Management of Chronic Unreduced Glenohumeral Dislocations: A Comprehensive Surgical Guide
Key Takeaway
Chronic unreduced shoulder dislocations present a complex reconstructive challenge characterized by severe soft-tissue contractures, capsular bowstringing, and significant bony defects. Successful management requires meticulous preoperative planning with advanced imaging, careful neurolysis, and extensive capsular release. This guide details the pathoanatomy, biomechanical alterations, and step-by-step surgical techniques—including joint reduction and concurrent stabilization procedures—necessary to restore glenohumeral kinematics and optimize patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Old, unreduced dislocations of the glenohumeral joint represent one of the most formidable and technically demanding challenges in upper extremity orthopedic surgery. By strict orthopedic definition, a shoulder dislocation is classified as "chronic," "old," or "neglected" when it has remained unreduced for a period exceeding three to four weeks. This specific chronological threshold is not arbitrary; it directly correlates with the biological timeline of dense fibroblastic proliferation, capsular contracture, and the onset of irreversible osseous remodeling that absolute precludes safe closed reduction maneuvers. Attempting closed reduction beyond this window carries an unacceptably high risk of catastrophic iatrogenic complications, including surgical neck fractures of the humerus, avulsion of the brachial plexus, and rupture of the axillary artery.
Epidemiologically, chronic unreduced dislocations demonstrate a distinct bimodal distribution, reflecting two entirely different patient phenotypes and mechanisms of injury. The most frequent presentation occurs in the elderly population, specifically patients over the age of 65. In this demographic, the initial dislocation is typically an anterior instability event precipitated by a seemingly trivial mechanism, such as a low-energy fall from a standing height. The chronicity of the dislocation in these patients is often the result of delayed presentation, cognitive impairment, or a failure of the primary care provider to obtain adequate orthogonal radiographs. This susceptibility to dislocation and subsequent neglect is largely driven by advancing age, inherent muscular weakness, osteopenia, and progressive, preexisting degeneration of the dynamic static stabilizers, particularly massive, retracted rotator cuff tears involving the subscapularis and supraspinatus tendons.
Conversely, in the younger, higher-demand patient population, chronic unreduced dislocations are almost exclusively highly correlated with specific, severe comorbidities and high-energy mechanisms. These injuries most frequently manifest as posterior dislocations, which are notoriously missed during primary and secondary trauma surveys. They predominantly occur in individuals with a history of chronic alcoholism, uncontrolled seizure disorders (e.g., epilepsy, alcohol withdrawal seizures), or those who have sustained severe electrical shocks. The mechanism involves violent, uncoordinated, tetanic contractions of the shoulder musculature. Because the internal rotators (latissimus dorsi, pectoralis major, and subscapularis) vastly overpower the external rotators (infraspinatus and teres minor), the humeral head is forcefully driven posteriorly over the glenoid rim. Furthermore, polytrauma patients in the intensive care unit, particularly those with traumatic brain injuries or those requiring prolonged intubation, are at high risk for missed dislocations due to the inability to communicate pain and the logistical challenges of obtaining high-quality axillary radiographs in the supine, immobilized patient.
The clinical presentation of a chronic unreduced shoulder dislocation is classically characterized by intractable, mechanically induced pain and a profound, pathognomonic limitation of glenohumeral motion. Unlike the acute inflammatory pain seen immediately following a traumatic dislocation, the pain profile in a chronic setting is typically provoked by functional demands. At rest, the shoulder may be relatively asymptomatic once the initial hemarthrosis and acute capsular tearing have organized. However, any attempt by the patient to move the arm beyond its newly restricted, pathological arc of motion provokes severe discomfort secondary to mechanical impingement of the deformed osseous structures and extreme tension on the fibrotic joint capsule. Loss of motion is the chief clinical finding, and the specific pattern of restriction dictates the direction of the dislocation. Patients with old anterior dislocations exhibit a severe restriction in abduction and internal rotation, as the humeral head is locked anterior and medial to the glenoid. Conversely, patients with old posterior dislocations demonstrate a marked, unyielding restriction in abduction and external rotation; the arm is rigidly locked in internal rotation, and any examiner's attempt to externally rotate the humerus is met with a firm, mechanical bony block.
