Multidirectional Shoulder Instability: Comprehensive Surgical Management
Key Takeaway
Multidirectional instability (MDI) of the shoulder is characterized by symptomatic glenohumeral subluxation or dislocation in multiple directions, primarily driven by a redundant inferior capsular pouch. Surgical intervention, such as the Neer inferior capsular shift or glenoid bone grafting, is indicated only after exhaustive conservative rehabilitation fails. This guide details the biomechanics, step-by-step surgical techniques, and postoperative protocols for managing complex MDI.
Comprehensive Introduction and Patho-Epidemiology
Introduced into the orthopedic lexicon by Charles Neer and C.R. Foster in 1980, the term multidirectional instability (MDI) describes symptomatic glenohumeral subluxation or dislocation occurring in multiple directions—specifically anterior, posterior, and inferior. Unlike acute traumatic dislocations, the primary pathoanatomic abnormality driving multidirectional instability is a loose, highly redundant, and patulous inferior capsular pouch, almost invariably accompanied by a widened rotator interval. This global capsular redundancy creates a biomechanical environment where the humeral head fails to remain centered within the glenoid vault during dynamic arcs of motion, leading to repetitive microtrauma, labral attenuation, and profound patient disability.
It is of paramount clinical importance for the evaluating surgeon to distinguish multidirectional instability from routine unidirectional traumatic dislocation. The latter is classically conceptualized under the TUBS acronym (Traumatic, Unidirectional, Bankart, Surgery), where a discrete pathological lesion—such as an anteroinferior labral avulsion—can be surgically repaired to restore stability. Conversely, MDI typically falls under the AMBRI classification paradigm (Atraumatic, Multidirectional, Bilateral, Rehabilitation, Inferior capsular shift). Because the underlying pathology in MDI is an intrinsic global capsular redundancy rather than a discrete labral avulsion, it is fundamentally not correctable by standard unidirectional repairs. Attempting an isolated Bankart repair in an MDI patient will reliably fail, as the untreated inferior and posterior capsular volume will continue to permit pathological translation.
The epidemiology of multidirectional instability reveals a bimodal presentation, predominantly affecting adolescents and young adults in their second and third decades of life. There is a strong predilection for overhead athletes, such as competitive swimmers, gymnasts, and volleyball players, whose repetitive microtraumatic stretching of the capsuloligamentous complex exacerbates an underlying baseline laxity. Furthermore, a substantial subset of these patients exhibits generalized ligamentous laxity, which can be quantified using the Beighton score. In severe cases, the surgeon must maintain a high index of suspicion for underlying heritable disorders of connective tissue, such as Ehlers-Danlos syndrome or Marfan syndrome, which alter type I and type III collagen cross-linking, rendering soft-tissue plication procedures highly susceptible to late attenuation and clinical failure.
The pathophysiology of MDI is essentially a failure of the static and dynamic restraints of the glenohumeral joint. While normal shoulders rely on a finely tuned interplay of capsular tension, negative intra-articular pressure, and dynamic rotator cuff compression, the MDI shoulder suffers from a loss of the "cam effect." The redundant capsule fails to wind up and tighten at the extremes of motion. Consequently, the dynamic stabilizers become easily fatigued as they attempt to compensate for the absent static restraints, leading to periscapular dyskinesia, secondary impingement, and a debilitating cycle of pain and subluxation that severely limits the patient's activities of daily living and athletic participation.
Detailed Surgical Anatomy and Biomechanics
The glenohumeral joint is inherently unstable, often likened to a golf ball sitting on a specialized tee. This profound mismatch in articular surface area—where only 25% to 30% of the humeral head articulates with the glenoid at any given time—allows for the greatest range of motion of any joint in the human body, but strictly at the expense of intrinsic bony stability. The osseous architecture is deepened by the glenoid labrum, a fibrocartilaginous ring that increases the depth of the glenoid concavity by approximately 50%, providing a critical "chock-block" effect against humeral head translation. In MDI, while the labrum may be intact, its effectiveness is negated by the overwhelming volume of the joint capsule.
