
Comprehensive Introduction and Patho-Epidemiology
Glenohumeral instability represents a significant biomechanical failure of the shoulder's complex static and dynamic stabilizing mechanisms. The shoulder is the most commonly dislocated major joint of the human body, accounting for up to 45% of all joint dislocations encountered in emergency and orthopedic practice. The inherent mobility of the glenohumeral joint, characterized by a large spherical humeral head articulating with a relatively shallow, retroverted, and small glenoid fossa, predisposes it to instability when subjected to supraphysiologic forces. This delicate balance between mobility and stability is often summarized by the "golf ball on a tee" analogy, which underscores the joint's reliance on soft tissue constraints rather than osseous congruity for its fundamental stability.

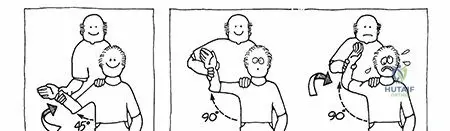
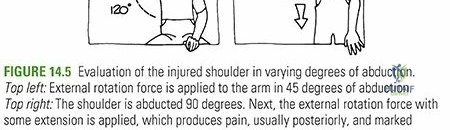
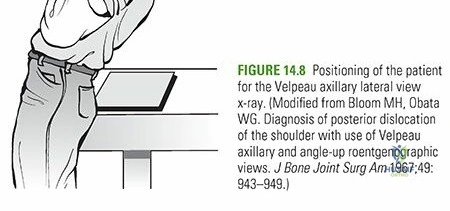
Anterior dislocations are overwhelmingly the most frequent, accounting for approximately 96% of all documented cases. The classic mechanism of injury involves a forced extension, abduction, and external rotation moment applied to the upper extremity, which levers the humeral head out of the glenoid fossa, catastrophically loading the anteroinferior capsuloligamentous complex. Posterior dislocations represent the second most common direction, comprising 2% to 4% of cases. These are classically associated with intense, uncoordinated muscle contractions seen in seizure disorders, electrical shock, or high-energy axial loading of an adducted, flexed, and internally rotated arm. Inferior dislocations, clinically termed luxatio erecta, and true superior shoulder dislocations are exceedingly rare, accounting for approximately 0.5% of documented cases, and often present with the patient's arm locked in extreme abduction with a high incidence of concomitant neurovascular compromise.
The overall incidence of glenohumeral dislocation is approximately 17 to 24 per 100,000 population per year, though this varies significantly based on the demographic studied. Epidemiological data demonstrates a distinct bimodal distribution that dictates both the pathoanatomy of the injury and the subsequent treatment algorithm. The primary incidence peak occurs in young males in the 15 to 30-year age range, predominantly driven by high-energy athletic trauma, collision sports (such as rugby, American football, and hockey), and military training. A secondary peak is observed in females in the 61 to 80-year age range, typically resulting from low-energy falls from a standing height. In this older demographic, the dislocation is frequently accompanied by a rotator cuff tear rather than a capsulolabral avulsion, fundamentally altering the surgical approach.

The natural history of glenohumeral dislocation is heavily dictated by the patient's age at the time of the initial event, their activity level, and the presence of underlying ligamentous laxity. The overall recurrence rate across all age groups is approximately 50%. However, this rate rises dramatically to nearly 89% in the 14 to 20-year age demographic when treated non-operatively. This unacceptably high recurrence rate in young, high-demand athletes frequently necessitates early surgical intervention to restore capsulolabral integrity, prevent progressive glenoid bone loss, and mitigate the risk of long-term dislocation arthropathy.
Pathoanatomy of Anterior Shoulder Instability
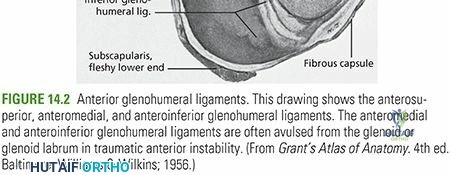
The pathoanatomy of anterior shoulder instability involves a predictable cascade of structural failures within the anteroinferior capsulolabral complex. Dislocation requires stretching, plastic deformation, avulsion, or frank tearing of the joint capsule and its ligamentous thickenings. The classic "Bankart lesion" is the sine qua non of anterior instability, referring to the avulsion of the anteroinferior labrum and its attached inferior glenohumeral ligament (IGHL) complex from the anterior glenoid rim. This lesion abolishes the concavity compression effect and is identified in up to 90% of traumatic anterior dislocations undergoing surgical stabilization. When the avulsion includes an osteochondral fracture of the anterior glenoid rim, it is termed a "bony Bankart" lesion, which critically reduces the articular surface area and predisposes the joint to recurrent instability even with minimal provocative forces.
Beyond the classic Bankart lesion, several morphological variants exist that the orthopedic surgeon must meticulously recognize during diagnostic arthroscopy. The Anterior Labroligamentous Periosteal Sleeve Avulsion (ALPSA) lesion involves the medial displacement and inferior healing of the labroligamentous complex along the scapular neck. Unlike a standard Bankart lesion, the ALPSA lesion retains an intact, albeit stripped, periosteal sleeve. Failure to recognize and adequately mobilize an ALPSA lesion back to the anatomical glenoid rim results in high recurrence rates due to non-anatomical healing and persistent capsular volume expansion.

