Management of Chronic Unreduced Shoulder Dislocations: A Comprehensive Surgical Guide

Key Takeaway
The management of chronic unreduced shoulder dislocations requires a highly individualized approach, balancing patient functional demands with complex pathoanatomy. Treatment options range from benign neglect in low-demand patients to complex open reduction, tendon transfers, and arthroplasty. Successful intervention demands a thorough understanding of capsular contractures, humeral head impression defects, and altered neurovascular anatomy to restore glenohumeral stability and optimize functional outcomes.
Comprehensive Introduction and Patho-Epidemiology
The management of a chronic, unreduced dislocation of the glenohumeral joint remains one of the most formidable and technically demanding challenges in the field of orthopedic surgery. By strict academic definition, a shoulder dislocation is classified as "chronic," "neglected," or "unreduced" when the dissociation between the humeral head and the glenoid fossa has persisted unrecognized or untreated for a duration exceeding three to four weeks. Beyond this critical temporal threshold, the joint undergoes a cascade of profound, often irreversible pathoanatomic changes that render standard closed reduction techniques not only ineffective but potentially catastrophic. The glenoid fossa, devoid of its normal articulating counterpart, becomes rapidly obliterated by the proliferation of dense, organized fibrous scar tissue. Simultaneously, the joint capsule undergoes severe contracture and bowstringing, while the surrounding rotator cuff musculature—deprived of its normal resting length and tension—progressively shortens, fibroses, and retracts.

Furthermore, the unrelenting mechanical pressure exerted by the hardened cortical rim of the glenoid against the softer cancellous bone of the dislocated humeral head inevitably leads to progressive, expanding impression fractures. In the setting of chronic anterior dislocations, the posterolateral aspect of the humeral head impacts the anterior glenoid rim, creating a massive Hill-Sachs lesion. Conversely, in the setting of chronic posterior dislocations, the anteromedial aspect of the humeral head impacts the posterior glenoid rim, resulting in a reverse Hill-Sachs (or McLaughlin) lesion. As these osteochondral defects enlarge over time, they mechanically lock the humeral head outside of the glenoid vault, further complicating any efforts at relocation and significantly increasing the risk of severe joint arthrosis and humeral head osteonecrosis.

Epidemiologically, chronic unreduced dislocations present a unique bimodal distribution and are notoriously associated with missed initial diagnoses. Posterior dislocations, in particular, are missed on initial presentation in up to 60% of cases. This diagnostic failure typically occurs when evaluating physicians rely solely on standard anteroposterior (AP) radiographs, which may reveal only subtle, easily overlooked abnormalities such as the "lightbulb sign" (due to fixed internal rotation of the humerus) or the loss of the normal elliptical overlap between the humeral head and the glenoid (the "half-moon" sign). These injuries are classically associated with violent muscle contractions, such as those experienced during epileptic seizures, electrocution injuries, or extreme trauma. In contrast, chronic anterior dislocations are more frequently encountered in the elderly or in patients with profound cognitive impairment, dementia, or multiple severe medical comorbidities, where the initial traumatic event (often a low-energy fall) may have been unwitnessed, minimized, or entirely forgotten by the patient.
The clinical approach to these complex injuries spans a wide and varied spectrum, ranging from benign neglect in low-demand patients to complex open reconstructions and advanced arthroplasty techniques. The decision-making process must be meticulously individualized, taking into account a multitude of critical variables: the patient’s physiological age, functional demands, hand dominance, medical comorbidities, the exact duration of the dislocation, the precise percentage of articular surface involvement in the humeral head defect, and the structural integrity of the remaining glenoid bone stock. An axillary lateral radiograph is absolutely mandatory in all suspected cases to definitively confirm the direction of displacement and to begin quantifying the extent of the impression defect where the glenoid rim is incarcerated.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the altered surgical anatomy and biomechanics of the chronically dislocated shoulder is the absolute prerequisite for safe and effective surgical intervention. In the normal glenohumeral joint, stability is maintained by a complex interplay of static stabilizers (the labrum, glenohumeral ligaments, and joint capsule) and dynamic stabilizers (the rotator cuff musculature and the long head of the biceps tendon). However, in the setting of a chronic unreduced dislocation, this delicate anatomical equilibrium is entirely destroyed. The empty glenoid cavity rapidly fills with a dense, adherent fibrotic pannus that must be meticulously excised during open surgery to allow the humeral head to seat concentrically. The joint capsule, rather than providing a supportive hammock, becomes a rigid, contracted tether. In anterior dislocations, the anterior capsule and subscapularis are stretched and attenuated, while the posterior capsule becomes severely contracted. In posterior dislocations, the reverse is true: the posterior capsule is redundant, and the anterior structures, particularly the subscapularis and the coracohumeral ligament, become rigidly shortened.