The static stabilization of the shoulder relies on the complex interplay of the glenohumeral ligaments, which function as check-reins at the extremes of motion. The superior glenohumeral ligament (SGHL) and the coracohumeral ligament (CHL) form the boundaries of the rotator interval, a critical anatomical space that, when patulous, permits excessive inferior translation of the adducted arm. The middle glenohumeral ligament (MGHL) provides anterior stability in the mid-ranges of abduction. However, the most critical structure in the pathogenesis of MDI is the inferior glenohumeral ligament (IGHL) complex. Composed of an anterior band, a posterior band, and an intervening axillary pouch, the IGHL functions as a hammock that supports the humeral head. In MDI, this hammock is profoundly elongated, failing to tension adequately during abduction and external rotation, thereby allowing the humeral head to slide inferiorly and anteriorly.
Biomechanically, the concept of "coupled translation" is essential to understanding MDI. In a normal shoulder, as the arm is elevated and rotated, the capsular ligaments on the side opposite the direction of motion become taut, forcing the humeral head into the center of the glenoid. In the MDI shoulder, the global redundancy prevents this obligate centering. For instance, an excessively loose posterior capsule will fail to push the humeral head anteriorly during internal rotation, leading to posterior subluxation. Similarly, a widened rotator interval fails to resist the gravitational pull on the arm, resulting in the classic "sulcus sign." The loss of negative intra-articular pressure, which normally provides a suction-cup effect, further exacerbates this multi-planar instability.
Dynamic stabilization is provided primarily by the rotator cuff musculature and the periscapular stabilizers (serratus anterior, rhomboids, trapezius). These muscles compress the humeral head into the glenoid concavity through a mechanism known as concavity compression. In patients with MDI, the chronic reliance on dynamic stabilizers to prevent subluxation leads to rapid muscular fatigue, altered firing patterns, and profound scapular dyskinesia. The proprioceptive feedback loops, normally triggered by tension in the capsuloligamentous structures, are severely blunted in the redundant capsule. This proprioceptive deficit means the dynamic stabilizers are activated too late in the arc of motion to prevent subluxation, highlighting why targeted neuromuscular rehabilitation is the mandatory first line of treatment.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention in a patient with multidirectional instability is among the most challenging in orthopedic sports medicine. Surgery is strictly contraindicated unless the patient has failed an exhaustive, well-documented, and strictly supervised trial of conservative treatment. This non-operative phase must last a minimum of 6 to 12 months and focus intensely on periscapular muscular rehabilitation, rotator cuff strengthening, and proprioceptive re-education. Only when a patient experiences frequent, significant disability that precludes activities of daily living or prevents return to their desired level of sport, despite maximal non-operative effort, should surgical reconstruction be entertained.
A critical component of the preoperative evaluation is identifying the patient's psychological profile and the precise nature of their instability. The surgeon must definitively rule out voluntary dislocators who utilize abnormal muscle firing patterns to subluxate the joint for secondary gain or psychological reasons. Operating on a habitual, voluntary dislocator with an underlying, untreated psychiatric condition is an absolute contraindication, as the patient will invariably stretch out any surgical repair, leading to catastrophic failure and potentially worse clinical outcomes than the natural history of the disease. Furthermore, patients with profound, unmanaged connective tissue disorders (e.g., severe Ehlers-Danlos hypermobility type) represent a highly precarious surgical demographic, as their intrinsic collagen defects predispose them to recurrent capsular stretching regardless of the surgical technique employed.
The indications for specific surgical procedures within the MDI spectrum depend heavily on the presence or absence of critical glenoid bone loss. While MDI is primarily a soft-tissue pathology, chronic, repetitive dislocations can lead to attritional bone loss. If the anterior glenoid bone loss approaches 20% to 25%, or if there is significant posterior bone loss associated with recurrent posterior dislocations, soft-tissue plication alone will fail. In these instances, a bony augmentation procedure, such as the Eden-Hybbinette, becomes indicated to restore the articular arc. Conversely, in the absence of critical bone loss, a volume-reducing soft-tissue procedure, classically the Neer Inferior Capsular Shift, is the gold standard.
