Open Reduction of Anterior Shoulder Dislocations: Surgical Techniques and Protocols
Key Takeaway
Open reduction of an anterior shoulder dislocation is indicated for chronic, irreducible, or complex fracture-dislocations. Utilizing the Rowe and Zarins technique via a deltopectoral approach allows for direct visualization, subscapularis release, and capsular mobilization. Meticulous surgical technique is paramount to safely clear the fibrotic glenoid fossa, achieve concentric reduction without iatrogenic fracture, and protect the axillary nerve during subscapularis repair.
Comprehensive Introduction and Patho-Epidemiology
While the vast majority of acute anterior shoulder dislocations can be successfully managed with closed reduction techniques in the emergency department, a distinct and highly challenging subset of patients requires surgical intervention. Open reduction of an anterior shoulder dislocation is a formidable orthopedic undertaking, typically reserved for chronic (unreduced) dislocations, irreducible acute dislocations secondary to soft tissue interposition (e.g., the long head of the biceps tendon, capsule, or subscapularis), or complex fracture-dislocations where closed manipulation poses an unacceptable risk of iatrogenic neurovascular or osseous injury. The transition from a simple acute dislocation to a chronic, irreducible state represents a profound shift in the local biomechanical and cellular environment of the glenohumeral joint.
The pathoanatomy of a chronic anterior dislocation is characterized by severe soft tissue contracture and rapid osseous remodeling. The anterior capsule, the rotator interval, and the coracohumeral ligament become profoundly contracted, effectively tethering the humeral head in its dislocated, anteroinferior position beneath the coracoid process. Concurrently, the empty glenoid fossa rapidly fills with dense, tenacious fibrocartilaginous and scar tissue, obliterating the articular concavity and removing the congruent surface necessary for a stable reduction. This fibrotic obliteration is a rapid cellular response to the hemarthrosis and subsequent inflammatory cascade initiated at the time of the initial dislocation.
Furthermore, the dislocated humeral head undergoes rapid disuse osteopenia. Stripped of its normal mechanical loading and bathed in an inflammatory milieu, the trabecular architecture of the humeral head rapidly deteriorates. This renders the proximal humerus highly susceptible to iatrogenic crush fractures, indentation injuries, or shear fractures during forceful reduction attempts. The chronicity of the dislocation also dictates the severity of secondary osseous defects, such as the progressive enlargement of a Hill-Sachs lesion as the humeral head continuously abrades against the anterior glenoid rim, or the attritional loss of the anterior glenoid bone stock itself. Understanding this hostile pathoanatomic environment is paramount for the orthopedic surgeon, as it dictates the necessity for extensive surgical releases and meticulous, low-force reduction maneuvers.
Detailed Surgical Anatomy and Biomechanics
Osseous and Articular Architecture
The glenohumeral joint is inherently unstable, often described as a "golf ball on a tee," relying heavily on a complex interplay of static and dynamic soft tissue stabilizers. The osseous anatomy features a large humeral head articulating with a shallow, pear-shaped glenoid fossa. The glenoid is typically retroverted by approximately 2 to 7 degrees and tilted superiorly by 5 degrees. In chronic anterior dislocations, the anterior rim of the glenoid is frequently eroded, altering this version and significantly compromising the bony buttress against anterior translation. The humeral head, normally retroverted approximately 30 degrees relative to the epicondylar axis, may sustain a substantial posterolateral impaction fracture (Hill-Sachs lesion) that can engage the anterior glenoid rim, further locking the joint in a dislocated position.
Static Soft Tissue Stabilizers
The static stabilizers of the glenohumeral joint include the glenoid labrum, the articular capsule, and the glenohumeral ligaments. The labrum deepens the glenoid concavity by approximately 50%, providing a critical "chock-block" effect. The capsuloligamentous complex consists of the superior, middle, and inferior glenohumeral ligaments (SGHL, MGHL, IGHL). The IGHL is the most critical static stabilizer against anterior translation when the arm is abducted and externally rotated. It functions as a hammock, with a distinct anterior band, posterior band, and axillary pouch. In chronic anterior dislocations, the anterior band of the IGHL is often avulsed from the glenoid (Bankart lesion) and subsequently scars down in a medially displaced position along the scapular neck (ALPSA lesion), requiring meticulous surgical mobilization to restore its anatomic footprint.