Detailed Surgical Anatomy and Biomechanics
The pathoanatomy of a chronic unreduced dislocation is characterized by profound, progressive, and often irreversible distortion of both the soft-tissue envelope and the osseous architecture of the shoulder girdle. Within a matter of weeks following the initial dislocation, a robust inflammatory cascade leads to the development of dense, unyielding fibrous and capsular contractures across the base of the glenoid and the surrounding fascial planes. The rotator cuff muscles, deprived of their normal resting physiological length and tension, undergo rapid fatty infiltration, severe contracture, and fibrosis. This fibrotic obliteration is not confined to the glenohumeral joint capsule; it frequently extends inferiorly and medially into the axillary space, aggressively enveloping critical neurovascular structures. The axillary artery and the axillary nerve become densely tethered within this scar tissue, drastically altering their normal anatomical trajectories and rendering them highly susceptible to traction injuries during surgical mobilization.
A critical biomechanical and pathoanatomical concept in the understanding of chronic dislocations is the capsular “bowstringing” phenomenon, classically described by Neviaser. In the setting of a prolonged dislocation, the native joint capsule becomes densely adherent to the empty, denuded articular surface of the glenoid fossa. This fibrotic obliteration of the joint space acts as an absolute physical barrier, preventing the humeral head from being reduced into its anatomical position even if the surrounding musculature is paralyzed under general anesthesia.

As illustrated in the classic Neviaser diagrams, the specific pattern of capsular adhesion is dictated by the direction of the dislocation. In an old anterior dislocation, the posterior capsule is pulled across the joint space and develops dense adhesions to the articular surface of the glenoid. Conversely, in an old posterior dislocation, it is the anterior capsule that becomes bowstrung and adherent to the glenoid surface. This necessitates a meticulous, complete 360-degree capsulectomy during surgical intervention to recreate the joint space.
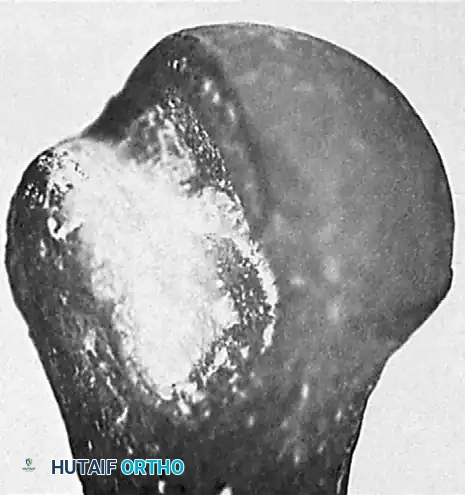
Concomitant with these severe soft-tissue contractures, the osseous architecture undergoes significant, destructive remodeling due to the chronic, abnormal articulation and the patient's continuous attempts to mobilize the locked joint. In chronic anterior dislocations, a massive impaction fracture occurs in the posterolateral aspect of the humeral head where it continuously grinds against the dense cortical bone of the anterior glenoid rim. Because of the repeated, forceful, and often desperate efforts of the patient to achieve normal motion, this osseous defect is substantially larger, deeper, and more morphologically complex than the classic Hill-Sachs lesion observed in recurrent, episodic anterior instability.