| Clinical Parameter | Surgical Indications | Relative Contraindications | Absolute Contraindications |
|---|---|---|---|
| Conservative Therapy | Failure of 6-12 months of targeted physical therapy | Less than 6 months of supervised rehabilitation | Complete lack of prior conservative management |
| Symptomatology | Disabling pain, recurrent subluxation affecting ADLs/Sports | Mild, asymptomatic laxity or painless subluxation | Asymptomatic hypermobility (e.g., party tricks) |
| Psychiatric Profile | Highly motivated, compliant with postoperative restrictions | Poor compliance history, unrealistic postoperative expectations | Voluntary dislocators with secondary gain motives |
| Tissue Quality | Normal collagen, acquired redundancy from microtrauma | Mild generalized ligamentous laxity (Beighton > 4) | Severe, untreated Ehlers-Danlos or Marfan syndrome |
| Bone Loss | >20% Glenoid loss (Indicates Eden-Hybbinette bone block) | 10-15% bone loss (Gray zone, may need combined approach) | Active joint infection or severe glenohumeral osteoarthritis |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning begins with an exhaustive physical examination, both awake and subsequently under anesthesia. The awake examination must quantify the degree of generalized laxity using the Beighton criteria. Specific to the shoulder, the surgeon must evaluate the sulcus sign with the arm in neutral rotation and external rotation; persistence of the sulcus sign in external rotation strongly implies a patulous rotator interval. Anterior and posterior load-and-shift tests should be graded (1+ to 3+) to determine the primary vector of instability. Advanced imaging is mandatory. A true AP, scapular Y, and axillary lateral radiograph will rule out dysplasia or large osseous defects. Magnetic Resonance Arthrography (MRA) is the imaging modality of choice, providing unparalleled visualization of capsular volume, labral integrity, and the presence of occult partial-thickness rotator cuff tears or capsular avulsions (HAGL lesions).
The cornerstone of surgical decision-making in MDI is the Examination Under Anesthesia (EUA). Once a general anesthetic is administered and complete neuromuscular blockade is achieved, the instability of the shoulder must be systematically re-evaluated to dictate the final surgical approach. Anterior instability is tested with the arm in external rotation and extension at progressive levels of abduction. Inferior instability is quantified by applying longitudinal traction with the arm at 0 degrees and 45 degrees of abduction. Posterior instability is assessed with the arm in internal rotation at various levels of forward elevation, applying a posteriorly directed axial load. The EUA allows the surgeon to confirm the dominant direction of instability without the confounding variable of patient guarding, thereby dictating whether an anterior or posterior surgical approach is warranted.
Patient positioning is critical for optimal exposure and dynamic assessment during the procedure. For an anterior approach (Neer Capsular Shift or Eden-Hybbinette), the patient is typically placed in a modified beach-chair position. The head of the bed is elevated to approximately 45 to 60 degrees, and the patient is shifted laterally so that the entire shoulder girdle, including the medial border of the scapula, is free off the edge of the table. A sterile arm positioner (e.g., Spider arm, McConnell positioner) is highly recommended, as it allows the surgeon to lock the arm in precise degrees of abduction and external rotation during the capsular shift. Proper positioning prevents inadvertent over-tensioning of the capsule, which is the most common technical error in MDI surgery.
If an iliac crest bone graft is anticipated for an Eden-Hybbinette procedure, the ipsilateral iliac crest must be widely prepped and draped into the sterile field. A bump is placed under the ipsilateral hip to elevate the crest, facilitating access for the harvest of a tricortical graft. The surgical team must ensure that the draping allows for simultaneous access to both the shoulder and the pelvis, minimizing operative time and reducing the risk of contamination during the graft transfer process. Prophylactic intravenous antibiotics must be administered within one hour prior to the skin incision, and meticulous hemostasis should be planned to maintain a clear surgical field during deep capsular dissection.