Dynamic Stabilizers and Neurovascular Proximity
The dynamic stabilizers comprise the rotator cuff muscles (subscapularis, supraspinatus, infraspinatus, and teres minor), the long head of the biceps tendon, and the periscapular musculature. The subscapularis is of paramount importance in the open anterior approach; it must be mobilized and subsequently repaired with absolute integrity to prevent postoperative anterior subluxation. The neurovascular anatomy is intricately related to these structures and is at extreme risk during open reduction. The axillary nerve exits the axilla through the quadrangular space, passing immediately inferior to the muscular border of the subscapularis and the inferior joint capsule. In a chronic anteroinferior dislocation, the humeral head frequently stretches the axillary nerve and the posterior cord of the brachial plexus. The nerve becomes encased in perineural fibrosis, significantly increasing the risk of iatrogenic transection or traction neurapraxia during inferior capsular releases.
Exhaustive Indications and Contraindications
The decision to proceed with an open reduction of an anterior shoulder dislocation requires a nuanced understanding of the patient's physiological status, the chronicity of the dislocation, and the presence of concomitant osseous or soft tissue injuries. A meticulous risk-benefit analysis must be conducted, weighing the morbidity of the surgical exposure against the functional deficits of a chronically dislocated shoulder.
Indications for Open Reduction
Surgical intervention is absolutely indicated in cases of acute irreducible dislocations. Irreducibility is most commonly caused by soft tissue interposition. The long head of the biceps tendon can rupture and interpose itself between the humeral head and the glenoid, or the joint capsule can buttonhole around the humeral head, preventing closed reduction. Additionally, complex fracture-dislocations, such as those involving a displaced surgical neck fracture combined with an anterior dislocation, prohibit closed manipulation due to the inability to transmit torque to the articular segment, risking further displacement or neurovascular compromise. Chronic, unreduced dislocations (typically defined as those persisting for greater than 3 to 4 weeks) almost universally require open reduction due to the severe soft tissue contractures and fibrotic obliteration of the glenoid fossa described previously.
Contraindications to Surgical Intervention
Contraindications to open reduction can be absolute or relative. Absolute contraindications include active surgical site infection, severe medical comorbidities precluding general anesthesia, or a patient who is non-ambulatory and entirely asymptomatic with a chronic dislocation (a state of "tolerated pseudoparalysis"). Relative contraindications include severe, long-standing chronic dislocations in elderly, low-demand patients where the risk of iatrogenic fracture, axillary nerve palsy, or catastrophic postoperative stiffness outweighs the potential functional gains. In such cases, a "skillful neglect" approach or primary reverse total shoulder arthroplasty (if the rotator cuff is deficient and bone stock allows) may be more appropriate alternative strategies.
Tabular Summary of Indications and Contraindications
| Category | Specific Condition | Rationale and Clinical Details |
|---|---|---|
| Absolute Indication | Acute Irreducible Dislocation | Soft tissue interposition (biceps, capsule, subscapularis) prevents closed reduction. Attempting forceful closed reduction will cause iatrogenic injury. |
| Absolute Indication | Complex Fracture-Dislocation | Displaced surgical neck fractures with dislocation cannot be closed reduced; manipulation will displace the fracture further and risk the axillary artery. |
| Absolute Indication | Chronic Unreduced Dislocation (>4 weeks) | Fibrotic filling of the glenoid and capsular contracture render closed reduction physically impossible and highly dangerous to the osteopenic humeral head. |
| Relative Indication | Concomitant Massive Cuff Tear | In younger/active patients, open reduction allows for simultaneous repair of massive rotator cuff tears associated with the dislocation. |
| Absolute Contraindication | Active Glenohumeral Infection | Purulent arthritis or overlying cellulitis precludes elective open reduction and internal fixation/repair. |
| Relative Contraindication | Asymptomatic Elderly Patient | A low-demand patient with a chronic dislocation who has adapted to the functional deficit and is pain-free may face higher risks from surgery than from non-operative management. |
| Relative Contraindication | Severe Neurologic Deficit | Pre-existing complete brachial plexopathy or devastating axillary nerve palsy may render the limb functionally useless even if concentric reduction is achieved. |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging and Osseous Templating
Thorough preoperative planning is mandatory and relies heavily on high-quality, multi-modal imaging. Standard trauma series radiographs (true anteroposterior, scapular Y, and axillary lateral views) are essential to confirm the direction of the dislocation and identify gross osseous lesions. However, advanced imaging, particularly Computed Tomography (CT) with 3D reconstruction with digital subtraction of the humeral head, is the gold standard for chronic dislocations. This allows the surgeon to meticulously quantify anterior glenoid bone loss and assess the structural integrity, depth, and orientation of the humeral head (Hill-Sachs defect). Templating the "glenoid track" is critical; if the Hill-Sachs lesion is off-track (engaging), the surgeon must be prepared to perform an adjunctive Remplissage procedure or an anterior bony augmentation (Latarjet) concomitantly with the open reduction.