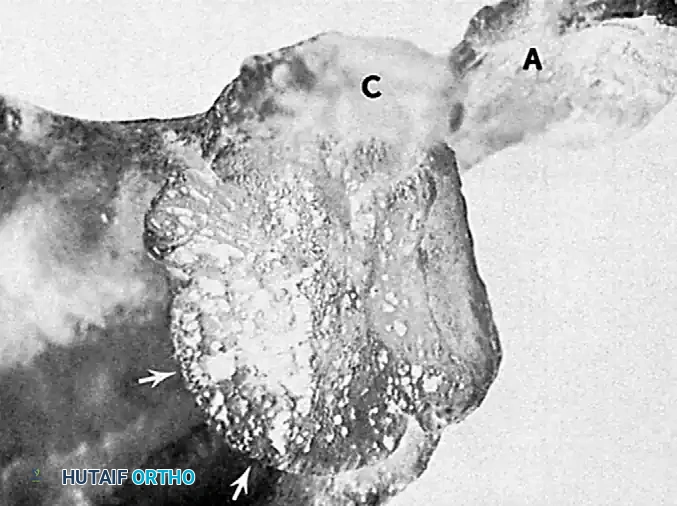
Furthermore, the constant friction, pressure, and abnormal load transmission lead to severe attrition, compression fractures, and volumetric bone loss of the apposing anterior glenoid rim. In long-standing, neglected cases, the biological response to this altered biomechanical state is the formation of a pseudoarticulation, or false joint, between the displaced humeral head and the anterior aspect of the scapular neck.
In chronic posterior dislocations, a similar but anatomically reversed bony lesion is encountered. This impaction fracture, often termed a "reverse Hill-Sachs" or McLaughlin lesion, is located on the anteromedial aspect of the humeral head and is caused by the relentless impingement of the posterior glenoid rim. Like their anterior counterparts, these reverse Hill-Sachs lesions are typically massive, often involving greater than 40% of the articular surface, rendering the joint highly unstable even if reduction is surgically achieved, thereby necessitating complex osseous reconstruction or prosthetic arthroplasty.
Exhaustive Indications and Contraindications
The decision-making process for the management of chronic unreduced glenohumeral dislocations requires a highly nuanced, individualized approach, balancing the patient's physiological age, functional demands, medical comorbidities, and the specific pathoanatomical characteristics of the bony and soft-tissue defects. Operative intervention is generally the standard of care for the vast majority of patients presenting with a chronic dislocation, as the natural history of a neglected dislocation is characterized by progressive, debilitating pain, profound functional impairment of the upper extremity, and eventual severe glenohumeral arthrosis. The primary goals of surgical intervention are the alleviation of mechanically induced pain, the restoration of a stable, concentric glenohumeral reduction, and the optimization of functional range of motion to allow the patient to perform activities of daily living.
However, surgical intervention is not universally indicated, and a strategy of "skillful neglect" or non-operative management may be the most prudent course of action in a highly selected subset of patients. This approach is typically reserved for elderly, low-demand, or medically frail patients who present with a truly chronic, long-standing dislocation (often unrecognized for many months or years) and who have developed a painless pseudoarticulation. If the patient has minimal pain at rest, possesses sufficient compensatory scapulothoracic motion to perform essential activities of daily living (such as feeding and basic hygiene), and has severe medical comorbidities that would make prolonged general anesthesia and major reconstructive surgery prohibitively dangerous, non-operative management is strongly advised. Attempting complex reconstruction in these specific scenarios often results in a stiff, painful shoulder that is functionally inferior to the patient's preoperative, adapted state.
When operative intervention is indicated, the specific surgical procedure selected—ranging from joint-preserving techniques to prosthetic arthroplasty—is dictated primarily by the chronicity of the dislocation, the quality of the surrounding soft-tissue envelope, and, most importantly, the size and location of the humeral head articular defect. Joint-preserving procedures, such as open reduction combined with transfer of the lesser tuberosity (modified McLaughlin procedure) or structural osteochondral allografting, are generally reserved for younger, high-demand patients with articular defects involving less than 30% to 40% of the humeral head. Conversely, in older patients, or in any patient presenting with massive articular defects exceeding 40% to 50% of the humeral head volume, severe glenoid bone loss, or an irreparably contracted and fatty-infiltrated rotator cuff, prosthetic replacement (hemiarthroplasty, anatomic total shoulder arthroplasty, or reverse total shoulder arthroplasty) becomes the mandatory reconstructive option.