Step-by-Step Surgical Approach and Fixation Technique
Reconstruction of the Anterior Glenoid: The Eden-Hybbinette Procedure
While soft-tissue redundancy is the hallmark of MDI, chronic, repetitive instability can lead to catastrophic attritional glenoid bone loss. When anterior glenoid bone loss exceeds 20% to 25%, soft-tissue procedures alone are biomechanically destined to fail. The Eden-Hybbinette procedure, utilizing an iliac crest autograft, is the gold standard for reconstructing the anterior glenoid vault. The procedure begins with the harvest of a tricortical iliac crest autograft, typically measuring 2 cm wide by 3 cm long. The graft is meticulously contoured on the back table using a high-speed burr. It is imperative that the articulating surface of the graft is shaped to perfectly match the native glenoid radius of curvature.
Exposure of the anterior glenoid is achieved through a standard deltopectoral approach. The subscapularis is split or tenotomized, and the anterior capsule is incised to expose the bony defect. The anterior glenoid neck is thoroughly decorticated using a burr or osteotome down to bleeding subchondral bone. This decortication is critical to maximize the osteogenic healing interface between the native glenoid and the autograft. Two pilot holes are drilled into the native glenoid neck, parallel to the articular surface, and marked with electrocautery for easy identification.
The contoured iliac crest graft is then brought into the field. Appropriate positioning is strictly vertical and flush with the native articular cartilage. The graft must act as a seamless extension of the glenoid track, not as a proud mechanical block, which would rapidly induce secondary osteoarthritis. The graft is secured to the decorticated glenoid neck using two 4.0-mm or 4.5-mm cannulated, partially threaded bicortical screws. The redundant anterior capsule is then repaired directly to the native capsule or anchors placed in the graft, providing a secondary soft-tissue restraint over the bony reconstruction.
Soft Tissue Reconstruction: The Neer Inferior Capsular Shift
For the vast majority of MDI patients without critical bone loss, the primary surgical objective is to obliterate the redundant inferior capsular pouch. The open Neer Inferior Capsular Shift remains the benchmark against which all other procedures are measured. The patient is positioned in the beach-chair position, and a 9-cm deltopectoral incision is made. The cephalic vein is identified and retracted laterally with the deltoid to preserve its venous drainage. The clavipectoral fascia is divided, and the conjoined tendon is retracted medially to expose the underlying subscapularis tendon.
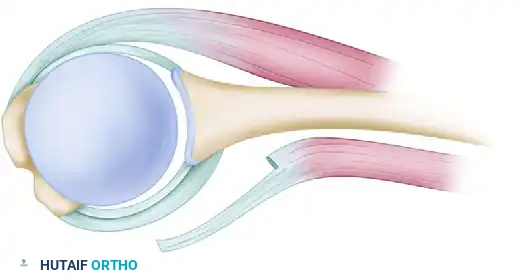
Management of the subscapularis is a critical step. With the arm in external rotation to tension the tendon, the superficial half of the subscapularis thickness is divided transversely, approximately 1 cm medial to the bicipital groove. Crucially, the deep half of the subscapularis tendon is left intimately attached to the underlying anterior joint capsule. This technique reinforces the anterior capsular wall, providing robust tissue for the subsequent shift. The superficial half of the tendon is tagged with heavy non-absorbable stay sutures and retracted medially.
Figure A: Reinforcement of capsular flaps. Notice how approximately half the thickness of the subscapularis tendon is left attached to reinforce the underlying capsule.
Next, a T-shaped capsulotomy is performed. The vertical limb of the incision is made directly adjacent to the humeral articular margin, extending from the rotator interval superiorly down to the 6 o'clock position inferiorly. The horizontal limb is then made perpendicular to the vertical limb, effectively splitting the capsule into a superior flap and an inferior flap.
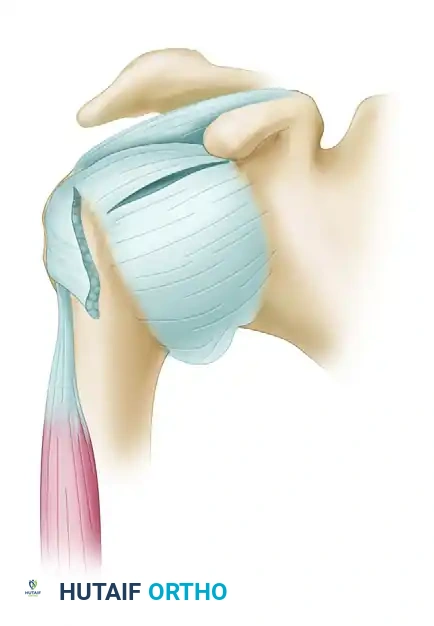
Figure B: The T-shaped capsular incision is created, separating the capsule from the humeral neck to allow for mobilization.
