Scapulothoracic Arthrodesis: An Intraoperative Masterclass for Complex Scapular Dysfunction

Key Takeaway
This masterclass guides fellows through scapulothoracic arthrodesis, a salvage procedure for refractory scapular pain, crepitus, or winging. We cover comprehensive anatomy, meticulous patient positioning, and step-by-step intraoperative execution from incision to closure. Emphasis is placed on neurovascular protection, precise bony preparation, hardware application, and managing potential complications, ensuring a successful fusion for improved shoulder function and pain relief.
Comprehensive Introduction and Patho-Epidemiology
Scapulothoracic arthrodesis represents a formidable yet incredibly rewarding surgical intervention within the armamentarium of the advanced shoulder reconstructive surgeon. This procedure is unequivocally not a routine, everyday shoulder operation; rather, it is an end-stage salvage operation reserved for a highly specific and rigorously vetted cohort of patients. These individuals suffer from profound, debilitating scapulothoracic dysfunction, intractable periscapular pain, or refractory scapular winging that has categorically failed all conservative modalities and less invasive surgical measures, including complex regional muscle transfers such as the pectoralis major or Eden-Lange procedures. The profound loss of upper extremity function associated with an unstable scapula cannot be overstated, as the scapula serves as the essential dynamic fulcrum for all glenohumeral motion.
The patho-epidemiology of conditions necessitating scapulothoracic arthrodesis is diverse, encompassing both primary myopathic processes and devastating traumatic neuropathies. Facioscapulohumeral muscular dystrophy (FSHD) remains one of the most classic and well-documented indications for this procedure. In FSHD, progressive fatty infiltration and functional destruction of the periscapular stabilizers—particularly the serratus anterior, rhomboids, and trapezius—lead to profound bilateral winging. Without a stable base, the deltoid and rotator cuff, which are typically spared early in the disease process, cannot generate the necessary tension to elevate the arm, resulting in a functional pseudoparalysis of the upper extremity.
Beyond muscular dystrophies, traumatic or iatrogenic nerve palsies constitute a significant portion of the patient demographic requiring this salvage procedure. Irreversible injury to the long thoracic nerve (innervating the serratus anterior) or the spinal accessory nerve (innervating the trapezius) leads to distinct patterns of medial or lateral winging, respectively. When these nerve injuries prove refractory to neurolysis, nerve grafting, or subsequent dynamic tendon transfers, the scapula remains mechanically uncoupled from the thoracic wall. Furthermore, patients with severe, recalcitrant "snapping scapula" syndrome—characterized by painful crepitus secondary to severe bursitis, osteochondromas, or morphological rib deformities that have failed prior partial scapulectomies—may also become candidates for arthrodesis to definitively eliminate the painful articulation.

Detailed Surgical Anatomy and Biomechanics
The Scapulothoracic Articulation
Before any surgical incision is contemplated, a masterful understanding of the regional anatomy and biomechanics is absolutely mandatory. The scapulothoracic articulation is not a true diarthrodial synovial joint; it lacks a joint capsule and hyaline cartilage. Instead, it is a complex physiological articulation where the concave anterior surface of the scapula glides smoothly over the convex posterolateral aspect of the thoracic rib cage, typically spanning from the second to the seventh ribs. This articulation is suspended anteriorly by the clavicle via the acromioclavicular and coracoclavicular ligaments, forming a critical strut that maintains the scapula at its optimal resting position on the posterior thorax.
The scapula itself is an anatomically complex, flat bone that serves as the origin or insertion point for no fewer than 17 distinct muscles. These muscles are functionally categorized into force couples that dictate the highly coordinated, multi-planar movements of the scapula: protraction, retraction, elevation, depression, and upward/downward rotation. The trapezius, rhomboids, levator scapulae, serratus anterior, and pectoralis minor work in an intricate, synergistic balance to dynamically position the glenoid during arm elevation. Disruption of this delicate muscular balance, whether through denervation, myopathy, or direct trauma, immediately destabilizes the glenohumeral fulcrum, leading to the profound dysfunction we aim to correct with arthrodesis.