| Clinical Parameter | Indications for Surgical Intervention | Contraindications (Absolute and Relative) |
|---|---|---|
| Patient Profile | Young, active, high-demand patients; Elderly patients with severe, intractable mechanical pain. | Absolute: Medically unstable for general anesthesia; Active joint infection. Relative: Low-demand elderly with a painless pseudoarthrosis. |
| Chronicity | Dislocation recognized between 3 weeks and 6 months; Progressive functional decline. | Relative: Dislocation > 1-2 years with established, painless false joint and adequate compensatory scapulothoracic motion. |
| Defect Size < 20-30% | Open reduction with soft-tissue stabilization; Lesser tuberosity transfer (McLaughlin). | Relative: Severe osteopenia precluding secure fixation of tuberosity transfer. |
| Defect Size 30-45% | Structural osteochondral allografting; Segmental reconstruction. | Relative: Advanced chronological age; Pre-existing severe glenohumeral osteoarthritis. |
| Defect Size > 45-50% | Prosthetic Arthroplasty (Hemiarthroplasty, aTSA, or rTSA depending on cuff status). | Absolute: Active Deltoid paralysis (for rTSA); Active axillary nerve palsy with no recovery potential. |
| Rotator Cuff Status | Intact or repairable cuff: Joint preservation or aTSA. Irreparable/Fatty infiltrated: rTSA. | Absolute: Attempting aTSA in the presence of an irreparable subscapularis or massive cuff tear. |
Pre-Operative Planning, Templating, and Patient Positioning
A complete, exhaustive, and meticulously detailed radiographic evaluation is the absolute cornerstone of preoperative planning for any chronic unreduced shoulder dislocation. The initial evaluation must include a high-quality, true anteroposterior (Grashey) view, a scapular Y view, and, most critically, an axillary lateral view of the shoulder. The axillary view is non-negotiable; it definitively confirms the direction of the dislocation, establishes the relationship of the humeral head to the glenoid, and provides the initial assessment of the size and depth of the impaction fracture (Hill-Sachs or reverse Hill-Sachs lesion). In the chronic setting, patients are often in significant pain and possess severely restricted motion, making a standard axillary view difficult or impossible to obtain. In such instances, a Velpeau axillary view—obtained with the patient leaning backward over the cassette while remaining in their sling—must be acquired.
While plain radiography provides the foundational diagnosis, advanced cross-sectional imaging in the form of Computed Tomography (CT), particularly with three-dimensional (3D) surface rendering and volumetric reconstruction techniques, is absolutely mandatory for definitive surgical planning. CT imaging is unparalleled in its ability to evaluate the complex, distorted bony anatomy, quantify the precise degree of glenoid bone loss and version alteration, and accurately measure the volumetric extent of the damage to the articular surface of the humeral head.
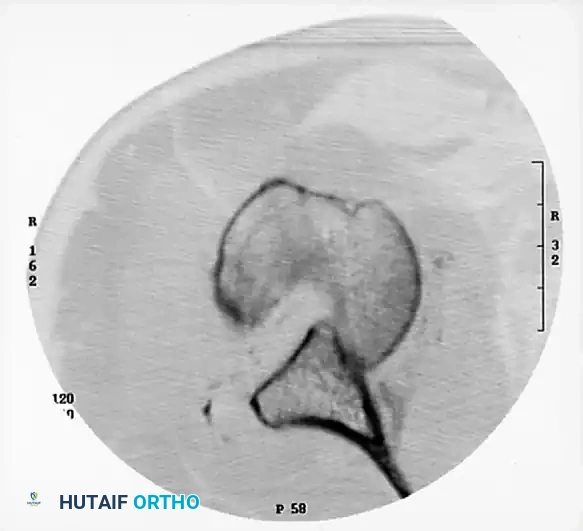
The degree of damage to the articular surface, as quantified on the preoperative CT scan, is the single major determining factor in the surgical procedure selected. Surgeons must calculate the percentage of articular involvement to decide between joint-preserving procedures (e.g., structural allograft reconstruction, transfer of the lesser tuberosity) and prosthetic arthroplasty. Furthermore, CT imaging allows for precise preoperative templating of prosthetic components, ensuring that the surgeon is prepared with the appropriate implant sizes, augmented glenoid baseplates, or custom components if severe, uncontained bone loss is identified. Magnetic Resonance Imaging (MRI) may be considered to evaluate the integrity and degree of fatty infiltration of the rotator cuff musculature; however, its utility is often limited by the distorted anatomy, dense fibrosis, and the fact that the decision to proceed with a reverse total shoulder arthroplasty (rTSA) is frequently made based on the bony destruction alone, regardless of cuff status in the elderly patient.
