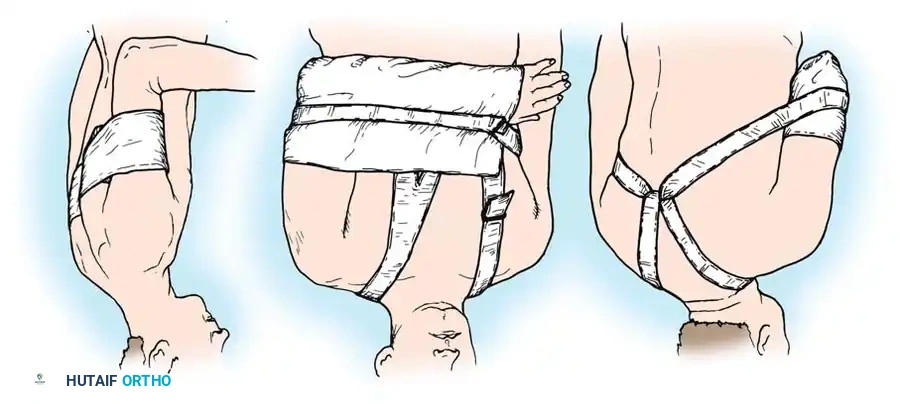
2. Positional Immobilization (Rowe and Zarins):
Rowe and Zarins strongly argued against the use of transarticular hardware, advocating instead for strict, rigid positional immobilization using custom orthoses or spica casts.
* For Chronic Anterior Dislocations: The joint is most unstable in external rotation and abduction. Therefore, the arm is rigidly immobilized anterior to the coronal plane of the body in internal rotation.
* For Chronic Posterior Dislocations: The joint is most unstable in internal rotation. The arm must be immobilized posterior to the coronal plane of the body, or in a "gunslinger" orthosis in neutral to slight external rotation.
Complications, Incidence Rates, and Salvage Management
The surgical management of chronic unreduced shoulder dislocations is associated with a notoriously high complication rate. The surgeon must be prepared to manage severe intraoperative and postoperative adverse events.
| Complication | Estimated Incidence | Prevention Strategy | Salvage Management |
|---|---|---|---|
| Axillary Nerve Injury | 10% - 15% | Direct visualization and neurolysis prior to inferior capsular release; avoid excessive traction. | Observation for 3-6 months; if no EMG recovery, consider nerve grafting or tendon transfers (e.g., L'Episcopo). |
| Axillary Artery Rupture | <1% (Higher in elderly) | Avoid forceful closed reduction in patients >60 years; meticulous sharp dissection of fibrotic planes. | Immediate intraoperative vascular surgery consultation; direct repair or saphenous vein interposition graft. |
| Re-dislocation | 15% - 20% | Strict adherence to positional immobilization; use of McLaughlin transfer for engaging defects. | Revision open reduction; conversion to Reverse Total Shoulder Arthroplasty (RTSA). |
| Avascular Necrosis (AVN) | 20% - 30% | Minimize soft-tissue stripping of the humeral head; avoid excessive disruption of the ascending branch of the anterior circumflex humeral artery. | If symptomatic and progressive, conversion to hemiarthroplasty or total shoulder arthroplasty. |
| Severe Postoperative Stiffness | 40% - 60% | Early, controlled passive range of motion; meticulous capsular release during initial surgery. | Arthroscopic or open capsular release after 6-9 months if functional ROM is not achieved. |
Vascular injury, while relatively rare, is the most catastrophic immediate complication. The axillary artery becomes rigid and inelastic due to atherosclerosis in the elderly population. When a chronically dislocated humerus is forcefully manipulated, the tethered artery can easily rupture, leading to rapid exsanguination or devastating limb ischemia.
Avascular necrosis (AVN) of the humeral head is a delayed complication that often presents months to years after a successful open reduction. The initial trauma, combined with the extensive soft-tissue stripping required to achieve reduction, severely compromises the delicate blood supply to the humeral head. Surgeons must counsel patients preoperatively that even if the joint is successfully preserved, secondary AVN may ultimately necessitate a delayed arthroplasty.
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following the open reduction of a chronic dislocation is a delicate balancing act. The surgeon and physical therapist must navigate the narrow therapeutic window between preventing catastrophic re-dislocation and avoiding profound, permanent joint stiffness.
If internal fixation (such as transarticular screws or crossed K-wires) is utilized, the arm is strictly supported in an abduction splint or a rigid spica cast. Absolutely no glenohumeral motion is permitted. The hardware is typically removed at 3 to 4 weeks in the outpatient clinic, after which early motion can begin.
If strict positional immobilization (the Rowe and Zarins method) is employed without hardware, the custom orthosis is maintained continuously for exactly 3 to 4 weeks.
Phased Rehabilitation:
* Weeks 0-3/4: Strict immobilization. Only active range of motion of the elbow, wrist, and hand is permitted to prevent distal edema and stiffness.
* Weeks 3-4: The orthosis is discontinued. The patient initiates gentle, gravity-assisted pendulum exercises. These must be performed strictly within the pain-free arc.
* Weeks 4-8: Progress to active-assisted and passive range of motion (PROM) within the limits of comfort. Aggressive passive stretching by the therapist is strictly avoided during this phase, as it can easily stretch the healing anterior or posterior restraints and precipitate a re-dislocation.
* Months 2-6: Isotonic strengthening of the rotator cuff and deltoid begins. The shoulder should continue to be supported in a resting splint at night until dynamic muscular stability is fully restored. Maximum medical improvement is typically not reached until 9 to 12 months postoperatively.
It is imperative to aggressively manage patient expectations from the very first preoperative consultation. Full, normal, symmetrical function of the shoulder is rarely, if ever, regained after the open reduction of a chronic dislocation. Motion will remain permanently limited, particularly in the extremes of abduction and external rotation. The primary, realistic goals of surgical intervention are the relief of chronic resting pain, the restoration of basic activities of daily living (such as reaching the mouth and perineum), and the prevention of further progressive neurovascular compromise.
Summary of Landmark Literature and Clinical Guidelines
The modern algorithms for treating chronic unreduced shoulder dislocations are built upon several foundational pillars of orthopaedic literature.
Neviaser's classic anatomical studies were the first to definitively identify the "bowstringing" of the joint capsule across the glenoid fossa. This singular observation shifted the paradigm away from forceful, dangerous closed reductions and established the absolute necessity of open capsular excision to achieve a concentric reduction.
Rowe and Zarins provided the definitive clinical series on the open surgical approach. They codified the extensile deltopectoral approach, highlighted the extreme vulnerability of the axillary nerve, and proved that strict positional immobilization was superior to transarticular hardware in preventing immediate postoperative re-dislocation while minimizing hardware-related complications.
For posterior dislocations, McLaughlin's original description of transferring the subscapularis tendon into the reverse Hill-Sachs defect remains a cornerstone technique. Neer's subsequent modification—transferring the lesser tuberosity bone plug rather than just the tendon—provided superior bone-to-bone healing and is now the preferred technique for defects between 20% and 45%.
Finally, Hawkins and Neer's longitudinal outcome studies established the modern indications for arthroplasty. By demonstrating a near 100% failure rate for joint preservation when the articular defect exceeds 45% or the dislocation has been neglected for over a year, they provided surgeons with clear, objective parameters for abandoning heroic open reductions in favor of immediate prosthetic replacement, thereby saving patients from the morbidity of multiple failed reconstructive surgeries.
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics and has been medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is designed to assist orthopedic residents ---