Careful preparation of the flaps is mandatory. The arm must be progressively externally rotated as the inferior flap is detached from the inferior humeral neck. This maneuver pulls the axillary nerve away from the inferior capsule, protecting it from iatrogenic injury. A bony slot is then created, or the humeral neck is aggressively decorticated at the intended site of capsular reattachment, to promote robust soft-tissue-to-bone healing.
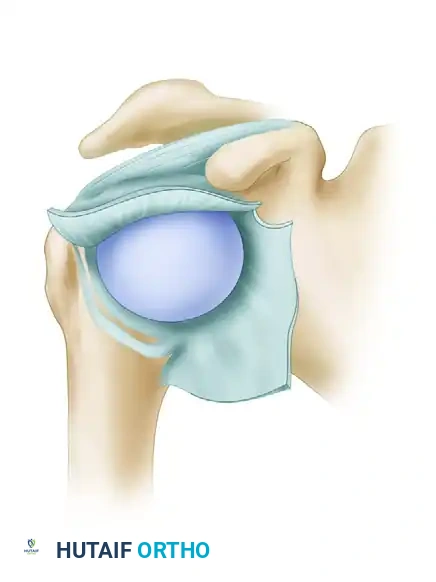
Figure C: Preparation of the capsular flaps and the bony slot on the humeral neck. The arm is externally rotated as the inferior flap is fully mobilized.
The critical step of the procedure is the relocation and shifting of the capsular flaps. The arm is positioned in slight forward flexion and exactly 10 to 15 degrees of external rotation. Securing the flaps with the arm in internal rotation is a catastrophic error, as it will severely over-constrain the joint, leading to an obligate loss of external rotation and early-onset arthropathy. The inferior flap is advanced superiorly and anteriorly, obliterating the redundant inferior pouch, and secured to the prepared bony bed. The superior flap is then brought down over the advanced inferior flap in a overlapping "pants-over-vest" fashion. This double-breasting technique doubles the capsular thickness anteriorly.
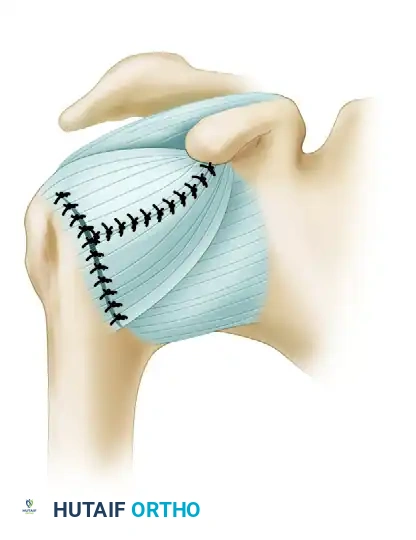
Figure D: Relocation of the flaps with the arm held in slight flexion and 10 degrees of external rotation. The inferior flap is shifted superiorly, and the superior flap is brought down over it, creating a reinforced, tightened anterior restraint.
Finally, the rotator interval is addressed. Imbrication and closure of the rotator interval using heavy non-absorbable sutures are mandatory to eliminate residual inferior translation. The superficial half of the subscapularis is then anatomically repaired back to its footprint on the lesser tuberosity. The arm is taken through a gentle range of motion to confirm stability without excessive constraint before standard layered closure.