Patient positioning and the choice of anesthesia are critical components of the operative setup. The procedure is typically performed under general endotracheal anesthesia, supplemented with a preoperative ultrasound-guided interscalene regional nerve block. This multimodal analgesic approach not only provides excellent postoperative pain control but also facilitates intraoperative muscle relaxation, which is essential when attempting to mobilize a chronically contracted joint. However, the surgeon must ensure a thorough, documented preoperative neurological examination of the axillary and musculocutaneous nerves before the block is administered, as preexisting neuropraxias are common.
The patient is optimally placed in the modified beach-chair position, with the backrest elevated to approximately 45 to 60 degrees. This position affords the surgeon unhindered, extensile access to the anterior shoulder, the superior shoulder girdle, and the axilla. The affected arm is prepped and draped entirely free, allowing for full, unrestricted manipulation of the limb during the reduction maneuvers and trial reductions. A sterile Mayo stand or a dedicated mechanical arm positioner (e.g., SPIDER2 Limb Positioner) should be utilized to support the limb, allowing the surgical assistant to maintain precise traction and rotation during the delicate neurolysis and capsular release phases of the operation.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of chronic unreduced dislocations is a major, high-risk undertaking that demands meticulous anatomical knowledge and extreme patience. It must be reiterated that closed reduction should never be forcefully attempted in a truly chronic setting (>3-4 weeks). The fibrotic adhesions and capsular bowstringing render the joint mechanically locked; forceful manipulation will inevitably result in a catastrophic iatrogenic complication, such as a spiral fracture of the humeral shaft, a surgical neck fracture, or devastating avulsion of the axillary artery or brachial plexus cords.
The Extended Deltopectoral Approach
An extended deltopectoral approach is the universally accepted workhorse incision for the management of chronic anterior dislocations, and it is highly versatile for chronic posterior dislocations when arthroplasty is anticipated. A generous incision is made starting just superior to the coracoid process and extending distally along the deltopectoral groove toward the deltoid tuberosity. The cephalic vein is identified and, depending on the venous tributary anatomy, is typically retracted laterally with the deltoid muscle to preserve its primary venous drainage, although medial retraction with the pectoralis major is an acceptable alternative if lateral mobilization is excessively tethered. The clavipectoral fascia is sharply incised, and the conjoined tendon (short head of the biceps and coracobrachialis) is identified. In chronic cases, the normal areolar tissue in the subcoracoid space is completely obliterated by dense, vascular scar tissue. The conjoined tendon is gently retracted medially using a Richardson or Kolbel retractor, taking extreme care not to place excessive traction on the musculocutaneous nerve, which typically enters the coracobrachialis 3 to 5 centimeters distal to the coracoid tip.
Soft-Tissue Mobilization and Neurolysis
This phase represents the most critical and dangerous portion of the operation. Before any capsular release or reduction maneuver is attempted, the axillary nerve must be definitively identified and protected. The nerve is frequently displaced from its normal anatomical position, tethered by severe inferior capsular fibrosis, and draped over the displaced humeral head. A blind "tug test" on the axillary nerve in the axilla should be strictly avoided, as the tethered nerve is highly susceptible to traction neurapraxia. Instead, meticulous, sharp dissection is required to trace the nerve from its origin at the posterior cord, along the anterior surface of the subscapularis, and down to the inferior border of the capsule where it enters the quadrangular space.
