AC Joint Injury? Effective Healing with a Clavicle Strap Sling
Key Takeaway
In this comprehensive guide, we discuss everything you need to know about AC Joint Injury? Effective Healing with a Clavicle Strap Sling. An Acromioclavicular (AC) joint injury involves trauma to the joint connecting the lateral clavicle and medial acromion, frequently from a direct fall onto the shoulder. It typically presents with a downward shoulder sag, visible step-off deformity, and pain, diagnosed via clinical exam and X-rays. A clavicle strap sling provides crucial support and immobilization for these injuries, aiding healing and comfort.
AC Joint Injury Effective Healing with a Clavicle Strap Sling
Introduction and Epidemiology
Acromioclavicular (AC) joint injuries represent a significant and frequently encountered challenge in orthopedic trauma. These injuries often affect a young, active population, with a predominant association with contact athletic activities. Understanding the epidemiology, biomechanics, and comprehensive management spectrum of AC joint injuries is crucial for optimal patient outcomes.
Historically, AC joint dislocations represent a substantial proportion of acute traumatic injuries to the shoulder girdle, accounting for approximately 9% to 10% of such presentations. The demographic profile is skewed towards the second decade of life, corresponding with periods of high athletic engagement. A marked gender disparity is observed, with males affected approximately five times more frequently than females, reflecting higher participation rates in contact sports and occupations prone to direct shoulder trauma. While often considered a sports injury, falls from height, motor vehicle accidents, and industrial accidents also contribute to the incidence.
The spectrum of AC joint injuries ranges from mild sprains (Rockwood Type I) to severe dislocations (Rockwood Type VI), each necessitating a tailored approach to management. While non-operative treatment with immobilization, often involving a clavicle strap sling, remains the cornerstone for lower-grade injuries, higher-grade dislocations frequently require surgical intervention to restore stability and function. This comprehensive review will delve into the nuanced anatomical considerations, diagnostic principles, surgical indications, meticulous operative techniques, potential complications, and structured rehabilitation protocols pertinent to the effective management of AC joint injuries.
Surgical Anatomy and Biomechanics
The acromioclavicular joint is a critical component of the shoulder girdle, facilitating scapular motion and stability. Understanding its intricate anatomy and biomechanics is fundamental to comprehending injury mechanisms and guiding therapeutic interventions.
Acromioclavicular Joint Architecture
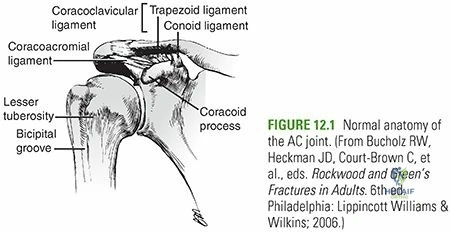
The AC joint is classified as a diarthrodial joint, characterized by fibrocartilage-covered articular surfaces articulating between the lateral end of the clavicle and the medial acromion. Unlike many synovial joints, the plane of the AC joint can exhibit variability, ranging from nearly vertical to an inclination medially by as much as 50 degrees. This variability can influence the joint's intrinsic stability and predisposition to specific injury patterns.
Within the joint, a meniscoid intra-articular disc is typically present. This disc contributes minimally to the joint's overall stability and undergoes age-dependent degeneration, often becoming essentially nonfunctional beyond the fourth decade of life. The thin fibrous capsule surrounding the joint is reinforced significantly by four capsular ligaments: anterior, posterior, superior, and inferior AC ligaments. The superior AC ligament is further strengthened by the blending fibers of the deltoid and trapezius muscles, which contribute to the joint's stability, particularly against superior translation.
Ligamentous Stabilizers and Biomechanics
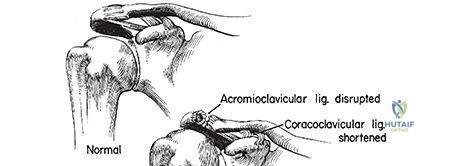
The stability of the AC joint is conferred by two primary ligamentous complexes: the acromioclavicular (AC) ligaments and the coracoclavicular (CC) ligaments.
- Acromioclavicular Ligaments: These ligaments, intrinsic to the joint capsule, are the primary restraints to horizontal stability (anterior and posterior translation) of the clavicle relative to the acromion.