A specialized, multi-layered bursal system normally separates the anterior surface of the scapula from the underlying rib cage, facilitating frictionless gliding during upper extremity motion. The two primary bursae are the supraserratus bursa (located between the subscapularis and serratus anterior) and the infraserratus bursa (situated between the serratus anterior and the posterolateral chest wall). In pathological states, these bursal layers can become hypertrophic, fibrotic, or scarred, leading to the painful, audible crepitus characteristic of snapping scapula syndrome. During arthrodesis, these gliding planes must be meticulously obliterated to achieve rigid bony apposition.
Neurovascular Considerations
The surgical approach to the scapulothoracic interval is fraught with potential neurovascular hazards that demand the utmost respect and vigilance. The long thoracic nerve, derived from the anterior rami of C5, C6, and C7, is arguably the most critical structure at risk during the deep dissection. It courses inferiorly along the superficial (lateral) surface of the serratus anterior muscle. Because our arthrodesis preparation requires partial resection of the serratus anterior to expose the anterior scapular cortex, the surgeon must remain acutely aware of this nerve's trajectory to avoid iatrogenic injury, which would ironically worsen any residual stabilizing function the muscle might possess.
The spinal accessory nerve (Cranial Nerve XI) provides the sole motor innervation to the trapezius muscle. It courses along the deep surface of the trapezius, entering the muscle superiorly and medially. During our initial exposure, the trapezius must be meticulously elevated and retracted laterally or medially depending on the specific approach variant. Aggressive retraction or careless dissection in the superior aspect of the wound can easily stretch or transect this nerve, leading to devastating lateral winging and further functional compromise. Additionally, the dorsal scapular nerve and artery, which supply the rhomboids and levator scapulae, course along the medial border of the scapula and must be carefully identified and protected or selectively ligated during the release of the medial periscapular musculature.
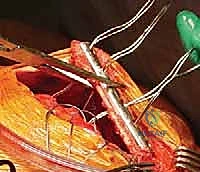
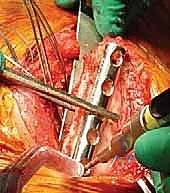
Perhaps the most immediately life-threatening anatomical structures encountered during this procedure are the intercostal neurovascular bundles and the underlying parietal pleura. The intercostal vein, artery, and nerve run in the subcostal groove along the inferior border of each respective rib. When passing cerclage wires, cables, or heavy sutures around the ribs to secure the scapula, the surgeon must maintain a strict subperiosteal plane. Straying from this plane risks lacerating the intercostal artery, resulting in massive, difficult-to-control hemorrhage, or breaching the exceedingly thin parietal pleura, causing an immediate tension pneumothorax.

Exhaustive Indications and Contraindications
Clinical Evaluation and Diagnostic Criteria
The decision to proceed with a scapulothoracic arthrodesis is never made lightly and requires an exhaustive, multi-disciplinary clinical evaluation. Patients typically present with a primary complaint of debilitating, unrelenting periscapular pain, profound shoulder fatigue, and a dramatic loss of active forward elevation and abduction. On physical examination, the surgeon must meticulously evaluate the entire shoulder girdle, observing both scapulae at rest and dynamically. We specifically look for the classic signs of medial winging (indicative of serratus anterior dysfunction) or lateral winging (indicative of trapezius palsy) during provocative maneuvers such as wall push-ups or resisted forward flexion.
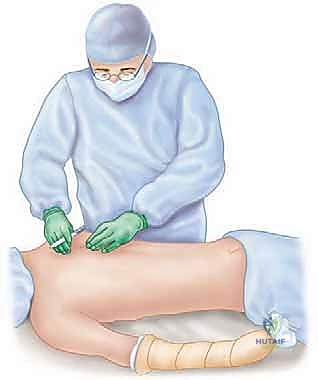
The cornerstone of the physical examination for these patients is the "scapular stabilization test." During this maneuver, the examiner stands behind the patient and manually compresses the scapula firmly against the posterior thoracic wall, physically reducing the winging and stabilizing the fulcrum. The patient is then asked to actively elevate their arm. A positive test is characterized by a dramatic, immediate improvement in active forward elevation and a significant reduction in pain (typically ≥75% relief). This test essentially simulates the biomechanical outcome of a successful arthrodesis; a strongly positive result is highly predictive of a favorable surgical outcome and serves as a primary justification for proceeding with the fusion.