Once the neurovascular structures are protected, the subscapularis tendon must be managed. In chronic dislocations, the subscapularis is severely contracted and shortened. Depending on the planned reconstruction and the degree of contracture, the surgeon may elect to perform a formal lesser tuberosity osteotomy (LTO), a subscapularis peel, or a coronal Z-lengthening. An LTO is often preferred as it provides excellent bone-to-bone healing upon repair and allows for robust mobilization. Following subscapularis reflection, the adherent capsule (Neviaser's bowstringing) must be systematically excised from the glenoid fossa. A complete, 360-degree capsular release, including a thorough inferior capsulectomy off the surgical neck of the humerus, is almost always necessary to sufficiently mobilize the humeral head and recreate the native joint space.
Bony Reconstruction and Joint Reduction
Once the soft tissues are fully mobilized and the glenoid fossa is cleared of all fibrotic tissue, the humeral head is gently levered into the anatomical position using a combination of longitudinal traction and a bone skid or Darrach retractor. Forceful leverage must be avoided to prevent iatrogenic fractures of the osteopenic humeral head or the glenoid rim. Following reduction, the stability of the joint is dynamically assessed. If the humeral head impaction defect (Hill-Sachs or reverse Hill-Sachs) is small (<20%), the joint may be stable after reduction and capsulorrhaphy.
However, if a large, engaging defect is present, it must be definitively addressed to prevent immediate postoperative re-dislocation. For defects between 20% and 40% in younger patients, joint-preserving options include structural osteochondral allografting of the defect (to restore the spherical contour of the humeral head) or the modified McLaughlin procedure (transferring the lesser tuberosity and subscapularis tendon into the reverse Hill-Sachs defect to render it extra-articular). In older patients, or in cases of massive articular destruction (>40-50%), profound glenoid wear, or irreparable rotator cuff tearing, prosthetic arthroplasty is indicated. In the modern era, Reverse Total Shoulder Arthroplasty (rTSA) has become the gold standard for chronic unreduced dislocations in the elderly, as it reliably restores stability and functional motion by bypassing the compromised rotator cuff and utilizing the deltoid as the primary elevator, while concurrently addressing the severe glenoid bone loss with augmented baseplates or bone grafting techniques.
Management of Concomitant Shoulder Girdle Trauma
In patients who have sustained high-energy polytrauma, chronic shoulder dislocations may be accompanied by other neglected, unreduced injuries of the shoulder girdle, such as chronic acromioclavicular (AC) joint disruptions or distal clavicle fractures. If concurrent reconstruction of the AC complex is indicated during the same anesthetic event to restore the superior suspensory complex of the shoulder, modern suspensory fixation techniques are employed. The distal clavicle remnant is reduced, and the coracoclavicular interval is restored using a cortical suspensory device (e.g., an EndoButton construct, Smith & Nephew, Andover, MA). To provide biological augmentation to this mechanical fixation, a modified Weaver-Dunn technique is often performed, wherein the coracoacromial ligament is transferred to the resected end of the clavicle and secured with heavy, non-absorbable sutures to the suspensory construct, ensuring long-term stability of the shoulder girdle.
Complications, Incidence Rates, and Salvage Management
The prognosis for patients undergoing surgical reconstruction of chronic unreduced dislocations is inherently guarded when compared to those treated for acute injuries. Patients and their families must be extensively counseled preoperatively that a return to a completely "normal," pain-free shoulder with full, symmetrical range of motion is highly unlikely, regardless of the surgical technique employed. The primary objectives are the restoration of stability, the mitigation of intractable pain, and the achievement of functional, overhead motion sufficient for activities of daily living. The extensive soft-tissue dissection, the prolonged period of joint immobilization, and the altered biomechanics predispose these patients to a unique and challenging set of postoperative complications.
The most ubiquitous complication following open reduction of a chronic dislocation is severe postoperative stiffness. This is an almost inevitable consequence of the extensive scar tissue formation, the necessary capsular reconstruction, and the mandatory period of postoperative immobilization required to protect the soft-tissue repairs or tuberosity osteotomies. Avascular Necrosis (AVN) of the humeral head is another devastating complication, with a significantly elevated risk profile in chronic cases. The AVN is multifactorial, resulting from the initial traumatic insult to the intraosseous blood supply, the prolonged abnormal pressure on the articular cartilage, and the extensive surgical soft-tissue stripping—particularly the disruption of the anterior humeral circumflex artery—required to achieve reduction.