- Coracoclavicular Ligaments: Comprising the conoid and trapezoid ligaments, these extrinsic ligaments are the principal stabilizers against vertical displacement of the clavicle relative to the scapula. The conoid ligament is positioned more medially and posteriorly, resisting posterior rotation and superior displacement. The trapezoid ligament is more lateral and anterior, resisting anterior rotation and superior displacement. The average coracoclavicular distance, measured radiographically from the superior cortex of the coracoid process to the inferior cortex of the clavicle, typically ranges from 1.1 to 1.3 cm in an uninjured shoulder. A significant increase in this distance is a hallmark of CC ligament disruption.
- Secondary Stabilizers: The fascial attachments of the deltoid and trapezius muscles to the clavicle and acromion, particularly reinforcing the superior AC ligament, act as secondary stabilizers, contributing to both horizontal and vertical stability.
- Joint Kinematics: The AC joint allows for subtle motion, including rotation (upward/downward, internal/external) and translation (anterior/posterior, superior/inferior), which is crucial for full scapulothoracic rhythm and overall shoulder mobility, especially during arm elevation. Disruption of this intricate stability significantly impairs shoulder function.
Mechanism of Injury
AC joint injuries primarily result from two distinct mechanisms:
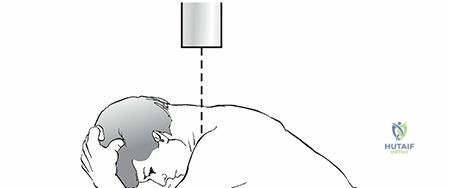
- Direct Mechanism: This is the more common etiology, typically involving a direct fall onto the superior aspect of the shoulder with the arm adducted. The force drives the acromion inferiorly and medially relative to the clavicle, sequentially disrupting the AC ligaments and then the CC ligaments. The energy transmitted can also cause displacement of the distal clavicle superiorly.
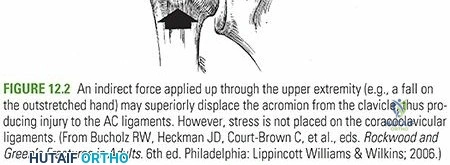
- Indirect Mechanism: Less frequent, this mechanism involves a fall onto an outstretched hand (FOOSH) with force transmission through the humeral head and glenohumeral joint, then into the AC articulation. This can lead to compression or shear forces across the joint, potentially disrupting the ligaments.
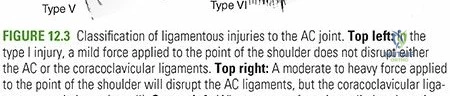
Rockwood Classification System
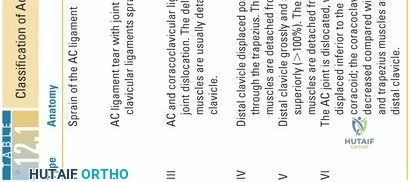
The Rockwood classification system is the most widely adopted method for categorizing AC joint injuries, guiding both diagnosis and treatment decisions.
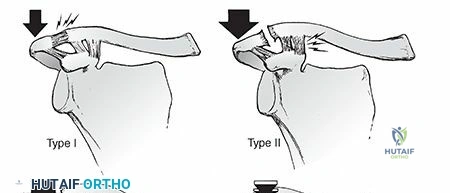
- Type I: Sprain of the AC ligaments, capsule intact, minimal displacement. CC ligaments intact.
- Type II: Complete tear of the AC ligaments and capsule. CC ligaments intact but sprained. Subluxation of the AC joint, but the coracoclavicular distance is normal or minimally increased. The clavicle is superiorly displaced but remains above the superior aspect of the acromion.
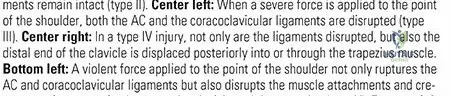
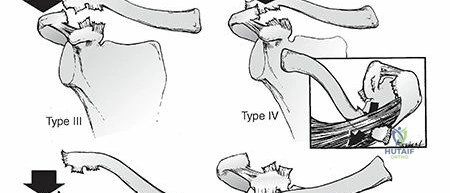
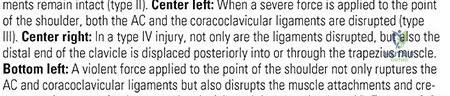
- Type III: Complete disruption of both AC and CC ligaments. Significant superior displacement of the clavicle, typically 25% to 100% greater than the contralateral CC distance. The clavicle is above the superior aspect of the acromion. The deltoid and trapezius fascia may be partially detached.