Neurologic Assessment and Soft Tissue Evaluation
Magnetic Resonance Imaging (MRI) is frequently utilized to evaluate the status of the rotator cuff, which is torn in up to 80% of patients over the age of 60 who sustain an anterior shoulder dislocation. Identifying a massive, retracted rotator cuff tear preoperatively alters the surgical plan, potentially necessitating a transition to a primary reverse total shoulder arthroplasty in the older demographic. Furthermore, a meticulous clinical neurologic examination is paramount. The axillary nerve and the musculocutaneous nerve are at significant risk. The humeral head often rests directly against the brachial plexus cords. Preoperative electromyography (EMG) and nerve conduction studies (NCS) must be documented in chronic cases to establish a baseline before surgical intervention, differentiating pre-existing traction neurapraxia from iatrogenic surgical injury.
Anesthesia, Positioning, and Draping
General endotracheal anesthesia is preferred, ensuring complete neuromuscular blockade to eliminate dynamic muscle resistance during the reduction maneuver. This is almost universally supplemented with an interscalene regional nerve block, which provides optimal postoperative pain control and decreases the general anesthetic requirement. The patient is placed in the beach-chair (modified Fowler) position, with the head and neck secured in a neutral posture using a specialized headrest to prevent cervical spine hyperextension or lateral flexion, which could stretch the contralateral brachial plexus. The affected upper extremity is prepped and draped free to allow for completely unrestricted manipulation of the arm. A sterile pneumatic arm positioner (e.g., Spider arm or Trimano) is highly recommended, as it allows the surgeon to maintain the limb in precise degrees of traction, abduction, and rotation during the delicate capsular releases and subsequent reduction.
Step-by-Step Surgical Approach and Fixation Technique
The technique described by Rowe and Zarins remains a foundational procedure for the open reduction of complex or chronic anterior shoulder dislocations. It utilizes a standard anterior deltopectoral approach, providing extensile access to the anterior glenohumeral joint while preserving the deltoid origin, which is critical for postoperative function.
The Deltopectoral Approach and Superficial Dissection
The procedure begins with a longitudinal incision extending from the lateral third of the clavicle, coursing inferiorly and slightly laterally along the deltopectoral groove for approximately 10 to 12.5 cm toward the deltoid tuberosity. The superficial fascia is incised, and the deltopectoral interval is identified by locating the cephalic vein. The management of the cephalic vein is dictated by its venous tributaries; it is typically retracted laterally with the deltoid muscle to preserve its primary deltoid branches, minimizing postoperative venous congestion of the muscle flap. However, medial retraction with the pectoralis major is an acceptable alternative if the venous anatomy dictates. The deep dissection proceeds by separating the deltoid and pectoralis major muscles to expose the underlying clavipectoral fascia.