Other recognized pathoanatomic entities include the Perthes lesion, wherein the labrum is detached from the glenoid rim but the periosteal sleeve remains intact and the labrum is not medially displaced. This creates a functional incompetence of the labrum that is often difficult to visualize without aggressive probing, as it may appear anatomically reduced in the resting state. The Glenolabral Articular Disruption (GLAD) lesion involves a superficial tear of the anteroinferior labrum associated with an articular cartilage injury of the adjacent glenoid. Unlike Bankart variants, GLAD lesions typically present with deep, aching pain rather than frank clinical instability. Furthermore, the capsuloligamentous complex may occasionally fail at its humeral insertion, resulting in a Humeral Avulsion of the Glenohumeral Ligament (HAGL lesion), which must be specifically evaluated on preoperative MRI and during arthroscopy.

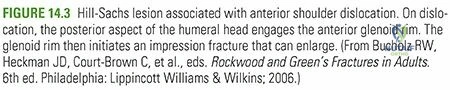
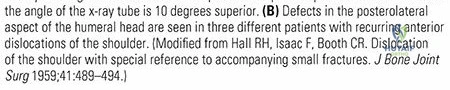
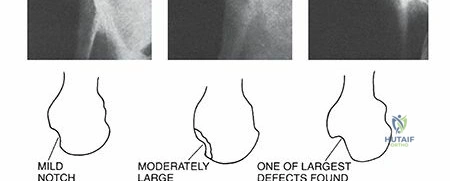
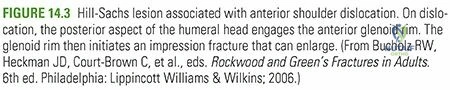
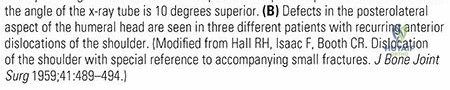
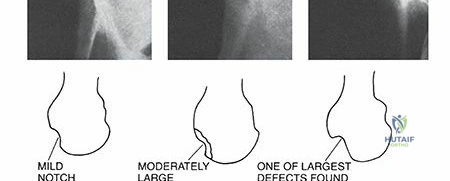
The Hill-Sachs lesion is a critical, obligate component of the pathoanatomic cascade in anterior instability. It is a compression fracture of the posterolateral humeral head created when the dislocated humeral head impacts and engages the hard, cortical anterior glenoid rim. This defect is radiographically evident in 27% of acute first-time anterior dislocations and up to 74% to 100% of recurrent anterior dislocations. The size, depth, and orientation of the Hill-Sachs lesion, particularly in relation to the glenoid track, dictate whether the lesion will engage the anterior glenoid rim during functional ranges of motion, thereby necessitating specific surgical interventions such as a Remplissage procedure.