Complications, Incidence Rates, and Salvage Management
Surgical intervention for multidirectional instability is fraught with potential complications, primarily due to the delicate balance required between restoring stability and preserving functional range of motion. The most common complication is recurrent instability, which occurs in approximately 10% to 15% of open capsular shifts and can be even higher in arthroscopic plications, particularly in patients with underlying connective tissue hyperlaxity. Recurrence is often secondary to biological failure of the capsular tissue to heal to the humerus or progressive stretching of the inherently abnormal collagen matrix. Salvage management for recurrent MDI typically requires revision open capsular shift, often augmented with allograft tissue or an Eden-Hybbinette procedure if attritional bone loss has occurred during the recurrent dislocation episodes.
Conversely, over-constraint of the glenohumeral joint is a devastating complication resulting from technical errors during the capsular shift. If the surgeon tensions the capsular flaps with the arm in internal rotation, the patient will suffer a profound loss of external rotation. This obligate posterior translation of the humeral head during attempted external rotation leads to rapid, accelerated wear of the posterior glenoid cartilage, a condition termed capsulorrhaphy arthropathy. The incidence of clinically significant loss of motion ranges from 5% to 10%. Salvage requires prompt recognition and may necessitate arthroscopic capsular release to restore motion before irreversible chondral damage occurs.
Neurologic injury, specifically to the axillary nerve, is a catastrophic risk during the inferior capsular dissection. The axillary nerve runs in close proximity (often within 2 to 3 millimeters) to the inferior capsule at the 6 o'clock position. The incidence of transient neurapraxia is reported at 1% to 2%, while permanent transection is exceedingly rare but devastating. Meticulous surgical technique, specifically maintaining the arm in external rotation during inferior flap mobilization to drop the nerve away from the capsule, is essential for prevention. If a nerve injury is identified postoperatively, baseline EMG/NCS should be obtained at 6 weeks, with early exploration and nerve grafting indicated if no recovery is evident by 3 months.
| Surgical Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Strategy / Management |
|---|---|---|---|
| Recurrent Instability | 10% - 15% | Connective tissue disorder, poor compliance, inadequate initial shift | Revision open capsular shift, allograft augmentation, or bone block |
| Over-constraint (Loss of ER) | 5% - 10% | Tying flaps in internal rotation, excessive capsular imbrication | Aggressive physical therapy; arthroscopic anterior capsular release if refractory |
| Axillary Nerve Injury | 1% - 2% | Blind dissection inferiorly, failure to externally rotate arm during flap prep | Observation and EMG at 6 wks; early nerve exploration/grafting if no recovery |
| Subscapularis Failure | 2% - 4% | Poor tissue quality, aggressive early active internal rotation | Surgical repair of the tendon; pectoralis major transfer for chronic, retracted tears |
| Capsulorrhaphy Arthropathy | 3% - 5% | Chronic over-constraint, proud hardware (in Eden-Hybbinette) | Hardware removal, capsular release; Total Shoulder Arthroplasty in end-stage disease |
Phased Post-Operative Rehabilitation Protocols
The ultimate success of both the Eden-Hybbinette bone block procedure and the Neer Inferior Capsular Shift relies just as heavily on strict adherence to a phased, meticulously supervised postoperative rehabilitation protocol as it does on the surgical execution. The primary goal of rehabilitation is to protect the healing capsulolabral tissues and the subscapularis repair while simultaneously preventing the onset of adhesive capsulitis. Communication between the operating surgeon and the physical therapist is critical, particularly regarding the intraoperative "safe zones" of motion established after the capsular shift.
Phase I: Maximum Protection (Weeks 0-4)
Immediately postoperatively, the patient is placed in a dedicated shoulder immobilizer or a sling with a small abduction pillow. Strict immobilization is maintained for 4 weeks to allow for initial soft-tissue-to-bone healing at the humeral neck. During this phase, absolute protection of the anterior capsular repair and the subscapularis tenotomy is paramount. No active shoulder motion is permitted. However, active range of motion (ROM) of the elbow, wrist, and hand must be initiated immediately in the recovery room to prevent distal edema and stiffness. Cryotherapy is utilized aggressively to manage postoperative pain and inflammation.