Neurological injury, specifically transient or permanent neurapraxia of the axillary or musculocutaneous nerves, can occur in up to 30% of cases despite meticulous surgical technique and direct visualization. This is primarily due to the chronic traction placed on the nerves during the dislocated state and the unavoidable tension applied during the surgical reduction maneuvers. Finally, progressive glenohumeral arthrosis is a near certainty in cases where joint-preserving techniques are chosen for long-standing dislocations, as the articular cartilage suffers irreversible hypoxic and mechanical damage during the unreduced period, often necessitating future conversion to prosthetic arthroplasty.
| Complication | Estimated Incidence Rate | Etiology / Risk Factors | Salvage Management / Treatment Strategy |
|---|---|---|---|
| Postoperative Stiffness | 40% - 60% | Extensive capsular fibrosis; Prolonged immobilization; Non-compliance with rehab. | Aggressive physical therapy; Intra-articular corticosteroid injections; Arthroscopic or open capsular release (after 6-12 months). |
| Avascular Necrosis (AVN) | 10% - 25% | Disruption of anterior humeral circumflex artery; Extensive soft-tissue stripping; Chronicity > 3 months. | Observation if asymptomatic; Core decompression (early stages); Conversion to anatomic or reverse Total Shoulder Arthroplasty (late stages with collapse). |
| Neurological Injury (Axillary Nerve) | 15% - 30% | Chronic tethering in axillary scar tissue; Iatrogenic traction during reduction maneuvers. | Baseline EMG at 6 weeks if no clinical improvement; Observation for 3-6 months; Nerve exploration, neurolysis, or nerve transfer (e.g., Somsak procedure) if no recovery. |
| Recurrent Instability | 5% - 15% | Failure to address large engaging bone defects; Insufficient capsulorrhaphy; Non-compliant early motion. | Revision stabilization (Latarjet, structural allograft); Conversion to Reverse Total Shoulder Arthroplasty to provide inherent mechanical stability. |
| Progressive Arthrosis | 50% - 80% (in joint preservation) | Irreversible chondral damage during dislocated state; Altered joint kinematics. | NSAIDs, activity modification, injections; Eventual conversion to prosthetic arthroplasty when symptoms become debilitating. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following the surgical management of a chronic unreduced dislocation is a delicate, highly customized tightrope walk. The physical therapist and the surgeon must constantly balance the critical need for biological tissue healing—protecting the subscapularis repair, the lesser tuberosity osteotomy, or the joint capsule—with the urgent necessity of preventing recurrent, debilitating stiffness, which is the most common complication in this patient cohort. The protocol is heavily dictated by the specific surgical procedure performed (e.g., joint preservation vs. rTSA) and the intraoperative stability of the reconstruction.
Phase I: Protection and Restricted Motion (Weeks 0 to 4)
Immediately postoperatively, the arm is strictly immobilized in a secure, well-padded sling or a dedicated shoulder immobilizer with an abduction pillow, depending on the tension of the repair. This immobilization is maintained continuously for 3 to 4 weeks. During this critical protective phase, normal, active use of the elbow, wrist, and hand is strongly encouraged and mandatory to prevent distal joint stiffness, mitigate edema, and reduce the risk of developing complex regional pain syndrome (CRPS). The sling is removed only for strictly supervised, gentle, gravity-assisted pendulum exercises and for personal hygiene. Active shoulder motion, lifting, and any forceful pushing or pulling are strictly prohibited to protect the delicate soft-tissue repairs and osseous integration.
Phase II: Early Controlled Motion (Weeks 4 to 8)
At the 4-week mark, assuming radiographic evidence of stable fixation and appropriate clinical healing, the sling is gradually discontinued. The patient transitions into Phase II, which focuses on the restoration of passive range of motion (PROM) and the initiation of active
