Scapulothoracic Decompression & Bursectomy: An Intraoperative Masterclass
Key Takeaway
Welcome to the OR, fellows. Today, we're tackling snapping scapula syndrome. This masterclass will guide you through the intricate anatomy, meticulous preoperative planning, and both open and arthroscopic surgical decompression techniques. We'll cover precise instrument use, critical neurovascular considerations, and strategies for managing potential pitfalls, ensuring a comprehensive understanding of this challenging condition and optimizing patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Welcome to the operating theater, colleagues. Today, we are addressing a fascinating, often debilitating, and frequently misdiagnosed condition: snapping scapula syndrome. While first described by the French physician Boinet in 1867, its clinical nuances and optimal surgical management continue to challenge even the most seasoned shoulder and elbow surgeons. This pathology is not merely a simple "creak" or benign joint noise; it represents a painful disruption of scapulothoracic motion accompanied by distinct crepitus. This crepitus can range from a gentle, almost imperceptible friction rub to a loud, pathologic snap that can be heard across the examination room. The etiology is highly variable, occurring with or without a clear history of macrotrauma, and most often stems from a relentless cycle of repetitive overuse and microtrauma in overhead athletes or manual laborers.
Historically, this clinical entity has been referred to by a myriad of names in the orthopedic literature, including scapulothoracic bursitis, retroscapular creaking, superior scapular syndrome, washboard syndrome, and retroscapular pain. At its fundamental core, this syndrome boils down to a profound incongruence of the scapulothoracic articulation. This mechanical mismatch is sometimes compounded by overt bony anomalies, but more frequently, it is a soft-tissue phenomenon. The audible and tactile crepitus, as elegantly described by Milch and Burman in their seminal works, is a tactile-acoustic phenomenon. It is the direct mechanical result of an abnormality within the narrow, highly constrained scapulothoracic interval. This dynamic maltracking or static compression irritates the intervening bursal tissues, leading to a vicious, self-perpetuating cycle of inflammation, fibrovascular proliferation, and escalating pain.
It is absolutely crucial for the operating surgeon to appreciate the clinical spectrum of crepitus, which we classify into three distinct groups based on acoustic volume and pathophysiologic origin. First is Physiologic Crepitus, characterized by a "gentle friction" sound. This is often asymptomatic, representing normal fluid dynamics and fascial gliding within the periscapular tissues. Second is Grating Crepitus, which presents as louder, grinding sounds. This is characteristic of the vast majority of symptomatic snapping scapula patients and typically represents fibrotic, thickened bursal tissue catching between the scapula and the thoracic cage. Finally, we have Pathologic Snapping, a loud, distinct, and sharply defined snapping noise. This presentation is almost invariably indicative of an underlying structural or bony pathology, such as an osteochondroma or a malunited rib fracture, forcefully striking the deep surface of the scapula.
Epidemiologically, snapping scapula syndrome presents most frequently in young, active patients, typically in their second to third decades of life. Overhead athletes—particularly baseball pitchers, swimmers, and volleyball players—are at exceptionally high risk due to the extraordinary demands placed on periscapular stabilization and the repetitive extremes of scapular protraction and retraction. The insidious onset of symptoms often masks the underlying microtraumatic cascade. As the scapulothoracic bursae become chronically inflamed, intrafascicular fibrosis develops within the subscapularis and serratus anterior muscles. This leads to subtle scapular dyskinesia, further exacerbating the mechanical impingement, and ultimately resulting in profound shoulder girdle muscle atrophy and intractable pain if left untreated.
Detailed Surgical Anatomy and Biomechanics
Before we even consider making an incision or establishing an arthroscopic portal, a master-level deep dive into the regional anatomy is paramount. The scapulothoracic articulation is a highly complex dynamic interface between the concave anterior aspect of the scapula and the convex posterior thoracic chest wall. It is critical to understand that this is not a true diarthrodial synovial joint; rather, it is a muscular articulation, devoid of a true joint capsule, and cushioned entirely by several key muscle bellies and specialized bursal sacs. The harmonious gliding of this articulation is responsible for roughly one-third of total shoulder elevation, making its preservation essential for normal upper extremity biomechanics.
The primary muscular cushions that facilitate this articulation are the subscapularis on the deep, ventral surface of the scapula and the serratus anterior, which originates from the lateral aspects of the first through eighth ribs and inserts onto the entire length of the medial border of the scapula. These muscles act as dynamic shock absorbers, allowing for smooth, frictionless gliding of the scapula across the rib cage during complex multi-planar movements. Within this muscular interval, we find several distinct bursae, which are the epicenter of the pathology in non-osseous snapping scapula syndrome.