Deep Dissection and Subscapularis Management
The clavipectoral fascia is incised lateral to the conjoined tendon (comprising the short head of the biceps brachii and the coracobrachialis). The conjoined tendon is retracted medially using a blunt retractor (e.g., a Richardson or a conjoint retractor). Extreme care must be taken during medial retraction to avoid traction injury to the musculocutaneous nerve, which enters the coracobrachialis muscle belly as proximally as 2 to 5 cm distal to the coracoid tip. At this stage, the dislocated humeral head may be directly visualized or palpated in an abnormal anteroinferior position. The subscapularis muscle is typically stretched tightly over the dislocated head. Access to the joint requires mobilization of the subscapularis. While a vertical tenotomy 1 cm medial to the lesser tuberosity is common, a lesser tuberosity osteotomy (LTO) is frequently preferred in chronic cases. An LTO provides bone-to-bone healing upon closure, which is biomechanically superior and allows for more aggressive early postoperative rehabilitation compared to a soft tissue tenotomy repair.
Capsular Mobilization and Glenoid Preparation
The critical barrier to reduction in a chronic setting is the contracted soft tissue envelope and the fibrotic obliteration of the glenoid. Following subscapularis reflection, a formal anterior capsulotomy is performed. It is imperative to completely divide the contracted coracohumeral ligament and the rotator interval tissue, which act as primary tethers preventing the humeral head from translating posteriorly and inferiorly back into the glenoid. The surgeon must then inspect the glenoid cavity. In chronic cases, it will be entirely filled with dense, organized fibrous tissue. A combination of ring curettes, pituitary rongeurs, and periosteal elevators is used to meticulously free the glenoid cavity of this fibrotic material. The labrum should be preserved if possible, but the articular surface must be completely exposed. Failure to completely clear the glenoid fossa will result in an eccentric reduction, excessive pressure on the articular cartilage, and immediate postoperative instability.
The Reduction Maneuver and Extensile Exposures
Once the glenoid is prepared and the capsular releases are complete, the reduction maneuver is attempted. The surgeon must avoid using excessive mechanical force or heavy metallic levers (e.g., bone skids or Cobb elevators) against the articular surface. The osteoporotic bone of the chronically dislocated humeral head is exceptionally fragile and will collapse under focal pressure. Reduction is achieved by applying gentle, sustained longitudinal traction to the arm while simultaneously translating the humeral head laterally and posteriorly, utilizing a "shoehorn" technique with a broad, smooth instrument only if absolutely necessary.
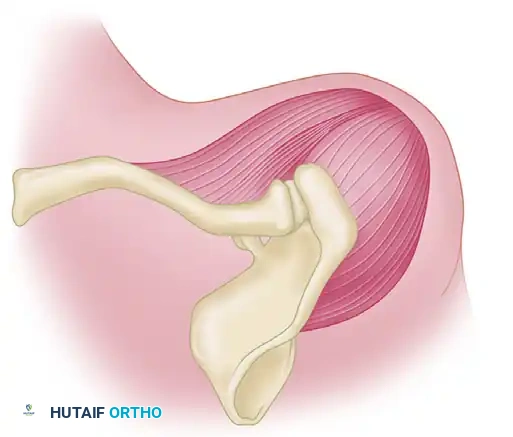
In cases of severe chronic unreduced dislocations where the standard deltopectoral approach provides insufficient access, an extensile approach may be indicated. As described by Rowe and Zarins for highly complex reconstructions, a deltoid turn-down approach can be utilized.
Rather than detaching the deltoid directly from the bone—which carries an unacceptably high risk of postoperative deltoid dehiscence—a precise osteotomy of the acromion is performed. As illustrated, the osteotomy is made to leave approximately 5 mm of acromial bone attached to the proximal origin of the deltoid muscle. The deltoid muscle, along with its attached bony sleeve, is then reflected distally. This provides unparalleled, 270-degree visualization of the glenohumeral joint, allowing for extensive posterior capsular releases and safe mobilization of the chronically displaced head. During closure, the bony sleeve is rigidly repaired back to the native acromion using heavy transosseous sutures or tension band wiring.
Complications, Incidence Rates, and Salvage Management
Surgeons undertaking the open reduction of chronic anterior dislocations must be acutely aware of the high complication profile associated with this procedure. The altered anatomy, poor bone quality, and extensive soft tissue contractures create a surgical minefield that requires meticulous technique and advanced reconstructive capabilities.