The biomechanical implications of these neglected dislocations dictate the patient's presenting functional deficit and heavily influence the decision between operative intervention and benign neglect. Patients with untreated posterior dislocations generally exhibit significantly better functional tolerance than those with anterior dislocations. In a chronic posterior dislocation, the arm rests at the patient's side in a position of fixed internal rotation. Because the elbow can still flex and extend in this dependent position, the patient retains the biomechanical ability to perform several essential activities of daily living. They can often reach their face to feed themselves, reach the top of their head for basic grooming, and reach the anterior and posterior aspects of their torso for hygiene. While overhead elevation and external rotation are entirely lost, the arm remains functionally useful for activities occurring in the sagittal plane and internal rotation.
Conversely, the biomechanical derangement associated with an untreated anterior dislocation renders the upper extremity highly dysfunctional and often severely painful. In a chronic anterior dislocation, the humeral head is displaced anteriorly and inferiorly, resting beneath the coracoid process. This mechanically locks the arm away from the body in a position of fixed external rotation and slight abduction. The patient is unable to bring the elbow to the side of the thorax. This fixed posture makes it exceedingly difficult, if not impossible, for the patient to reach their face, feed themselves, or perform basic hygiene on the contralateral side of their body or their back. The extremity becomes an obstruction rather than a functional appendage, strongly driving the indication for surgical intervention even in relatively low-demand individuals.
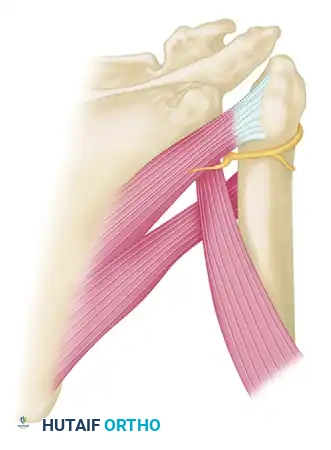
Perhaps the most critical anatomical consideration in the chronically dislocated shoulder is the severe distortion of the regional neurovascular structures, particularly the axillary nerve and the axillary artery. In chronic anterior dislocations, the subscapularis muscle is displaced anteriorly, inferiorly, and medially. This abnormal vector creates a severe traction injury to the axillary nerve. The nerve becomes physically entrapped and tethered—held superiorly by the cords of the brachial plexus and held inferiorly where it wraps tightly behind the surgical neck of the humerus through the quadrangular space. As the humeral head displaces further anteriorly over time, the axillary nerve is stretched like a bowstring across the inferior capsule.
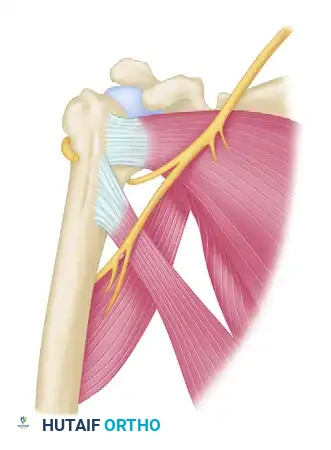
During any surgical approach, particularly the standard deltopectoral approach, the surgeon must be acutely aware that the axillary nerve is no longer in its normal anatomical safe zone. Aggressive retraction of the conjoined tendon or blind release of the inferior capsule and subscapularis can easily result in catastrophic, permanent denervation of the deltoid muscle. Similarly, in elderly patients with significant atherosclerosis, the axillary artery becomes tethered by scar tissue and the overlying pectoralis minor muscle. Any forceful manipulation or leverage applied during attempted reduction maneuvers carries a devastating risk of axillary artery rupture, necessitating immediate vascular surgery intervention.