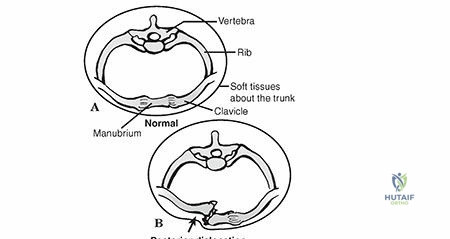
- Type IV: Complete disruption of AC and CC ligaments. The clavicle is displaced posteriorly into or through the trapezius muscle, often buttonholing through the fascia. This displacement is best visualized on an axillary lateral radiograph.
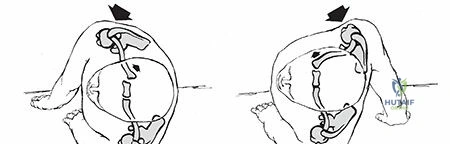
- Type V: Complete disruption of AC and CC ligaments, with severe superior displacement of the clavicle. The soft tissue envelope (deltoid and trapezius attachments) is extensively stripped from the distal clavicle and acromion, resulting in significant superior displacement (often >100% increase in CC distance).
- Type VI: Extremely rare. Complete disruption of AC and CC ligaments, with inferior displacement of the clavicle beneath the coracoid process or acromion. This is a severe injury requiring significant force.
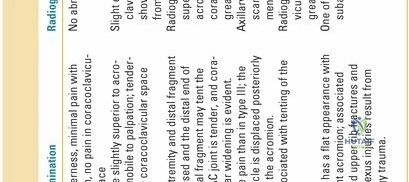
Thorough clinical evaluation, combined with appropriate radiographic imaging (including AP, lateral, axillary, and Zanca views, with stress radiographs in some cases), is essential for accurate classification and treatment planning.
Indications and Contraindications
The decision-making process for managing AC joint injuries is nuanced, weighing injury severity, patient factors, and functional demands. While non-operative treatment is preferred for lower-grade injuries, surgical intervention is indicated for specific higher-grade dislocations and cases of failed conservative management.
Non-Operative Management Indications
The majority of AC joint injuries, particularly lower-grade sprains and subluxations, are effectively managed non-operatively. The primary goals are pain control, protection of the healing tissues, and restoration of function.
- Rockwood Type I: These are simple sprains of the AC ligaments without significant disruption or instability.
- Rockwood Type II: Characterized by complete AC ligament disruption but intact CC ligaments, resulting in AC joint subluxation. While some argue for surgical fixation, the consensus for most patients remains non-operative.
- Rockwood Type III (Controversial): For many patients, particularly those with low functional demands, a sedentary lifestyle, or older individuals, Type III injuries can be managed non-operatively with good to excellent results. The natural history often involves residual deformity but acceptable function. However, the controversy lies in the outcome for high-demand athletes or laborers, where surgical intervention may provide superior outcomes regarding endurance and overhead activities, albeit with potential surgical risks. The initial treatment often involves a trial of non-operative care.
Non-operative Strategy:
Initial management involves:
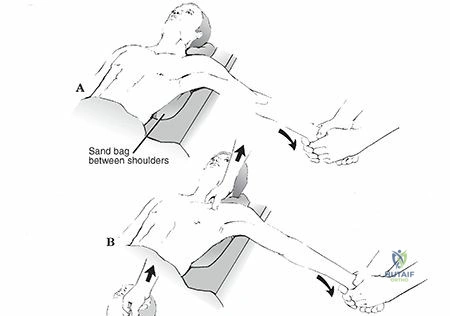
* Sling Immobilization: A simple arm sling or a specialized clavicle strap sling (often figure-of-eight style or a commercially available AC joint brace) is used for comfort and to support the arm, reducing tension on the healing ligaments. The clavicle strap sling aims to push the clavicle down, though its effectiveness in maintaining reduction or preventing later deformity is limited; its primary role is comfort and support.
* Pain Management: NSAIDs, analgesics, and ice application.
* Early Motion: Progressive range of motion exercises initiated as pain allows, typically within 1-2 weeks for Type I/II and 2-4 weeks for Type III.
* Rehabilitation: Gradual strengthening of shoulder girdle musculature, focusing on scapular stabilizers.
Operative Management Indications
Surgical intervention is generally reserved for higher-grade injuries, specific patient populations, or cases where conservative treatment has failed. The goal of surgery is to restore anatomical alignment, provide stable fixation, facilitate ligamentous healing, and optimize long-term shoulder function.
- Rockwood Type III (Specific Cases):
- High-demand overhead athletes or laborers: These individuals may benefit from surgical stabilization to ensure robust return to sport/work and reduce the risk of chronic pain or fatigue.