The bursal anatomy is classically divided into major and minor bursae. The Major Bursae consist of the infraserratus bursa (located between the serratus anterior muscle and the posterolateral chest wall) and the supraserratus bursa (situated between the serratus anterior and the subscapularis muscle bellies). The Minor Bursae are more variable but highly clinically relevant. They include two bursae located at the superomedial angle of the scapula, one at the inferior angle of the scapula, and a trapezoid bursa located at the medial base of the scapular spine, deep to the trapezius muscle. Chronic, repetitive motion irritates these soft tissues, leading to a cascade of inflammation, profound fibrosis, and dense scarring. This thickened tissue physically occupies space in the scapulothoracic interval, further exacerbating mechanical impingement, altering scapular kinematics, and generating the characteristic grating crepitus.
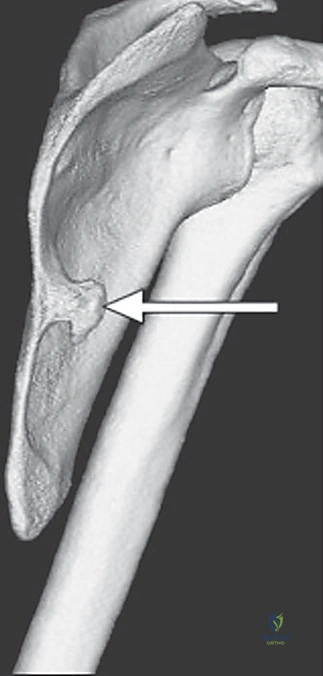
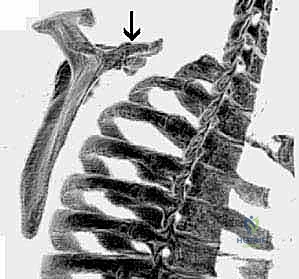
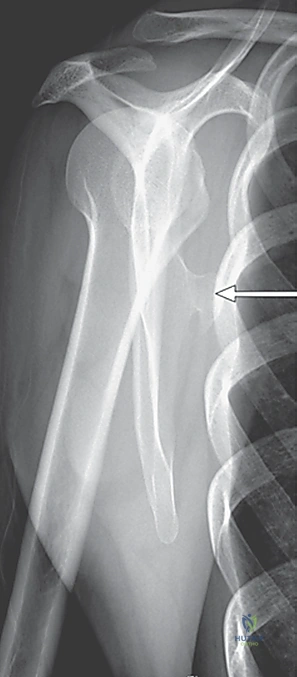
While soft-tissue bursitis is the most common culprit, osteology and bony anomalies represent definitive, structural sources of pathologic snapping that must be meticulously ruled out. The most frequent osseous cause is a scapular osteochondroma or exostosis, which has a distinct predilection for the superomedial angle or the ventral surface of the scapular body. Other skeletal etiologies include an exaggerated anterior angulation of the superomedial scapula, malunited scapula or rib fractures, the presence of a Luschka tubercle (an anomalous bony prominence at the superomedial border), and complex skeletal abnormalities of the cervicothoracic spine such as an omovertebral bone seen in Sprengel's deformity.
Surgical intervention in this region is fraught with neurovascular risks, and meticulous, plane-specific dissection is non-negotiable. The Dorsal Scapular Nerve (DSN) and its accompanying artery are at extreme risk during medial border exposures. The DSN innervates the rhomboids and levator scapulae, typically coursing parallel to the medial border of the scapula, approximately 2 cm medial to the osseous edge. Iatrogenic injury here leads to devastating lateral scapular winging. The Long Thoracic Nerve (LTN), which innervates the serratus anterior, runs superficially along the muscle belly anterior to the midaxillary line; over-penetration during arthroscopic bursectomy can cause classic medial winging. Furthermore, the Spinal Accessory Nerve (SAN) and transverse cervical artery, supplying the trapezius, are highly vulnerable during superior portal placement. Finally, the intercostal neurovascular bundles running along the inferior borders of the ribs must be respected during deep arthroscopic shaving or aggressive open bony resections to prevent intractable intercostal neuralgia or massive hemothorax.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention for snapping scapula syndrome must be highly calculated and strictly evidence-based. Surgery is rarely, if ever, the first line of treatment. The absolute primary indication for scapulothoracic decompression—whether open or arthroscopic—is the persistence of debilitating, functionally limiting pain and mechanical crepitus that has definitively failed a rigorous, comprehensive 3 to 6-month trial of conservative management. This conservative protocol must include activity modification, targeted non-steroidal anti-inflammatory drugs (NSAIDs), and, most importantly, a highly specific physical therapy regimen focused on periscapular muscle strengthening, core stabilization, and postural correction.