Exhaustive Indications and Contraindications
The therapeutic algorithm for chronic unreduced shoulder dislocations is highly nuanced, requiring the surgeon to balance the severe pathoanatomic derangements against the patient's physiological capacity to withstand complex surgery and rigorous postoperative rehabilitation. It is a fundamental clinical axiom that not all patients with old, unreduced dislocations require surgical intervention. The concept of "benign neglect" is a highly valid, widely accepted management strategy for a carefully selected subset of patients. If a patient is elderly, highly inactive, institutionalized, or presents with severe medical comorbidities (e.g., advanced cardiopulmonary disease, severe dementia) that render them an unacceptable anesthetic risk, non-operative management is often the most prudent course. This is particularly true for chronic posterior dislocations, where the arm's resting position of internal rotation allows for a surprising degree of functional independence in basic activities of daily living.
When surgical intervention is indicated, the choice of procedure—ranging from closed reduction to open joint preservation techniques, to arthroplasty—is dictated primarily by the duration of the dislocation, the size of the humeral head impression defect, the quality of the articular cartilage, and the patient's age. Closed reduction is generally contraindicated for any shoulder that has been dislocated for more than three to four weeks. Attempting closed manipulative reduction beyond this timeframe is fraught with peril due to the insurmountable barriers of soft tissue contracture, glenoid fibrosis, and rotator cuff retraction. Furthermore, forceful leverage techniques in the presence of disuse osteopenia frequently result in iatrogenic fractures of the surgical neck of the humerus or catastrophic rupture of the tethered axillary artery.
Open reduction and joint-preserving soft tissue reconstructions (such as the McLaughlin procedure, Neer modification, or structural allografting) are indicated for younger, active patients with viable articular cartilage and humeral head defects involving less than 40% of the articular surface. The widely accepted Rockwood criteria provide a highly regarded algorithm for surgical decision-making based on defect size: defects less than 20% can often be managed with soft tissue transfers alone; defects between 20% and 40% require bone grafting or lesser tuberosity transfer (Neer modification); and defects exceeding 40% generally necessitate prosthetic replacement. Arthroplasty (hemiarthroplasty, anatomic total shoulder, or reverse total shoulder) is strictly indicated for older patients, patients with massive defects (>40%), severe pre-existing glenohumeral osteoarthritis, or avascular necrosis of the humeral head.
| Treatment Modality | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Benign Neglect | Elderly, low-demand patients; severe medical comorbidities; acceptable functional ROM (usually posterior dislocations); high anesthetic risk. | Young, active patients; severe intractable pain; severe neurovascular compromise; functional inability to perform ADLs. | Dominant extremity involvement; progressive neurologic deficit. |
| Closed Reduction | Dislocation duration < 3-4 weeks; absence of significant impression defect (<20%); patient medically stable for general anesthesia with full paralysis. | Dislocation duration > 4 weeks; massive impression defect (>20%); severe osteoporosis (high fracture risk); vascular calcifications. | Advanced age; history of prior failed closed reduction attempts. |
| Open Reduction & Joint Preservation | Young, active patients; dislocation > 4 weeks; humeral head defect < 40%; viable articular cartilage; failed closed reduction. | Humeral head defect > 40-50%; advanced glenohumeral osteoarthritis; established avascular necrosis of the humeral head. | Poor patient compliance with complex postoperative rehabilitation protocols. |
| Shoulder Arthroplasty (Hemi/TSA/RTSA) | Humeral head defect > 40%; severe osteoarthritis; avascular necrosis; older, lower-demand patients; chronic irreconstructible rotator cuff tears (requires RTSA). | Active joint infection; neuropathic (Charcot) joint; profound deltoid paralysis (axillary nerve injury). | Young, high-demand manual laborers (due to risk of early prosthetic loosening/failure). |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the cornerstone of successful surgical management for chronic unreduced shoulder dislocations. The imaging protocol must be exhaustive. A standard trauma series consisting of a true anteroposterior (Grashey) view, a scapular Y view, and an axillary lateral view is absolutely non-negotiable. The axillary lateral view is the most critical plain radiograph, as it definitively establishes the spatial relationship between the humeral head and the glenoid, confirms the direction of the dislocation, and allows for initial estimation of the impression defect. However, plain radiography is insufficient for definitive surgical planning. A high-resolution Computed Tomography (CT) scan without contrast, featuring 3D surface-rendered reconstructions, is mandatory for every patient scheduled for operative intervention.