- Young, active individuals: To potentially prevent long-term functional deficits or early degenerative changes.
- Persistent pain or functional impairment after failed non-operative treatment: For those who continue to experience significant symptoms despite an adequate trial of conservative care.
- Rockwood Type IV: The clavicle is buttonholed posteriorly through the trapezius. This anatomical disruption prevents closed reduction and necessitates open surgical reduction and stabilization.
- Rockwood Type V: Characterized by severe superior displacement and extensive stripping of the deltoid and trapezius fascia. Surgical reduction and stabilization are almost always indicated to restore the deltotrapezial envelope and achieve adequate function.
- Rockwood Type VI: An extremely rare injury with inferior displacement of the clavicle. Requires surgical intervention due to severe anatomical disruption and potential neurovascular compromise.
- Chronic Instability/Pain: Patients presenting with symptomatic chronic AC joint instability or painful degenerative changes (e.g., osteolysis of the distal clavicle) following a previous injury may warrant surgical intervention, which could include distal clavicle excision, ligament reconstruction, or both.
Contraindications for Surgical Management
While not absolute for all types of injuries, certain factors may contraindicate or make surgical intervention less desirable:
- Absolute Contraindications:
- Active local or systemic infection.
- Severe comorbidities precluding safe anesthesia or surgery (e.g., uncontrolled cardiac disease, severe pulmonary dysfunction).
- Unwillingness or inability of the patient to comply with post-operative rehabilitation protocols.
- Relative Contraindications:
- Advanced age (often associated with lower functional demands and higher surgical risks).
- Severe osteopenia/osteoporosis (may compromise hardware fixation).
- Significant soft tissue compromise at the surgical site.
- Extremely low functional demands where non-operative management provides acceptable outcomes with less risk.
Table 1: Operative vs. Non-Operative Indications for AC Joint Injuries
| Rockwood Type | Non-Operative Management | Operative Management |
|---|---|---|
| Type I | Primary Management: Sling, RICE, early ROM, rehabilitation. | Rarely indicated. |
| Type II | Primary Management: Sling, RICE, early ROM, rehabilitation. | Rare; considered only for persistent severe pain or functional limitation. |
| Type III | Common: Sling, pain control, rehabilitation. Preferred for low-demand, older, or sedentary patients. Often a trial of conservative care. | Considered for: High-demand athletes/laborers, young active patients, failed non-operative treatment, significant functional deficits. |
| Type IV | Not indicated. Anatomical obstruction to closed reduction. | Primary Management: Open reduction and stabilization. |
| Type V | Not indicated. Severe displacement and soft tissue disruption. | Primary Management: Open reduction and stabilization. |
| Type VI | Not indicated. Severe displacement and potential neurovascular compromise. | Primary Management: Open reduction and stabilization. |
| Chronic | For stable, asymptomatic cases or mild symptoms. | Persistent pain, instability, symptomatic distal clavicle osteolysis. |
Pre Operative Planning and Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are crucial for successful AC joint reconstructive surgery. These steps minimize surgical time, optimize visualization, and reduce the risk of complications.
Pre-Operative Assessment
A comprehensive pre-operative assessment involves a detailed history and physical examination, focusing on neurovascular status of the upper extremity, assessment of any skin integrity issues, and careful documentation of the range of motion and pain. Imaging studies are reviewed thoroughly:
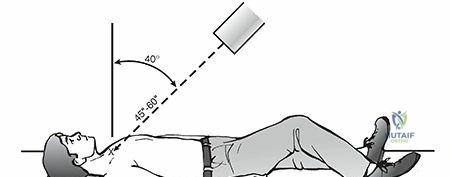
- Standard Radiographs: AP, lateral, and axillary views of the shoulder, along with a dedicated Zanca view (10-15 degrees cephalic tilt) to isolate the AC joint. Contralateral shoulder views are often obtained for comparison of coracoclavicular distance. Stress views (with weights) can be helpful for equivocal Type II/III injuries to unmask instability, though their routine use is debated due to discomfort and potential for false positives/negatives.
- CT Scans: Indicated for Type IV injuries to delineate posterior clavicular displacement and buttonholing through the trapezius, and for complex fracture patterns involving the distal clavicle or acromion.
- MRI Scans: While not routinely necessary for acute classification, MRI can provide detailed information regarding ligamentous integrity (AC and CC ligaments), muscle tears, and associated soft tissue injuries, which may influence surgical planning in select cases or for chronic pain evaluation.
