SLAP Tears: Your Guide to Diagnosis & Treatment in Elbow Cases
Key Takeaway
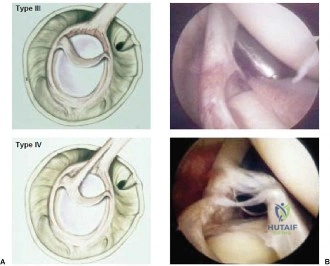
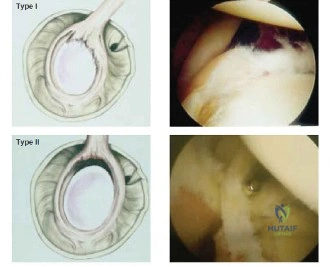
This topic focuses on SLAP Tears: Your Guide to Diagnosis & Treatment in Elbow Cases, After failed conservative management for shoulder SLAP tears, an MR arthrogram classifies the injury using Snyder criteria. For instance, Type II tears often require labrum repair in younger, unstable patients, or biceps tenodesis for older individuals. Such precise treatment decisions are crucial for optimal recovery in complex orthopaedic conditions, including specific elbow cases slap.
You are presented with a 21-year-old collegiate pitcher complaining of medial elbow pain and decreased velocity. He reports a "dead arm" and deep, vague shoulder pain. Clinical examination shows a 35-degree internal rotation deficit (GIRD) and a Type III scapular dyskinesis. How do you integrate these findings into a clinical diagnosis?
Candidate: The patient likely has a SLAP lesion causing secondary medial elbow overload. The shoulder pain and GIRD suggest the labrum is failing, which forces the pitcher to change their throwing mechanics—specifically "dropping the elbow"—to compensate for the shoulder pain. This increases the valgus torque on the elbow, leading to the medial symptoms.
Treating the elbow and shoulder as two separate, concurrent pathologies. Failing to acknowledge the "kinetic chain" or attempting to order an MRI of the elbow before a full shoulder examination is a red flag for the examiner.
The candidate demonstrates an understanding of "regional interdependence." They explain that the primary pathology is a proximal kinetic chain deficit (SLAP lesion). They note that the GIRD and scapular dyskinesis indicate a failure of the stabilizing structures, causing a biomechanical shift ("dropped elbow") that creates secondary symptomatic valgus stress on the UCL/medial complex. They conclude that the elbow is a "victim," not the "culprit."
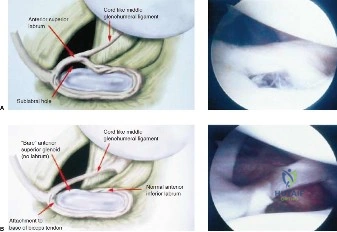
The MRA is performed. Look at the provided image. What key feature are we evaluating in this position, and what specific clinical phenomenon does it demonstrate?
Candidate: This is an MRA in the ABER (Abduction and External Rotation) position. It demonstrates the "peel-back" phenomenon where the superior labrum and biceps anchor shift medially and posteriorly over the glenoid rim during simulated late-cocking.
Failing to name the position (ABER) or failing to explain why the ABER position is used (it replicates the specific stress of the overhead throwing motion).
The candidate correctly identifies the ABER sequence and explains that it is the "gold standard" stress view for the superior labrum. They describe how this view reproduces the "peel-back" forces—where the biceps tendon, under tension in external rotation, creates a shear force that lifts the labrum from the glenoid, which is the pathomechanical basis for a Type II SLAP lesion in this population.
The patient has failed 6 months of conservative management. You are now in the OR. Describe your arthroscopic findings and how you would confirm the diagnosis.
Candidate: I would perform a diagnostic arthroscopy. I would use a probe to assess the superior labrum for instability. I would then perform the "peel-back" test by placing the arm in the ABER position under direct visualization to see the biceps anchor lifting off the glenoid.
Forgetting to mention the importance of debriding the glenoid rim to bleeding bone (creating a "biological bed") before anchor placement, which is essential for successful healing.
The candidate systematically outlines: 1. Inspection of the glenoid/labral complex. 2. Confirmation via the "peel-back" maneuver. 3. Meticulous preparation of the superior glenoid neck (decortication). 4. Use of a high anterior-superior portal (Port of Wilmington) to achieve the optimal "deadman’s angle" (45 degrees) for anchor placement, while specifically mentioning protection of the suprascapular nerve.
Why would you choose a SLAP repair over a biceps tenodesis in this specific patient?
Candidate: In an elite, young overhead athlete (21 years old), I prefer repair to preserve the length-tension relationship of the biceps. Tenodesis might alter his throwing mechanics and reduce his velocity, whereas a stable repair restores the native anatomy.
Suggesting tenodesis because "it's easier and has fewer complications." While true for a 40-year-old, it fails to recognize the specific biomechanical needs of a collegiate pitcher.
The candidate argues that in the elite pitcher, the long head of the biceps acts as a dynamic anterior/superior stabilizer. Tenodesis would remove this functional attachment, potentially altering the thrower's velocity and control. They successfully frame the surgical decision as one based on functional demand versus age-related degeneration.