The CT scan serves multiple critical functions. First, it allows the surgeon to precisely quantify the volumetric percentage of the humeral head that is involved in the Hill-Sachs or reverse Hill-Sachs defect. This calculation directly dictates the choice between joint preservation (McLaughlin/Neer transfer, allograft) and arthroplasty, as outlined by the Rockwood criteria. Second, the CT scan allows for the assessment of glenoid bone stock and version. In chronic posterior dislocations, the posterior glenoid rim is frequently eroded, leading to severe retroversion that must be addressed during surgery, either through asymmetric reaming, bone grafting, or the use of augmented glenoid baseplates if arthroplasty is chosen. Third, the CT scan helps identify any occult fractures of the surgical neck or tuberosities that could complicate intraoperative manipulation.
Pre-operative digital templating is an essential step, even if the primary surgical plan is joint preservation. The surgeon must always be prepared to convert to a hemiarthroplasty or a reverse total shoulder arthroplasty (RTSA) if the articular cartilage is found to be non-viable or if the humeral head collapses during attempted reduction. The surgeon must template for humeral stem size, head size, and glenoid component positioning. Given the high likelihood of severe soft tissue contractures, standard anatomic total shoulder arthroplasty is often less reliable than RTSA in the chronic setting, as RTSA relies on deltoid tension rather than an intact and balanced rotator cuff for stability.
Patient positioning in the operating room is typically performed in the modified beach-chair position. This position is strongly preferred over the lateral decubitus position for several reasons. First, it allows for a standard, extensile deltopectoral approach, which can be easily extended distally if humeral shaft exposure is required, or superiorly if the acromion needs to be addressed. Second, the beach-chair position provides excellent access to the anterior and posterior aspects of the shoulder, facilitating complex capsular releases and tendon transfers. Third, it allows the arm to be freely manipulated through a full range of motion to assess stability after reduction. The entire upper extremity must be meticulously prepped and draped free to allow for unencumbered manipulation. A sterile arm positioner (such as a Spider or TRIMANO arm) is highly advantageous for maintaining the extremity in precise degrees of rotation and elevation during complex reconstructive steps.
Step-by-Step Surgical Approach and Fixation Technique
When open reduction is mandated, the surgical approach must be meticulous, systematic, and highly respectful of the altered neurovascular anatomy. The standard deltopectoral approach is the workhorse incision for nearly all chronic anterior dislocations and the vast majority of chronic posterior dislocations with significant (>15-20%) anterior impression defects. The incision is made from the coracoid process extending distally toward the deltoid tuberosity. The cephalic vein is identified and typically retracted laterally with the deltoid to preserve its venous drainage, while the pectoralis major is retracted medially. The clavipectoral fascia is incised, exposing the conjoined tendon and the underlying, severely distorted subscapularis.
The first and most critical intraoperative step before any capsular release is the formal identification and protection of the axillary nerve. In chronic dislocations, the nerve is frequently encased in dense scar tissue at the inferior border of the subscapularis. The surgeon must carefully dissect the "tug lesion" of scar tissue, palpating the nerve as it crosses the anterior surface of the subscapularis before diving into the quadrangular space. Once the nerve is identified and protected with a vessel loop, the subscapularis can be addressed. In chronic posterior dislocations, the subscapularis is tightly contracted. It is typically detached via a lesser tuberosity osteotomy or a formal tenotomy, tagging the tendon with heavy non-absorbable sutures for later use in the Neer or McLaughlin reconstruction.