Patient comorbidities should be identified and optimized prior to surgery. Discussion with the patient regarding realistic expectations, potential complications, and the prolonged rehabilitation period is paramount. Informed consent should detail the chosen surgical technique and alternatives. Antibiotic prophylaxis is administered pre-operatively as per institutional guidelines.
Patient Positioning
The choice of patient positioning depends on surgeon preference, the specific technique planned, and the patient's body habitus.
- Beach Chair Position: This is the most common position for AC joint reconstruction.
- Advantages: Allows for easy access to the superior aspect of the shoulder, comfortable for the patient, and permits dynamic assessment of shoulder range of motion and stability intra-operatively. It also allows for potential arthroscopy of the glenohumeral joint if indicated.
- Setup: The patient is placed in a semi-recumbent position (30-60 degrees of back elevation). The head is secured in a well-padded headrest, maintaining a neutral position to prevent brachial plexus stretching. The involved arm is free-draped, allowing for full range of motion. The operative field includes the lateral neck, supraclavicular fossa, deltoid region, and potentially the ipsilateral hip (for autograft harvest, if planned). Pressure points (e.g., sacrum, heels, contralateral arm) are meticulously padded. Blood pressure monitoring in the non-operative arm or lower extremity is crucial, as hypotension can occur in this position.
- Lateral Decubitus Position: Less commonly used for primary AC reconstruction but can be an option if combined with glenohumeral arthroscopy or for specific approaches.
- Advantages: May provide slightly better exposure of the coracoid if extensive subcoracoid work is anticipated, and avoids the hypotensive risk associated with beach chair.
- Setup: The patient is positioned laterally on the non-operative side, with appropriate padding at the axilla and bony prominences. The operative arm is supported in traction.
Regardless of position, the entire shoulder and chest wall are prepped and draped to allow for adequate exposure and intra-operative manipulation of the shoulder girdle. Bony landmarks such as the acromion, distal clavicle, coracoid process, and sternal notch are clearly palpable and marked.

Detailed Surgical Approach and Technique
Surgical techniques for AC joint reconstruction have evolved significantly, aiming to restore both horizontal and vertical stability, facilitate ligament healing, and provide durable fixation. Modern approaches often combine direct AC joint repair/reconstruction with robust coracoclavicular (CC) ligament reconstruction.
Surgical Incision and Exposure
- Incision: A curvilinear or transverse incision, approximately 5-7 cm in length, is typically made over the superior aspect of the AC joint, centered on the distal clavicle and acromion. A curvilinear incision starting from the posterolateral acromion, curving medially over the AC joint and along the superior aspect of the clavicle, often provides excellent exposure and hides well cosmetically.
- Dissection: The incision is carried down through the skin and subcutaneous tissue. The superficial fascia is incised, and the deltoid and trapezius muscles are identified. For Types IV and V injuries, the deltotrapezial fascia is typically torn, requiring careful identification of the muscle edges. The interval between the deltoid and trapezius is developed superiorly to expose the AC joint capsule and distal clavicle. Care is taken to identify and protect the supraclavicular nerves traversing this region.
- Visualization: The distal clavicle, acromion, and the remnants of the AC ligaments are visualized. For CC ligament reconstruction, the deep dissection proceeds inferiorly and medially from the clavicle to identify the coracoid process. This often involves blunt dissection through the deltoid muscle fibers and careful identification of the pectoralis minor insertion onto the coracoid. The conoid and trapezoid insertions on the clavicle (conoid tubercle, trapezoid line) should also be identified.
Reduction of the AC Joint
The primary goal is to achieve an anatomical or near-anatomical reduction of the distal clavicle relative to the acromion and coracoid.
- Direct Reduction: The clavicle is grasped with a reduction clamp (e.g., bone-holding forceps or a towel clip) and manipulated to reduce its superior, posterior, or inferior displacement. For superior dislocations, downward pressure on the clavicle and upward pressure on the elbow (if the arm is mobile) can aid reduction. For Type IV injuries, the clavicle must be meticulously extracted from its buttonholed position within the trapezius.
- Temporary Fixation: Once reduced, the position is held with a provisional fixation, such as a K-wire traversing the AC joint. This temporary fixation ensures stability during the reconstruction of the CC ligaments. Careful placement of K-wires is essential to avoid neurovascular structures and to ensure adequate bony purchase.

Illustrates initial incision and dissection over the AC joint.
Depicts reduction of the clavicle into anatomical alignment.
Coracoclavicular Ligament Reconstruction Techniques
Restoring vertical stability by reconstructing the CC ligaments is paramount for durable AC joint fixation. Multiple techniques exist.