Detailed Surgical Anatomy and Biomechanics
A profound and nuanced comprehension of glenohumeral anatomy and biomechanics is the absolute prerequisite for understanding complex instability patterns and executing effective, durable surgical stabilization. The glenohumeral joint relies on a sophisticated, synergistic interplay of static and dynamic stabilizers to maintain concentric reduction throughout an expansive, multi-planar arc of motion.
Osseous Anatomy and the Bipolar Bone Loss Paradigm
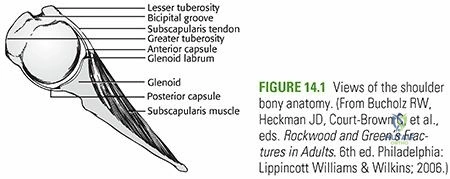
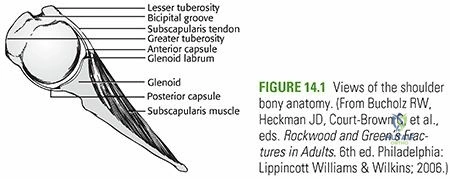
The articular surface of the glenoid is classically described as pear-shaped or inverted comma-shaped, being significantly wider inferiorly than superiorly. The "bare area" of the glenoid represents the central region of thinning articular cartilage, which serves as a critical intraoperative landmark for determining the center of the glenoid and calculating anterior bone loss. The glenoid typically exhibits slight retroversion relative to the scapular body (average 1 to 2 degrees) and slight superior inclination. The humeral head, conversely, is retroverted approximately 30 degrees relative to the transepicondylar axis of the distal humerus, with a neck-shaft angle averaging 135 degrees.
The concept of the "glenoid track," popularized by Yamamoto and Itoi, has revolutionized contemporary instability management by introducing a dynamic biomechanical framework for evaluating bipolar bone loss. The glenoid track represents the contact zone of the glenoid on the posterior humeral head as the arm is elevated in maximum external rotation and extension—the classic position of apprehension. The width of this track is calculated as 83% of the intact anterior-to-posterior width of the inferior glenoid. If a Hill-Sachs lesion extends medially beyond the medial margin of this track, it will "engage" the anterior glenoid rim during functional abduction and external rotation, levering the humeral head out of the joint. This is termed an "off-track" lesion. Conversely, if the Hill-Sachs lesion remains entirely within the boundaries of the track, it is an "on-track" lesion and will not engage, allowing for isolated capsulolabral repair.
Static Stabilizers of the Glenohumeral Joint
The static stabilizers include the articular congruity, the glenoid labrum, the capsuloligamentous complex, and negative intra-articular pressure. The labrum is a fibrocartilaginous ring that deepens the relatively flat glenoid fossa by approximately 50% (from 2.5 mm to 5 mm). More importantly, it significantly enhances joint stability through the mechanism of concavity compression, acting as a "chock block" that resists translational forces applied to the humeral head. Loss of the labrum, as seen in a Bankart lesion, reduces the resistance to anterior translation by up to 20%.