Phase II: Early Protected Motion (Weeks 4-8)
At 4 weeks, the sling is gradually weaned for activities of daily living in a safe, controlled environment. The focus shifts to restoring passive and active-assisted range of motion. Gentle, passive forward flexion in the scapular plane is initiated, aiming for 90 degrees by week 6. External rotation is the most critical parameter to monitor; it is strictly limited to the intraoperative safe zone (typically 0 to 15 degrees) to prevent catastrophic stretching of the repaired anterior capsule and subscapularis. Submaximal, pain-free isometric exercises for the deltoid and rotator cuff may begin late in this phase, provided they do not stress the surgical repairs.
Phase III: Active Motion and Scapular Kinematics (Weeks 8-12)
As the biological healing of the capsule solidifies, active ROM exercises are fully integrated. External rotation stretching is progressively and carefully introduced, aiming for 30 to 40 degrees by week 10. A major focus of Phase III is the restoration of normal glenohumeral rhythm through rigorous scapular stabilization exercises. Strengthening of the rhomboids, middle/lower trapezius, and serratus anterior is critical, as scapular dyskinesia is a primary driver of recurrent instability in the MDI population. Closed kinetic chain exercises, such as wall slides and rhythmic stabilization, are excellent for enhancing joint proprioception.
Phase IV: Strengthening and Return to Function (Weeks 12-24+)
Isotonic strengthening exercises for the rotator cuff, deltoid, and periscapular musculature are advanced. Plyometric training, utilizing medicine balls and dynamic rebounders, is introduced between 4 to 5 months to restore explosive power and reactive neuromuscular control. Sport-specific training for overhead athletes (e.g., throwing programs, swimming mechanics) begins only when symmetrical strength is achieved and the patient demonstrates a negative apprehension test. Return to contact sports, heavy manual labor, or competitive overhead athletics is strictly restricted until 6 to 9 months postoperatively, contingent upon the surgeon's final clinical clearance and the restoration of full dynamic stability.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for multidirectional instability is deeply rooted in a few landmark publications that have shaped modern orthopedic practice. The foundational text remains Neer and Foster's 1980 publication in the Journal of Bone and Joint Surgery, which first conceptualized MDI as a distinct clinical entity separate from traumatic unidirectional instability. They elegantly described the inferior capsular shift, emphasizing the necessity of detaching the capsule from the humeral side to effectively obliterate the redundant inferior pouch without restricting rotational motion excessively. This humeral-based shift remains the gold standard for open management of severe MDI.
Subsequent biomechanical and clinical studies refined the understanding of the capsuloligamentous restraints. Harryman et al. (1992) provided critical biomechanical data demonstrating the role of the rotator interval in preventing inferior translation. Their work established the modern consensus that rotator interval closure is a mandatory adjunct to any capsular shift procedure for MDI. In the realm of soft-tissue modifications, Altchek et al. popularized the T-plasty modification of the Bankart procedure, which allowed for a glenoid-based capsular shift. While effective for anteroinferior instability, the humeral-based Neer shift is generally preferred for true, global multidirectional redundancy due to its superior ability to address the axillary pouch.
In recent years, the paradigm has shifted toward arthroscopic management. Authors such as Treacy, Savoie, and McIntyre have published extensive series demonstrating that arthroscopic pancapsular plication can yield clinical outcomes comparable to open capsular shifts, with the added benefits of decreased morbidity, preservation of the subscapularis, and improved cosmesis. However, current clinical guidelines from the American Academy of Orthopaedic Surgeons (AAOS) and major sports medicine societies maintain that open inferior capsular shift remains the procedure of choice for patients with profound, massive capsular redundancy, revision scenarios, or those with underlying collagen disorders.
For the subset of MDI patients who have developed attritional bone loss, the literature clearly supports bony augmentation. Provencher et al. have extensively documented the outcomes of distal tibial allografts, while classical studies by Warner and others continue to support the Eden-Hybbinette iliac crest autograft as the most biologically robust solution for critical anterior glenoid defects. The synthesis of this literature dictates a highly individualized approach: rigorous non-operative management first, followed by tailored surgical intervention—arthroscopic plication for mild-to-moderate redundancy, open Neer shift for massive global laxity, and Eden-Hybbinette for cases complicated by critical bone loss.