Iatrogenic Fractures and Neurologic Injury
Iatrogenic fractures of the proximal humerus are among the most devastating intraoperative complications. The disuse osteopenia renders the humeral head highly susceptible to indentation or catastrophic fracture during reduction maneuvers. Forceful leverage must be strictly avoided. If a fracture occurs, the surgeon must be prepared to seamlessly transition to internal fixation using locking plates or, in cases of severe comminution with an unsalvageable articular surface, a primary hemiarthroplasty or reverse total shoulder arthroplasty. Neurologic injury, particularly to the axillary nerve, is another severe risk. The nerve is frequently tethered by scar tissue at the inferior capsule. Meticulous identification and protection of the nerve during the inferior capsular release are mandatory. Postoperative deltoid atony should prompt immediate neurologic evaluation and consideration for early nerve exploration if the injury is deemed iatrogenic rather than a preoperative traction neurapraxia.
Osteonecrosis and Postoperative Stiffness
Extensive soft tissue stripping required to achieve reduction can severely compromise the delicate blood supply to the humeral head, which is primarily derived from the ascending branch of the anterior humeral circumflex artery. Disruption of this blood supply, combined with the initial trauma, places the patient at a high risk for late-onset osteonecrosis (avascular necrosis). Patients must be thoroughly counseled on this risk preoperatively, as progressive collapse of the humeral head will eventually necessitate prosthetic arthroplasty. Furthermore, while recurrent instability is a known risk, severe postoperative stiffness (frozen shoulder) is far more common following open reduction of chronic dislocations. The extensive surgical trauma and necessary postoperative immobilization create a perfect storm for profound capsular fibrosis.
Tabular Summary of Complications and Salvage
| Complication | Estimated Incidence | Pathoetiology and Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Iatrogenic Humeral Fracture | 5% - 15% | Severe disuse osteopenia; forceful use of bone skids or excessive rotational torque during reduction. | Immediate Open Reduction Internal Fixation (ORIF) with locking plates; Arthroplasty if severely comminuted. |
| Axillary Nerve Injury | 3% - 10% | Altered anatomy; nerve tethered in scar tissue at the inferior capsule; iatrogenic suture ligation during subscapularis repair. | Observation with serial EMG/NCS for neurapraxia; early microsurgical exploration and grafting for documented transection. |
| Osteonecrosis (AVN) | 10% - 25% | Disruption of the anterior humeral circumflex artery during extensive soft tissue releases and capsulotomies. | Conservative management initially; core decompression if early stage; Total Shoulder Arthroplasty for advanced collapse. |
| Severe Postoperative Stiffness | 30% - 50% | Extensive surgical trauma, prolonged immobilization, and robust fibrotic healing response. | Aggressive physical therapy; Arthroscopic capsular release and manipulation under anesthesia (MUA) if refractory after 6 months. |
| Recurrent Instability | 5% - 10% | Failure to address significant anterior glenoid bone loss or engaging Hill-Sachs lesions; failed subscapularis repair. | Revision stabilization with bone block augmentation (Latarjet procedure) or Remplissage. |
Phased Post-Operative Rehabilitation Protocols
The postoperative care following an open reduction of an anterior shoulder dislocation is arguably as critical as the surgical intervention itself. The rehabilitation protocol must be carefully tailored to balance the competing demands of protecting the delicate soft tissue repairs (specifically the subscapularis and anterior capsule) while aggressively preventing debilitating postoperative stiffness. The protocol varies significantly depending on whether adjunctive internal fixation was required for associated fractures or severe instability.
Phase I: Immobilization and Early Protection (Weeks 0 to 3)
If the standard soft-tissue open reduction technique is utilized without internal osseous fixation, the arm is strictly supported in a sling or shoulder immobilizer. If a lesser tuberosity osteotomy was performed, the protection of the osseous repair is paramount. The arm is typically immobilized in neutral rotation or slight internal rotation to minimize tension on the anterior structures. During this initial phase, active range of motion of the elbow, wrist, and hand is highly encouraged to prevent distal edema and stiffness, as well as to promote venous return. Cryotherapy is utilized extensively to manage postoperative inflammation. Passive external rotation is strictly prohibited during this phase to protect the subscapularis repair or osteotomy site from catastrophic failure.