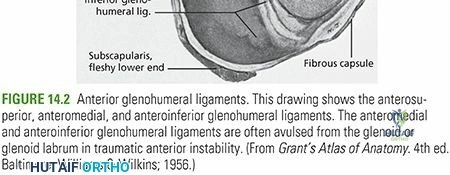
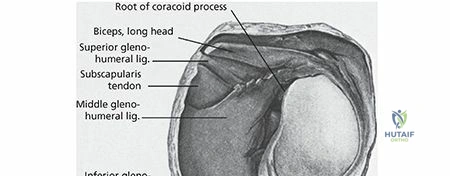
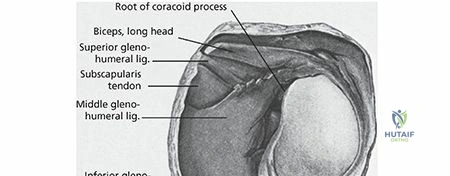
The capsuloligamentous complex consists of discrete, anatomically consistent thickenings of the joint capsule:
1. Superior Glenohumeral Ligament (SGHL): Originates from the supraglenoid tubercle anterior to the biceps tendon and inserts on the fovea capitis. It is the primary restraint to inferior translation in the adducted arm.
2. Middle Glenohumeral Ligament (MGHL): Originates from the anterosuperior labrum and inserts on the medial aspect of the lesser tuberosity. It primarily resists anterior translation in the mid-range of abduction (45 degrees). It exhibits significant anatomical variance, most notably the Buford complex, characterized by an absent anterosuperior labrum and a thick, cord-like MGHL. Misinterpreting a Buford complex as a detached labrum and surgically fixing it to the anterior glenoid rim will result in severe, iatrogenic loss of external rotation.
3. Inferior Glenohumeral Ligament (IGHL) Complex: The most critical static stabilizer. It consists of an anterior band, a posterior band, and an intervening axillary pouch. The IGHL acts like a hammock; as the arm is abducted and externally rotated, the anterior band becomes taut, serving as the primary restraint to anterior and inferior translation. Conversely, in internal rotation, the posterior band becomes the primary restraint to posterior translation.
Dynamic Stabilizers and Neuromuscular Control
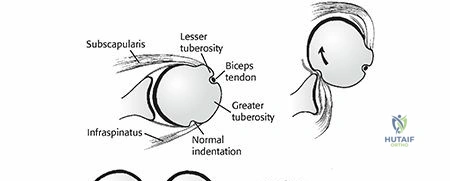
Dynamic stability is primarily conferred by the coordinated contraction of the rotator cuff musculature, the long head of the biceps tendon, and the periscapular muscles. The rotator cuff (supraspinatus, infraspinatus, teres minor, and subscapularis) compresses the humeral head concentrically into the glenoid fossa throughout the arc of motion. This active concavity compression is the most vital dynamic stabilizing mechanism of the shoulder.
The subscapularis dynamically supports the anterior capsule, tightening during external rotation to provide an active barrier against anterior translation. The infraspinatus and teres minor perform a similar function posteriorly. Furthermore, the periscapular musculature (trapezius, serratus anterior, rhomboids, and levator scapulae) ensures proper spatial positioning of the glenoid beneath the moving humeral head. This scapulohumeral rhythm maintains an optimal base of support, ensuring that the net joint reaction force remains directed within the confines of the glenoid fossa during complex upper extremity kinematics.
Exhaustive Indications and Contraindications
The decision-making process for managing glenohumeral instability is highly nuanced, requiring a careful, algorithmic analysis of patient demographics, physiological age, sport-specific demands, structural soft-tissue pathology, and, most critically, the precise quantification of bipolar bone loss. The Instability Severity Index Score (ISIS), developed by Balg and Boileau, remains a valuable preoperative tool, incorporating age, sport participation, type of sport, hyperlaxity, and radiographic bone loss to predict the risk of recurrence following isolated arthroscopic Bankart repair.
Historically, "critical" anterior glenoid bone loss was defined as >20-25% of the inferior glenoid width, serving as an absolute indication for bony augmentation procedures (e.g., Latarjet). However, contemporary literature has shifted this paradigm, demonstrating unacceptably high failure rates in isolated soft-tissue repairs with "subcritical" bone loss (13.5% to 15%). Consequently, the threshold for osseous reconstruction has been lowered, particularly in young, high-demand collision athletes.
Operative Versus Non-Operative Management Parameters
| Clinical Scenario | Recommended Management Strategy | Rationale and Biomechanical Considerations |
|---|---|---|
| First-Time Dislocation (Age > 30, Low Demand) | Non-Operative Management | Lower recurrence rate; initial trial of immobilization followed by dynamic stabilization rehabilitation is the standard of care. |
| First-Time Dislocation (Age < 20, Collision Athlete) | Early Operative Stabilization | Exceptionally high recurrence rate (>80%); early repair prevents progressive capsulolabral attenuation, cumulative glenoid bone loss, and further chondral damage. |
| Recurrent Anterior Instability (On-Track, Minimal Bone Loss <10%) | Arthroscopic Bankart Repair | Restoration of capsulolabral anatomy is highly successful when bone stock is preserved and the Hill-Sachs lesion is non-engaging. |
| Recurrent Instability with Subcritical Bone Loss (10-15%) and Off-Track Hill-Sachs | Arthroscopic Bankart Repair with Remplissage | Remplissage converts an off-track lesion to an on-track lesion by tenodesing the infraspinatus into the defect, preventing engagement without the morbidity of a bone block. |
| Recurrent Instability with Critical Bone Loss (>15-20%) or Failed Soft Tissue Repair | Latarjet Procedure or Free Bone Block Augmentation | Soft tissue repair will inevitably fail due to loss of the osseous articular arc. The Latarjet provides a triple-blocking effect (bone, sling, capsule). |
| Dislocation with Concomitant Rotator Cuff Tear (Age > 40) | Operative Repair of Cuff and Capsule | The primary pathology driving instability in this demographic is the loss of dynamic concavity compression; cuff repair is paramount. |

Contraindications to surgical intervention must be strictly observed to prevent catastrophic outcomes. Absolute contraindications include active joint infection, severe medical comorbidities precluding anesthesia, and voluntary, habitual dislocators with underlying psychiatric disorders who can dislocate their shoulders without provocation. Relative contraindications include poorly controlled seizure disorders (unless massive bony augmentation is planned), profound multidirectional instability primarily driven by connective tissue disorders (e.g., Ehlers-Danlos syndrome) where capsular plication tends to stretch out, and severe glenohumeral osteoarthritis (dislocation arthropathy), which may necessitate arthroplasty rather than stabilization.