Diagnostic imaging and neurophysiological studies are mandatory to confirm the underlying etiology and plan the surgical intervention. Electromyography (EMG) and Nerve Conduction Velocity (NCV) studies are critical for documenting the precise extent, severity, and chronicity of neurologic dysfunction, particularly distinguishing between isolated nerve palsies and broader myopathic processes like FSHD. For patients presenting primarily with painful crepitus rather than gross instability, a targeted diagnostic injection of a local anesthetic (e.g., 1% lidocaine) into the scapulothoracic bursa under fluoroscopic or ultrasound guidance can definitively isolate the articulation as the primary pain generator.

Indications and Contraindications Table
The criteria for surgical intervention must be strictly adhered to, as the procedure permanently alters the biomechanics of the shoulder girdle. Arthrodesis sacrifices roughly one-third of total shoulder elevation (the scapulothoracic contribution) to salvage the remaining two-thirds (the glenohumeral contribution). Therefore, the glenohumeral joint must be relatively preserved and functional to justify the procedure.
| Category | Specific Clinical Scenarios | Rationale / Considerations |
|---|---|---|
| Primary Indications | Facioscapulohumeral muscular dystrophy (FSHD) with severe bilateral or unilateral winging. | Restores a stable fulcrum for the preserved deltoid, drastically improving active elevation and function. |
| Irreducible, fixed scapular winging secondary to traumatic long thoracic or spinal accessory nerve palsy. | Indicated only after failure of conservative management and dynamic muscle transfers (e.g., Eden-Lange). | |
| Disabling, refractory "snapping scapula" syndrome with intractable pain. | Reserved for cases failing extensive non-operative care and prior arthroscopic/open bursectomy or scapulectomy. | |
| Salvage of failed prior periscapular reconstructive surgeries. | Provides definitive, rigid stabilization when soft tissue reconstructive options have been exhausted. | |
| Absolute Contraindications | Active local or systemic infection. | Risk of deep hardware infection and catastrophic osteomyelitis of the ribs/scapula. |
| Severe, concurrent glenohumeral arthropathy or massive, irreparable rotator cuff tear. | Fusing the scapula in the presence of a non-functional glenohumeral joint will result in a completely flail, useless extremity. | |
| Medical unfitness for prolonged general anesthesia in the prone position. | The procedure requires significant operative time, selective lung ventilation, and carries cardiopulmonary risks. | |
| Relative Contraindications | Severe osteoporosis or metabolic bone disease. | High risk of hardware pull-out, rib fractures during cerclage tightening, and ultimate nonunion. |
| Non-compliant patient or inability to adhere to strict postoperative immobilization. | The fusion mass is subjected to constant respiratory motion; strict adherence to bracing is vital for union. |
Pre-Operative Planning, Templating, and Patient Positioning
Imaging Modalities and Diagnostic Injections
Preoperative planning for a scapulothoracic arthrodesis is highly complex and requires a comprehensive suite of advanced imaging modalities. Standard plain radiographs, including true anteroposterior (AP) views in internal and external rotation, axillary lateral, and scapular Y views, are obtained to evaluate the overall bony architecture of the shoulder girdle. These initial films help rule out concurrent glenohumeral pathology, assess the integrity of the clavicle and acromioclavicular joint, and identify gross structural abnormalities of the ribs or scapula. However, plain films are insufficient for detailed preoperative templating of the fusion bed.
High-resolution Computed Tomography (CT) scans with multi-planar (axial, coronal, and sagittal) and three-dimensional (3D) volume-rendered reformations are the gold standard for preoperative planning. The CT scan provides exquisite detail of the patient's unique scapular morphology and the specific contours of the underlying rib cage. This allows the surgeon to virtually map the optimal fusion surface, identifying which ribs (typically ribs 3 through 6) will provide the best bony apposition against the anterior scapular cortex. Furthermore, the CT scan is crucial for assessing bone stock, identifying any occult exostoses, and evaluating the degree of thoracic kyphosis or scoliosis, which can significantly alter the required angle of scapular positioning during fixation.