Following subscapularis reflection, a complete 360-degree capsular release is almost always required. The anterior, inferior, and posterior capsule must be meticulously freed from the glenoid rim. The dense, organized fibrous tissue filling the glenoid fossa is then sharply excised using a combination of curettes, rongeurs, and electrocautery until the pristine articular cartilage of the glenoid is exposed. Only after this comprehensive soft tissue release and joint clearing can reduction be attempted. Gentle traction, combined with a bone hook placed around the anatomical neck, is used to lever the humeral head back into the glenoid vault. Extreme care must be taken to avoid spiral fractures of the osteoporotic humerus during this maneuver.
Once reduced, the management of the humeral head defect is paramount to prevent immediate recurrent instability. For anteromedial impression defects seen in chronic posterior dislocations, the McLaughlin procedure and its Neer modification are the gold standard techniques.
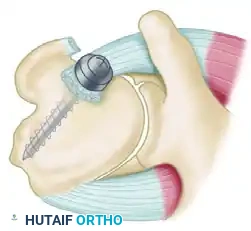
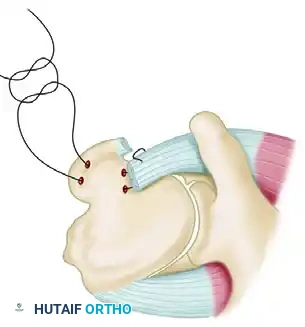
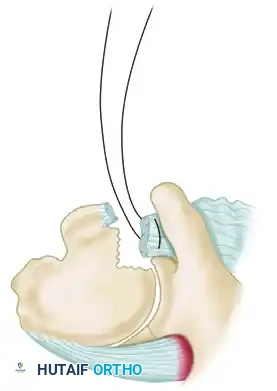
In the classic McLaughlin technique, the detached subscapularis tendon is transferred directly into the anteromedial defect. Two drill holes are placed transversely through the base of the defect, and heavy mattress sutures are passed through the tendon and the drill holes, tying the tendon securely into the void. This converts the defect into an extra-articular structure, preventing it from engaging the posterior glenoid rim during internal rotation. Neer advanced this concept significantly by utilizing a lesser tuberosity osteotomy. The subscapularis tendon, along with its attached bone block from the lesser tuberosity, is mobilized and rigidly fixed into the anterior defect using one or two cancellous lag screws. This provides superior bone-to-bone healing, which is mechanically far more robust than the tendon-to-bone healing of the original McLaughlin procedure.
For chronic posterior dislocations with moderate head defects, Elshewy et al. demonstrated excellent outcomes utilizing an open reduction combined with a posterior capsular shift.




This technique involves a T-shaped incision of the redundant posterior capsule. After the joint is reduced and cleared of scar tissue, the inferior capsular flap is shifted superiorly and laterally to eliminate redundancy. The superior flap is then brought down to overlap the inferior flap, creating a robust, double-layered reinforcement of the posterior repair that effectively prevents posterior subluxation. In highly selected cases with healthy cartilage and defects under 40%, a proximal humeral rotational osteotomy can be performed. By rotating the humeral shaft externally, the impression defect is moved permanently out of the functional arc of motion.
In cases where severe capsular deficiency or massive bone loss renders the reduction acutely unstable despite soft tissue reconstruction, temporary internal fixation across the glenohumeral joint may be a necessary, albeit risky, adjunct.
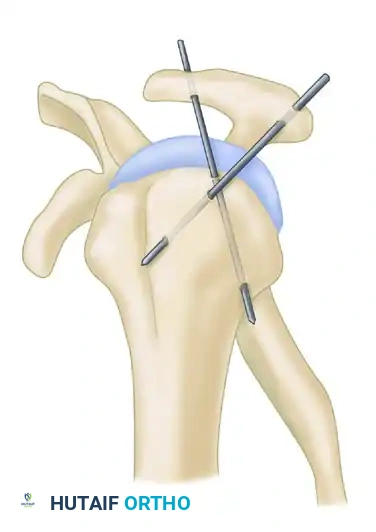
Techniques include the use of a large Swiss screw driven through the acromion directly into the humeral head (as described by Neviaser), or the Wilson and McKeever method utilizing two heavy, crossed Kirschner wires driven through the acromion into the humeral head. While these techniques can salvage an unstable reduction, they carry significant risks of hardware migration, articular cartilage damage, and pin-tract infections, and should be used only as a last resort.