A critical component of the surgical indication is the patient's response to a diagnostic injection. We consider a fluoroscopically or ultrasound-guided injection of local anesthetic and corticosteroid into the symptomatic scapulothoracic bursa (most frequently the superomedial bursa) to be pathognomonic. If the patient experiences near-complete, albeit temporary, relief of their pain and a cessation or significant reduction of their mechanical symptoms, they are considered an excellent surgical candidate. Conversely, a failure to achieve relief from a properly placed injection should give the surgeon serious pause and prompt a re-evaluation of the primary diagnosis, looking for cervical radiculopathy, glenohumeral pathology, or primary nerve palsy.
For patients presenting with clear, advanced structural lesions—such as a massive, space-occupying osteochondroma, a highly symptomatic Luschka tubercle, or a severely malunited rib fracture causing direct osseous impingement—the threshold for surgical intervention is considerably lower. In these cases, prolonged conservative management is futile and merely delays definitive mechanical resolution. In such scenarios, early surgical excision of the offending bony mass, coupled with a concurrent bursectomy, is the indicated standard of care to prevent progressive muscle damage and irreversible capsulolabral wear at the glenohumeral joint secondary to altered kinematics.
Contraindications must be strictly observed to avoid disastrous postoperative outcomes. Absolute contraindications include active local or systemic infection, severe medical comorbidities precluding safe prone positioning or anesthesia, and primary, uncorrected neurologic winging of the scapula (e.g., isolated long thoracic or spinal accessory nerve palsy not caused by a mass effect). Operating on a primarily denervated, winging scapula will not only fail to resolve the symptoms but will likely exacerbate the instability. Relative contraindications include poorly defined, diffuse pain without localizing signs, psychogenic pain disorders, and a lack of compliance with the rigorous postoperative rehabilitation protocols required for success.
| Category | Specific Clinical Scenarios |
|---|---|
| Absolute Indications | Failure of 6+ months of targeted periscapular physical therapy; highly symptomatic, radiographically confirmed osseous lesions (e.g., osteochondroma); significant, temporary pain relief from a targeted diagnostic bursal injection. |
| Relative Indications | Intractable grating crepitus interfering with activities of daily living or professional athletics; recalcitrant fibrotic bursitis confirmed on MRI in a compliant patient. |
| Absolute Contraindications | Active local or systemic infection; primary neurologic scapular winging (LTN, DSN, or SAN palsy); medical instability precluding prone positioning. |
| Relative Contraindications | Diffuse, non-localizing shoulder pain; failure to respond to a diagnostic injection; suspected cervical radiculopathy as the primary pain generator; severe psychiatric overlay or secondary gain issues. |
Pre-Operative Planning, Templating, and Patient Positioning
Effective surgical management of snapping scapula syndrome begins long before the patient enters the operating theater. Our preoperative planning is exhaustive, combining a meticulous clinical evaluation with a highly detailed, multi-modality imaging review. Clinically, patients typically present with deep, aching pain around the posterior shoulder girdle, which is reliably exacerbated by overhead activities, pushing movements, or repetitive reaching. The physical examination must actively seek palpable crepitus and localized tenderness, specifically palpating along the medial border and the superomedial angle while the patient actively protracts and retracts the shoulder.
Radiologic studies are the cornerstone of our preoperative templating, essential for ruling out or confirming bony abnormalities. Our initial screening tools are high-quality Anterior-Posterior (AP) and Tangential (Y) radiographic views of the scapula. These views are excellent for identifying gross bony lesions of the scapula body and the underlying ribs. However, plain films are often insufficient for surgical planning. Therefore, a Computed Tomography (CT) scan is mandatory whenever skeletal abnormalities are suspected. Three-dimensional (3D) CT reconstructions are absolutely invaluable; they allow the surgeon to virtually rotate the scapula, clearly visualizing the exact size, base, and spatial orientation of complex osteochondromas or subtle superomedial angulations, thereby dictating the extent of the necessary bony resection.