Pre-Operative Planning, Templating, and Patient Positioning
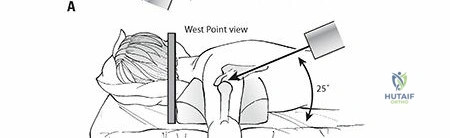
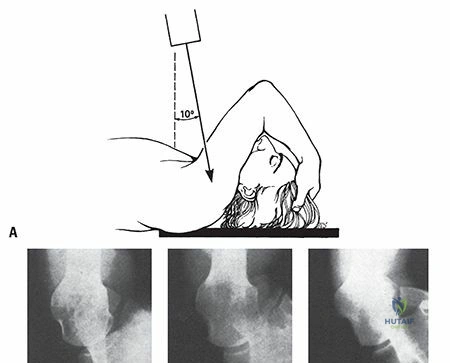
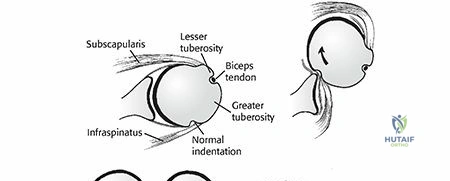
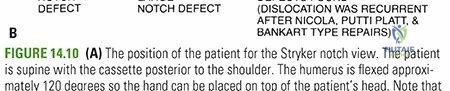
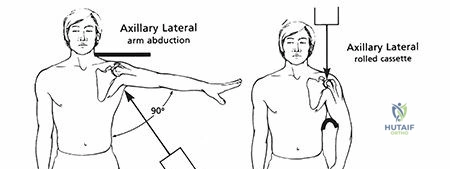
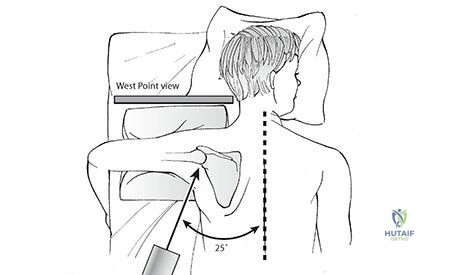
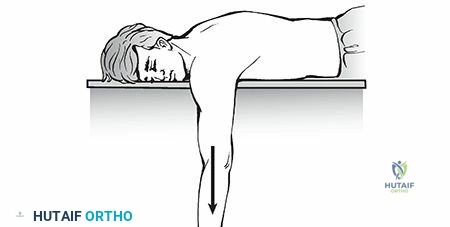
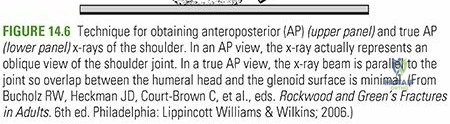
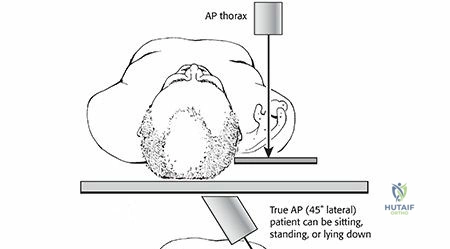
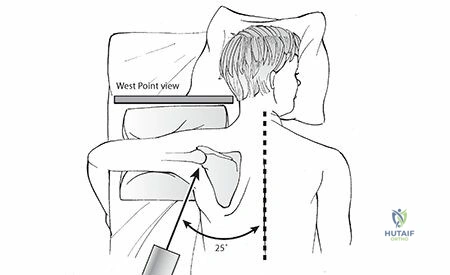
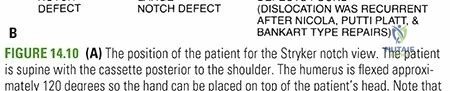
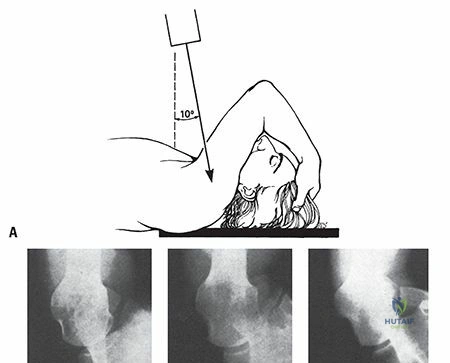
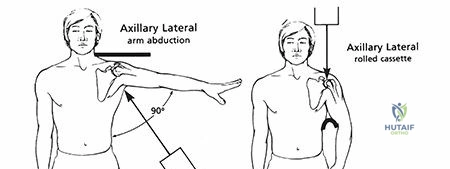
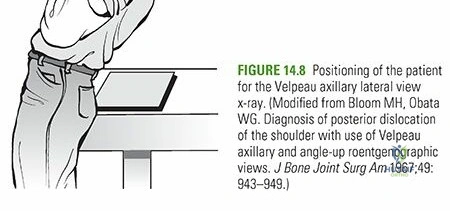
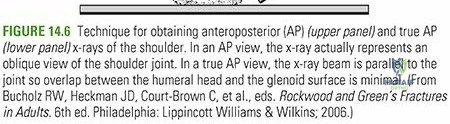
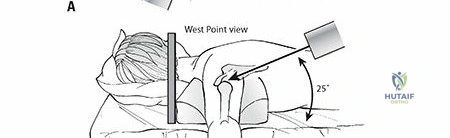
Pre-operative planning is the cornerstone of successful instability surgery. A comprehensive radiographic evaluation is mandatory. The standard trauma series includes a true anteroposterior (Grashey) view, a trans-scapular Y view, and an axillary lateral view. To specifically evaluate for osseous defects, specialized views are employed: the West Point axillary view optimally profiles the anteroinferior glenoid rim to detect bony Bankart lesions and attrition, while the Stryker Notch view profiles the posterolateral humeral head to identify and quantify Hill-Sachs lesions.
Advanced imaging is essential for surgical templating. Magnetic Resonance Imaging (MRI), preferably MR Arthrography (MRA) with intra-articular gadolinium, is the gold standard for evaluating the capsuloligamentous complex, identifying labral tears, ALPSA/GLAD/HAGL lesions, and assessing the integrity of the rotator cuff. However, for precise quantification of bone loss, a non-contrast Computed Tomography (CT) scan with 3D sagittal en face reconstructions with digital subtraction of the humeral head is mandatory.