1. Anatomic Coracoclavicular Reconstruction (ACCR) with Suture Buttons
This is a contemporary and increasingly favored technique that aims to replicate the anatomical footprint and function of both the conoid and trapezoid ligaments.
-
Coracoid Tunnel Preparation: A small portal or open approach is used to access the base of the coracoid. Two drill holes (typically 2.5-3.5 mm) are created through the coracoid, positioned anatomically to mimic the origins of the conoid and trapezoid ligaments. These holes are then connected to the superior surface of the clavicle.
Depicts suture button placement through coracoid and clavicle. -
Clavicle Tunnel Preparation: Two corresponding drill holes are created in the clavicle, precisely positioned at the anatomical insertion sites of the conoid and trapezoid ligaments. These holes are angled to align with the coracoid tunnels. A single large tunnel or two smaller diverging tunnels can also be utilized in the clavicle depending on the system used.
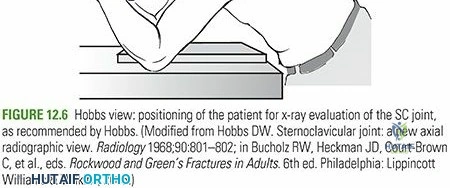
Illustration showing drilling of clavicular tunnels for CC reconstruction.
Another view of clavicular tunnel preparation for CC fixation. -
Graft Passage: High-strength sutures (e.g., FiberWire) pre-loaded onto a cortical button (e.g., TightRope system) are passed through the clavicular tunnels, then through the coracoid tunnels, and finally secured with a second cortical button on the inferior aspect of the coracoid.

Shows suture passing from clavicle through the coracoid. -
Tensioning and Fixation: With the AC joint manually reduced, the sutures are tensioned, and the buttons are flipped and secured. This provides robust vertical stability. The tension should be sufficient to reduce the clavicle but avoid over-compression, which could lead to complications like coracoid fracture or loss of clavicular motion.
Illustrates the final tightened construct with suture buttons.
Another image showing the suture button fixation providing vertical stability.
Demonstrates the secure reduction and fixation with suture buttons.

Radiographic appearance of dual suture button fixation. -
Autograft/Allograft Augmentation: For chronic injuries or very high-demand patients, the suture button system can be augmented with a tendon autograft (e.g., semitendinosus) or allograft. The graft is passed through the same tunnels as the sutures, providing biological reconstruction of the CC ligaments.

Depicts a graft being passed through the coracoid for augmentation.
Illustrates graft passage through the clavicle.
Shows the final graft and suture button construct.
2. Hook Plate Fixation
A hook plate is a non-anatomic but biomechanically strong fixation method providing temporary stabilization.
- Application: The hook of the plate is seated under the acromion, and the plate shaft is fixed to the superior surface of the distal clavicle with screws.

Demonstrates a hook plate in situ providing temporary AC joint fixation. - Considerations: This method provides excellent initial stability but requires a second surgery for hardware removal (typically 3-6 months post-operatively) to prevent subacromial impingement, acromial osteolysis, or plate breakage. It does not directly reconstruct the CC ligaments, relying on biological healing of native ligaments.
3. Weaver-Dunn Procedure (Modified)
A historical technique, often augmented, involving transferring the coracoacromial (CA) ligament from the acromion to the distal clavicle to reconstruct the CC ligaments.
- Original: Involved detachment of the CA ligament from the acromion and transfer to the distal clavicle.
- Modified: Often combined with a loop of suture or graft around the coracoid and clavicle to provide additional vertical stability, as the CA ligament itself is biomechanically inferior to the native CC ligaments.
AC Ligament Repair and Augmentation
Once vertical stability is restored via CC reconstruction, the torn AC ligaments and deltotrapezial fascia are meticulously repaired.
-
Direct Repair: The remnants of the superior and inferior AC ligaments and the deltotrapezial fascia are directly repaired using strong non-absorbable sutures. This helps to restore horizontal stability and reinforce the superior aspect of the joint.
Depicts repair of the AC ligaments and deltotrapezial fascia.
Another illustration of the final repair of the soft tissue envelope.
Shows the closure of the deltotrapezial fascia over the reconstructed joint. -
AC Joint K-wire Fixation (Temporary): Some surgeons may opt to place temporary K-wires across the AC joint in addition to CC reconstruction, particularly for very unstable injuries, though this is less common with robust CC reconstruction techniques. These wires must be removed.
Distal Clavicle Excision (DCE) / Mumford Procedure
This procedure involves resecting the distal 1-1.5 cm of the clavicle.