While the utility of Magnetic Resonance Imaging (MRI) is debated among some shoulder surgeons, I find it highly beneficial in cases of pure soft-tissue snapping. MRI excels at identifying the exact location and volume of inflamed, fluid-filled bursae, assessing for chronic muscle atrophy or fatty infiltration in the subscapularis, and ruling out rare soft-tissue lesions like a subscapular elastofibroma. Dynamic fluoroscopy can also be utilized in complex cases to visualize the snapping in real-time during simulated shoulder motion. Finally, Nerve Conduction Studies and Electromyography (NCS/EMG) are crucial if there is any clinical suspicion of primary neurologic injury contributing to scapular dyskinesia.

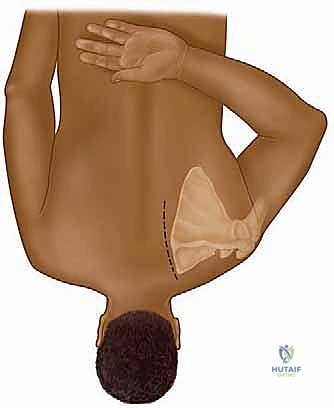
Patient positioning is a critical, highly specific step for both open and arthroscopic scapulothoracic techniques. The patient is carefully positioned prone on a specialized operating table. The positioning of the involved arm is the key to a successful procedure: the arm is meticulously placed in the "chicken-wing" position. This involves internal rotation of the shoulder with the dorsum of the hand tucked firmly against the patient's lower lumbar spine. This specific maneuver causes the scapula to dynamically wing outward and protract away from the posterior thorax. This dramatically opens the scapulothoracic interval, making the superomedial angle highly prominent and safely accessible, while simultaneously moving the medial border away from the dangerous neurovascular structures of the chest wall. We utilize customized chest rolls to maintain strict cervical and thoracic spinal alignment, and the head is supported in a neutral position to prevent any traction injury to the brachial plexus.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution for snapping scapula syndrome can be performed via an open or an arthroscopic approach. The choice of technique depends heavily on the underlying pathology. Massive bony lesions or complex revisions are typically best served by an open approach, whereas isolated bursitis, fibrotic bands, and minor superomedial bony prominent are ideally managed arthroscopically to minimize morbidity and accelerate rehabilitation.
Open Scapulothoracic Decompression
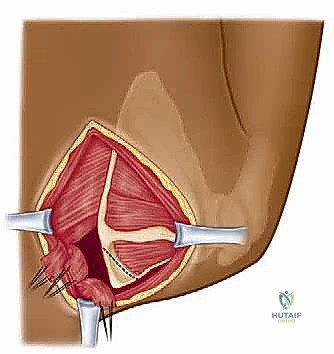
For the open technique, we begin with a precise longitudinal incision directly over the medial scapular edge, centered precisely at the level of the scapular spine. This incision typically measures 8 to 10 cm, tailored to the patient's body habitus and the planned resection volume. Subcutaneous tissues are meticulously undermined, creating full-thickness flaps to expose the superior portion of the scapula, extending cranially to the superomedial angle.
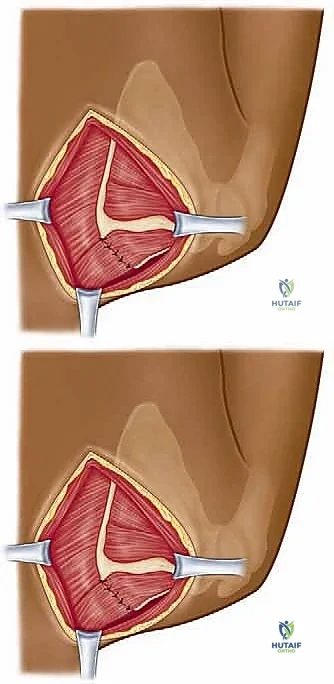
The next critical step is the trapezius split. Using needle-tip electrocautery, we identify the fascial plane and split the lower fibers of the trapezius in line with their direction, taking extreme care not to drift too far medially where the spinal accessory nerve arborizes. Once the trapezius is retracted, the rhomboid minor and the insertion of the levator scapulae are exposed.
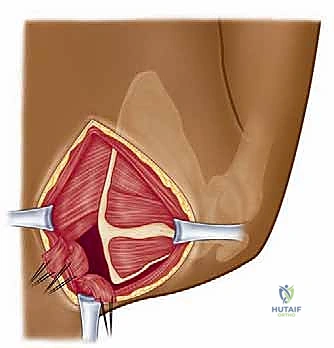
We then perform a sharp, subperiosteal detachment of the rhomboids and levator scapulae from the medial border and superomedial angle. It is during this specific step that the Dorsal Scapular Nerve is at its highest risk; the surgeon must stay strictly on the bone (subperiosteal) to avoid plunging into the medial soft tissues. Once the bone is exposed, a rongeur or an oscillating saw is utilized to resect the offending superomedial angle or osteochondroma. A standard resection typically involves removing a triangular wedge of bone measuring approximately 2 to 3 cm from the superomedial corner.