Phase II: Early Motion and Proprioception (Weeks 3 to 6)
At the 3 to 4-week mark, the focus shifts to restoring glenohumeral kinematics while continuing to respect the healing anterior structures. If temporary internal fixation (such as transarticular Kirschner wires used historically for highly unstable joints) was utilized, it is removed at this stage. Gentle pendulum (Codman) exercises are initiated to introduce early, low-stress joint mobilization. Passive and active-assisted forward elevation and scapular plane abduction are gradually introduced. These exercises must be strictly continued within the ranges of comfort. Aggressive passive stretching, particularly into external rotation past neutral, remains contraindicated. Scapulothoracic mobilization and periscapular isometric exercises are initiated to prevent scapular dyskinesia, which rapidly develops following prolonged glenohumeral immobilization.
Phase III: Strengthening and Functional Return (Weeks 6 and Beyond)
Progression to full active range of motion is encouraged as tolerated by pain and radiographic evidence of tissue healing (particularly if an LTO was performed). Because the dynamic stabilizers of the shoulder, specifically the rotator cuff and deltoid, have undergone significant atrophy during both the chronic dislocation period and the postoperative immobilization, the shoulder remains highly vulnerable to subluxation during sleep. The shoulder should be supported in a splint at night for several months until robust, active abduction and dynamic stability have been regained. Isotonic and isokinetic strengthening of the rotator cuff and periscapular stabilizers begins at 6 to 8 weeks. Rehabilitation focuses heavily on the subscapularis and infraspinatus to restore the critical transverse force couple of the glenohumeral joint, ensuring concentric rotation of the humeral head within the glenoid fossa during dynamic overhead activities.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for complex anterior shoulder dislocations is deeply rooted in landmark anatomical and clinical studies. The foundational work by Rowe and Zarins in the mid-20th century established the benchmark for the open anterior approach, emphasizing the absolute necessity of identifying and mobilizing the contracted subscapularis and clearing the fibrotic glenoid fossa. Their detailed descriptions of the pathoanatomy of chronic dislocations remain highly relevant, particularly their warnings regarding the fragility of the osteopenic humeral head and the high risk of iatrogenic fractures during forceful reduction attempts.
In modern orthopedic literature, the paradigm has shifted significantly toward an advanced biomechanical understanding of osseous defects. The concept of the "glenoid track," popularized by Di Giacomo, Itoi, and Burkhart, has revolutionized preoperative planning. Current clinical guidelines dictate that open reduction must not only restore the humeral head to the glenoid but must also definitively address the bipolar bone loss that invariably accompanies chronic dislocations. If a Hill-Sachs lesion is deemed "off-track" (engaging the anterior glenoid rim during abduction and external rotation), simple open reduction and capsulorrhaphy are destined to fail. In these scenarios, contemporary literature mandates concomitant procedures, such as an open Latarjet (coracoid transfer) to restore the anterior glenoid arc, or an open Remplissage (infraspinatus tenodesis into the humeral defect) to convert an intra-articular defect into an extra-articular one, thereby preventing engagement and recurrent instability.
Furthermore, recent systematic reviews comparing open versus arthroscopic management of chronic dislocations highlight that while arthroscopic contracture release is gaining traction for subacute cases, the open deltopectoral approach remains the gold standard for truly chronic (>3 months), unreduced anterior dislocations. The open approach provides the necessary extensile exposure to safely manage the encased neurovascular structures, perform complex osseous reconstructions, and achieve a stable, concentric reduction in the face of severe anatomical distortion.
📚 Medical References
- [anterior shoulder dislocation: an arthroscopic study, Arthroscopy 10:478, 1994.](https://pubmed.ncbi.nlm.nih.gov/?term=anterior%20shoulder%20dislocation%3A%20an%20arthroscopic%20study%2C%20Arthroscopy%2010%3A478"