- Indications: Primarily for chronic symptomatic distal clavicle osteolysis or painful AC joint arthritis that has failed conservative management. It can be performed as an open or arthroscopic procedure.
- Technique: A small osteotomy is performed on the distal clavicle, and the fragment is removed. Care is taken to preserve the CC ligaments if they are intact and asymptomatic.
Illustrates the principle of distal clavicle excision.
Shows the removal of the distal clavicular fragment during a Mumford procedure.

Depicts the result after distal clavicle excision.
Closure
After achieving stable fixation and repairing the AC ligaments and deltotrapezial fascia, the wound is irrigated. Subcutaneous tissues are closed, and skin is closed with sutures or staples. A sterile dressing is applied.
Illustrates the final appearance of the surgical incision and repaired tissue.
Post-operative view after AC joint reconstruction.
Final clinical appearance after successful reconstruction and healing.
Complications and Management
Despite advancements in surgical techniques, AC joint reconstruction is not without potential complications. A thorough understanding of these issues and their management is crucial for all orthopedic surgeons.
Common Complications and Salvage Strategies
| Complication | Incidence | Etiology | Signs and Symptoms | Management and Salvage Strategies |
|---|---|---|---|---|
| Loss of Reduction/Recurrence of Instability | 5-20% | Inadequate initial fixation, hardware failure (pull-out, breakage), premature return to activity, failure of biological healing. | Persistent deformity, pain with movement, clunking sensation, positive stress radiographs. | Acute: Revision surgery with more robust fixation (e.g., larger graft, different implant). Chronic: Revision CC reconstruction, often with autograft/allograft augmentation and distal clavicle excision if symptomatic arthritis. Hook plate removal followed by CC reconstruction if plate failure. |
| Hardware Failure | 5-15% (e.g., hook plate breakage, suture button pull-through) | Stress shielding, fatigue failure (especially hook plates), osteoporosis, technical error during placement (e.g., undersized tunnels, inadequate knots), non-union of ligament healing. | Pain, grinding, palpable hardware prominence, radiographic evidence of breakage/migration. | Hook Plate: Early removal and consider CC reconstruction if instability persists. Suture Button: Revision with new implants, potentially larger buttons or augmented with graft. Manage associated non-union if present. |
| Infection | <1-5% | Breach in sterile technique, prolonged surgery, compromised patient immunity, hardware contamination. | Redness, swelling, warmth, pain, purulent discharge, fever, elevated inflammatory markers. | Superficial: Oral antibiotics, local wound care. Deep: Surgical debridement, intravenous antibiotics, hardware removal if necessary (after initial healing if possible). Revision surgery once infection is eradicated. |
| Neurovascular Injury | Rare (<1%) | Direct trauma during dissection (supraclavicular nerves, brachial plexus), errant drill placement (subclavian vessels, lung pleura). | Numbness, paresthesias, motor weakness, vascular compromise (pallor, pulselessness), pneumothorax. | Immediate: Exploration and repair of injured structures. Delayed: Symptomatic management, nerve grafting/transfer for severe deficits, vascular repair. |
| Distal Clavicle Osteolysis | 5-10% (can be higher with hook plates) | Stress shielding from rigid fixation (e.g., hook plates), repetitive microtrauma, altered joint mechanics, inflammatory response. | Localized pain over the distal clavicle, especially with cross-body adduction or overhead activity. | Conservative management (NSAIDs, activity modification, steroid injections) for mild cases. Distal clavicle excision (Mumford procedure) for persistent, symptomatic osteolysis. |
| Subacromial Impingement | 5-10% | Prominence of hardware (e.g., hook plate, proud suture button), residual superior migration of clavicle, hypertrophic scar tissue. | Pain with overhead arm elevation, positive impingement signs. | Hook Plate: Scheduled removal. Suture Button: If symptomatic, removal of knot/button. If due to residual deformity: revision reconstruction or acromioplasty. |
| Heterotopic Ossification (HO) | Variable (0-15%) | Soft tissue trauma, hematoma, genetic predisposition. | Decreased range of motion, pain with movement. | Prophylactic NSAIDs or radiation in high-risk patients. Symptomatic management with physical therapy. Surgical excision if severe and functionally limiting, usually after maturation (6-12 months). |
| Post-Traumatic Arthritis | 10-30% (long-term) | Residual AC joint incongruity, chronic instability, cartilage damage at time of injury, altered biomechanics. | Chronic pain, stiffness, crepitus, progressive loss of motion. | Conservative management (NSAIDs, injections, physical therapy). Distal clavicle excision (Mumford procedure) for symptomatic arthritis. Fusion in very rare, extreme cases. |
| Surgical Site Pain/Scar Issues | Common | Incision site neuroma (supraclavicular nerve branches), keloid/hypertrophic scar, chronic incisional pain. | Localized tenderness, dysesthesia, hyperesthesia, itching, cosmetic concern. | Conservative management (nerve blocks, topical agents). Scar massage, silicone sheets. Surgical excision of neuroma or scar revision in recalcitrant cases. |
| Coracoid Fracture | Rare (<1%) | Excessive tensioning of CC reconstruction, errant drill hole placement, pre-existing coracoid pathology. | Acute post-operative pain, loss of fixation, crepitus, sudden loss of reduction. | Non-displaced: Immobilization, protected range of motion. Displaced: Revision surgery with internal fixation of the coracoid (if amenable) and revised CC reconstruction. |
Radiograph demonstrating potential hardware complications or loss of reduction.