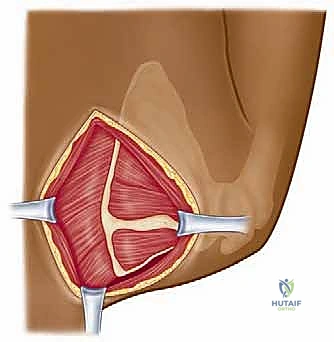
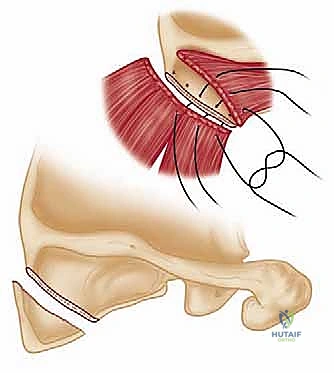
Following the bony resection, a meticulous, wide bursectomy is performed, excising all thickened, fibrotic bursal tissue from the supraserratus and infraserratus spaces using electrocautery and rongeurs. The bony edges are then heavily rasped and smoothed with bone wax to prevent future abrasion. The closure is as critical as the resection: the detached musculature must be securely repaired through transosseous drill holes in the remaining scapular border using heavy, non-absorbable sutures to prevent postoperative iatrogenic winging.
Arthroscopic Scapulothoracic Decompression
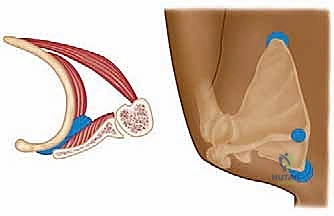
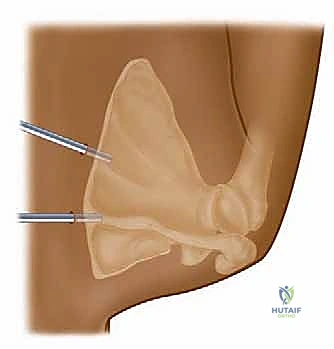
The arthroscopic approach is a masterclass in spatial awareness. With the patient in the prone "chicken-wing" position, bony landmarks (medial border, scapular spine, inferior angle) are meticulously outlined. We typically utilize two primary portals: a superior medial portal and an inferior medial portal. The inferior portal is established first, approximately 3 to 4 cm distal to the scapular spine and 2 to 3 cm medial to the medial border of the scapula. This lateralized placement is critical to avoid the DSN. A blunt trocar is used to carefully penetrate the trapezius and rhomboid musculature, entering the supraserratus space.
Once the camera is introduced, the superior portal is established under direct intra-articular visualization, usually just superior to the scapular spine. We strictly avoid portals superior to the superomedial angle to protect the Spinal Accessory Nerve. An arthroscopic pump is utilized, but fluid pressure must be strictly monitored (typically kept below 40-50 mmHg) to prevent massive fluid extravasation into the thoracic cavity or surrounding fascial planes.
The bursectomy is performed using a combination of an arthroscopic shaver and a radiofrequency ablation wand. The surgeon systematically clears the fibrotic, cobweb-like bursal tissue, working from the medial border laterally into the depths of the supraserratus and infraserratus spaces. The goal is to visualize the smooth, glistening muscle bellies of the subscapularis and serratus anterior.
If a bony resection is indicated, an arthroscopic burr or an acromionizer is introduced. The superomedial angle of the scapula is skeletonized using the radiofrequency wand, and the bone is resected from medial to lateral. The surgeon must constantly reference the depth of resection to avoid penetrating the anterior cortex of the scapula too aggressively, which risks injury to the underlying neurovascular structures.

Once the resection is complete, the arm is taken out of the "chicken-wing" position and dynamically moved through a full range of motion while visualizing the space arthroscopically to ensure that all mechanical impingement has been definitively eliminated.
Complications, Incidence Rates, and Salvage Management
While scapulothoracic decompression is highly successful when properly indicated, the surgeon must be acutely aware of the potential complications, which can be devastating. The most feared complication is iatrogenic nerve injury. Injury to the Dorsal Scapular Nerve (DSN) or Long Thoracic Nerve (LTN) can result in profound, often irreversible scapular winging. The incidence of nerve injury is generally reported to be low (< 2% in experienced hands), but the