In cases where the primary indication is intractable pain rather than gross instability, diagnostic injections play a pivotal role. Under fluoroscopic or ultrasound guidance, a long spinal needle is advanced into the scapulothoracic bursal space, typically targeting the superomedial or inferomedial angle. The injection of a short-acting local anesthetic (such as 1% lidocaine or bupivacaine) serves as a highly specific diagnostic tool. If the patient experiences profound, immediate relief of their periscapular pain following the injection, it confirms the scapulothoracic articulation as the primary pain generator, thereby strongly supporting the rationale for arthrodesis.
Anesthesia, Setup, and Patient Positioning
The anesthetic management and patient positioning for this procedure demand meticulous attention to detail and close collaboration with the anesthesiology team. General endotracheal anesthesia is mandatory. Crucially, the airway must be secured with a double-lumen endotracheal tube. This is a non-negotiable requirement for this operation. The double-lumen tube allows for selective, independent ventilation of the lungs, enabling the anesthesiologist to intentionally deflate the ipsilateral lung during the critical phases of rib preparation and cerclage wire passage. Deflating the lung dramatically reduces the risk of iatrogenic pneumothorax or parenchymal lung injury when instruments are passed deep to the ribs.
Patient positioning is equally critical to the success of the operation. The patient is carefully transferred to a radiolucent operating table in the prone position. Meticulous padding of all dependent bony prominences—including the face, elbows, knees, and anterior superior iliac spines—is essential to prevent devastating pressure sores or peripheral nerve neurapraxias during the lengthy procedure. A dedicated chest roll or specialized prone positioning frame is utilized to ensure the abdomen hangs free, minimizing inferior vena cava compression and reducing epidural venous bleeding.
The surgical prep and drape must be extensive. The entire involved upper extremity must be prepped free, allowing the surgeon to dynamically manipulate the arm throughout the procedure. The sterile field must extend medially well past the spinous processes of the thoracic vertebrae, superiorly to the base of the neck, and inferiorly to include the ipsilateral posterior superior iliac spine (PSIS). Inclusion of the PSIS in the sterile field is absolutely mandatory, as the harvesting of copious amounts of autologous cancellous bone graft from the posterior iliac crest is a vital step in achieving a successful, robust arthrodesis.
Step-by-Step Surgical Approach and Fixation Technique
Incision and Superficial Dissection
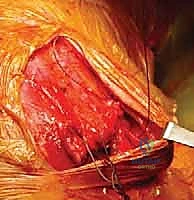
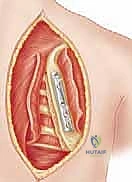
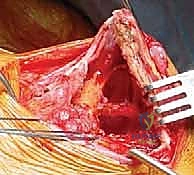
The surgical approach begins with a meticulously planned curvilinear incision. The incision is centered over the medial border of the scapula, beginning just superior to the medial root of the scapular spine and extending distally, curving gently to follow the contour of the medial border down to the inferior angle. This expansile incision provides unparalleled, direct access to both the medial scapula and the underlying thoracic cage. Hemostasis is achieved meticulously as the incision is carried down through the subcutaneous tissues to the level of the deep investing fascia.
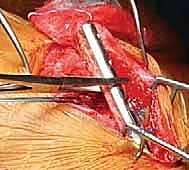
Upon incising the superficial fascia, the broad, flat, descending fibers of the trapezius muscle are immediately encountered. Utilizing a combination of sharp dissection and electrocautery, the trapezius is carefully elevated off the underlying musculature and retracted. Depending on the exact trajectory of the incision, the trapezius may be split in line with its fibers or mobilized as a full-thickness flap. Extreme care must be taken during the superior aspect of this mobilization to avoid any traction injury to the spinal accessory nerve. Once the trapezius is adequately retracted, the underlying rhomboid major and minor muscles, which insert along the medial border of the scapula, are widely exposed.
The next critical step involves the release of the medial periscap
Clinical & Radiographic Imaging Archive