Complications, Incidence Rates, and Salvage Management
The surgical management of chronic unreduced shoulder dislocations is associated with an exceptionally high complication rate, reflecting the severe underlying pathoanatomy and the technical difficulty of the required reconstructions. Surgeons undertaking these cases must be intimately familiar with potential pitfalls and possess the advanced skill sets required for immediate salvage management. The most devastating intraoperative complication is iatrogenic injury to the major neurovascular structures. Axillary nerve palsy occurs in up to 10-15% of open reductions for chronic anterior dislocations, resulting from excessive traction during exposure or inadvertent transection during the release of the severely scarred inferior capsule. If the nerve is completely transected, immediate microsurgical repair or nerve grafting is required. Axillary artery rupture is a catastrophic complication primarily associated with forceful closed reduction attempts in elderly patients with atherosclerotic vessels; it necessitates emergent vascular surgery consultation for bypass or grafting to prevent limb loss.
Postoperative complications are equally challenging. Recurrent instability is a frequent issue, particularly if the humeral head impression defect was underappreciated or inadequately addressed during the primary surgery. Failure of the Neer or McLaughlin transfer, either due to screw pullout or tendon rupture, allows the defect to re-engage the glenoid rim, leading to immediate re-dislocation. In such cases, salvage typically requires conversion to a reverse total shoulder arthroplasty (RTSA), as the native joint mechanics are often irreparably compromised. Avascular necrosis (AVN) of the humeral head is another significant long-term complication, occurring in 15-25% of cases. The risk of AVN is directly proportional to the duration of the dislocation and the extensiveness of the soft tissue stripping required to achieve reduction. If AVN progresses to symptomatic structural collapse, prosthetic replacement is the only viable salvage option.
Postoperative stiffness is ubiquitous and should be considered an expected outcome rather than a true complication. The extensive capsular releases, combined with the required period of strict postoperative immobilization to allow soft tissue healing, inevitably lead to a profound loss of glenohumeral motion. While aggressive, phased physical therapy can recover functional arcs of motion, patients rarely, if ever, regain full symmetric range of motion. Heterotopic ossification may also occur in the periarticular soft tissues, further limiting mobility, though it rarely requires surgical excision unless it causes a rigid mechanical block.
| Complication | Estimated Incidence | Primary Etiology | Salvage Management / Treatment |
|---|---|---|---|
| Axillary Nerve Palsy | 8 - 15% | Traction injury during exposure; inadvertent transection during inferior capsular release. | Observation and EMG at 3 months for neuropraxia; nerve grafting or tendon transfers for permanent deficits. |
| Recurrent Dislocation | 10 - 20% | Inadequate addressing of the humeral head defect; failure of hardware/tendon transfer; patient non-compliance. | Revision open reduction with structural allografting; conversion to Reverse Total Shoulder Arthroplasty (RTSA). |
| Avascular Necrosis (AVN) | 15 - 25% | Disruption of the ascending branch of the anterior humeral circumflex artery; extensive soft tissue stripping. | Observation for asymptomatic cases; conversion to Hemiarthroplasty or Total Shoulder Arthroplasty for symptomatic collapse. |
| Axillary Artery Rupture | < 1 - 2% | Forceful closed reduction in elderly/atherosclerotic patients; extreme traction during open exposure. | Emergent vascular surgery consultation; vascular bypass or interposition grafting; fasciotomies if ischemia is prolonged. |
| Severe Joint Stiffness | > 80% | Extensive surgical scarring; mandatory postoperative immobilization; capsular contracture. | Aggressive physical therapy; arthroscopic capsular release (rarely indicated, high risk of re-instating instability). |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following the surgical management of a chronic shoulder dislocation is a highly delicate, protracted process that requires a meticulous balance between protecting the fragile surgical reconstruction and preventing devastating, permanent joint stiffness. The protocol must be strictly customized based on the direction of the original instability, the specific type of soft tissue or bony reconstruction performed, and the intraoperative assessment of joint stability. The foundational principles of postoperative immobilization for these complex injuries were definitively established by Rowe and Zarins, who emphasized that the spatial plane of immobilization is critical for preventing immediate recurrence.