Bone loss is typically calculated using the Pico method or the best-fit circle method on the 3D CT en face view. A perfect circle is drawn over the inferior, intact portion of the glenoid, utilizing the posterior and inferior margins as references. The amount of missing anterior bone is calculated as a percentage of the total circle diameter. Simultaneously, the width of the Hill-Sachs lesion is measured, and the glenoid track is calculated to determine the on-track/off-track status, dictating the ultimate surgical procedure.
Patient Positioning and Anesthesia
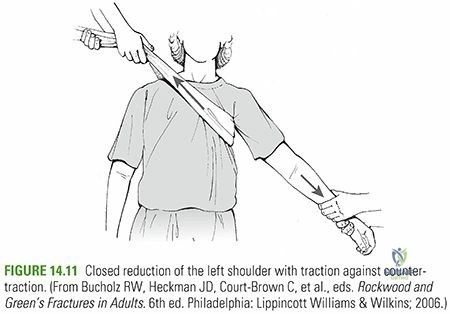
Surgical stabilization can be performed in either the beach chair or lateral decubitus position, largely dependent on surgeon preference, though each offers distinct biomechanical advantages. The lateral decubitus position utilizes longitudinal and lateral traction (typically 10-15 lbs), which significantly expands the glenohumeral joint space. This provides unparalleled visualization of the inferior capsule and the 6 o'clock position on the glenoid, facilitating optimal inferior anchor placement and aggressive capsular plication.
Conversely, the beach chair position places the patient in a semi-upright posture (typically 45 to 60 degrees). This orientation provides a more anatomical perspective of the shoulder, allows for unrestricted manipulation of the arm through a full range of motion to dynamically test stability intraoperatively, and permits seamless conversion to an open procedure (e.g., open Latarjet) without the need for repositioning. Regardless of position, regional anesthesia via an interscalene nerve block, combined with general anesthesia, is employed to provide profound muscle relaxation and optimal postoperative pain control.

Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of glenohumeral stabilization demands meticulous attention to soft tissue tensioning and precise hardware placement. The arthroscopic Bankart repair remains the workhorse procedure for patients with on-track lesions and preserved bone stock.
Arthroscopic Bankart Repair and Capsular Plication
Diagnostic arthroscopy is initially performed via a standard posterior viewing portal. The joint is systematically evaluated for labral pathology, chondral damage, and the presence of a HAGL lesion. An anterosuperior portal (rotator interval) and an anteroinferior portal (just superior to the subscapularis tendon) are established under direct visualization using outside-in spinal needle localization.

The first critical step is the aggressive mobilization of the torn capsulolabral complex. Using an arthroscopic elevator and tissue liberator, the labrum and the underlying capsule are freed from the anterior glenoid neck down to the 6 o'clock position. The tissue must be mobilized until the subscapularis muscle belly can be visualized anteriorly, ensuring that the capsule can be shifted superiorly and laterally without tension. The anterior glenoid rim is then decorticated using a motorized burr or rasp to create a bleeding cancellous bone bed, optimizing biological healing.
Suture anchors (typically 1.5 mm to 2.9 mm, knotless or knotted, composed of biocomposite or all-suture material) are sequentially placed on the glenoid rim. The first anchor is placed at the most inferior aspect of the tear, usually at the 5:30 position (in a right shoulder). The anchor must be placed exactly on the articular margin, angled at 45 degrees to the articular surface to maximize pullout strength and avoid penetrating the articular cartilage. A suture passing device (e.g., curved spectrum or penetrating grasper) is used to pass the suture through the capsule and labrum, taking a substantial bite of tissue inferior to the anchor to effect a superior-lateral capsular shift. This process is repeated with 2 to 3 additional anchors moving superiorly up to the 2 o'clock position. The sutures are tied or tensioned, recreating the anterior bumper and restoring the concavity compression.
The Remplissage Procedure
If an off-track Hill-Sachs lesion is identified in the setting of subcritical bone loss, a Remplissage (French for "to fill") procedure is performed concomitantly. Viewing from the anterior portal, the arthroscope is directed into the subacromial space, and the posterior capsule and infraspinatus tendon are visualized overlying the Hill-Sachs defect. One or two suture anchors are placed into the depths of the decorticated Hill-Sachs lesion. The sutures are passed through the posterior capsule and infraspinatus tendon. Once tied, this tenodesis effectively renders the defect extra-articular, preventing it from engaging the anterior glenoid rim during external rotation.
The Latarjet Procedure
For patients with critical bone loss (>15-20%), failed prior soft tissue stabilization, or high-demand collision athletes with significant structural damage, the Latarjet procedure is the gold standard. This involves the transfer of the coracoid process, along with its attached conjoint tendon (short head of the biceps and coracobrachialis), to the anteroinferior glenoid neck.

The procedure is typically performed open via a deltopectoral approach, though arthroscopic techniques are increasingly utilized by advanced surgeons. The coracoid is osteotomized at its base, yielding a bone graft approximately 2.5 to 3 cm in length. The inferior surface of the coracoid is decorticated to expose cancellous bone. The subscapularis tendon is split longitudinally at the junction of its middle and inferior thirds to expose the anterior shoulder capsule, which is incised vertically.
The anterior glenoid neck is prepared flat. The coracoid graft is passed through the subscapularis split and fixed to the anteroinferior glenoid (between the 2 and 5 o'clock positions) flush with the articular cartilage, typically using two 3.5 mm or 3.75 mm cannulated screws. The Latarjet provides a profound "triple-blocking" effect:
1. Bone Block Effect: Restores the osseous articular arc of the glenoid.
2. Sling Effect: The conjoint tendon acts as a dynamic sling across the anteroinferior capsule when the arm is abducted and externally rotated.
3. Capsular Repair: The native capsule is repaired to the stump of the coracoacromial ligament attached to the graft, restoring static restraint.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following glenohumeral stabilization occur and can profoundly impact patient outcomes. The surgeon must be adept at recognizing and managing these complex scenarios.

Recurrence of instability is the most common complication
Clinical & Radiographic Imaging Archive












Detailed Chapters & Topics
Dive deeper into specialized chapters regarding glenohumeral-dislocation