Post Operative Rehabilitation Protocols
A structured and progressive post-operative rehabilitation protocol is critical for maximizing outcomes following AC joint reconstruction, facilitating tissue healing, restoring range of motion, and regaining strength and function. The protocol is typically divided into phases, with clear goals and precautions for each.
Phase I: Protection and Early Healing (Weeks 0-6)
Goals:
* Protect the surgical repair and allow initial tissue healing.
* Control pain and inflammation.
* Prevent stiffness in adjacent joints.
Management:
* Immobilization: The arm is typically immobilized in a sling for 4-6 weeks. The type of sling may vary based on surgeon preference and the specific repair. A simple arm sling is often preferred over an aggressive clavicle strap sling (figure-of-eight) in the immediate post-operative phase, as the latter can create tension that may jeopardize the repair.
* Pain Control: Prescribed analgesics, NSAIDs (if not contraindicated for bone healing), cryotherapy.
* Activity Restrictions: No active shoulder elevation, abduction, or external rotation. No lifting, pushing, or pulling with the affected arm. Avoid sleeping on the operative side.
* Gentle Passive Range of Motion (PROM): Initiated early, typically within the first week, for the glenohumeral joint (e.g., pendulum exercises, table slides, supine passive flexion to 90 degrees) and elbow/wrist/hand. Crucially, no aggressive passive motion or stretching of the AC joint itself. Scapular stabilization exercises (e.g., gentle scapular retraction) may be introduced cautiously.
* Wound Care: Maintain a clean, dry surgical incision.
Phase II: Controlled Motion and Gradual Strengthening (Weeks 6-12)
Goals:
* Gradually restore full pain-free passive and active range of motion.
* Initiate gentle strengthening of the shoulder girdle.
* Improve neuromuscular control.
Management:
* Sling Discontinuation: The sling is typically discontinued around 6 weeks, progressing to active-assisted range of motion (AAROM) and then active range of motion (AROM).
* Progressive ROM: Gradually increase shoulder flexion, abduction, and rotation, aiming for full pain-free motion by 10-12 weeks. Emphasis on proper scapulohumeral rhythm.
* Isometrics: Begin with gentle isometric exercises for the rotator cuff and deltoid, with the arm in neutral positions.
* Scapular Stabilization: Progress scapular strengthening exercises (e.g., seated rows, press-ups, prone extension with scapular retraction).
* Light Resistance Training: Introduce very light resistance bands or weights for rotator cuff and deltoid strengthening, always maintaining good form and avoiding pain.
* Precautions: Avoid heavy lifting, sudden jerking movements, or activities that place direct stress on the AC joint. No pushing up from a seated position with the operative arm.
Phase III: Advanced Strengthening and Return to Function (Weeks 12-24)
Goals:
* Restore full strength, endurance, and power.
* Progress to functional and sport-specific activities.
* Achieve dynamic joint stability.
Management:
* Advanced Strengthening: Progress resistance training with increasing weights and repetitions. Incorporate eccentric exercises. Focus on multi-planar movements.
* Proprioceptive Training: Balance and proprioception exercises for the shoulder (e.g., plyoball throws, unstable surface training).
* Core and Kinetic Chain Integration: Emphasize strengthening of the trunk and lower extremities to support overall shoulder function.
* Sport/Activity-Specific Training: Begin drills specific to the patient's sport or occupational demands. Gradually increase intensity and complexity.
* Precautions: Continue to avoid contact sports or activities with high risk of re-injury until full strength and confidence are achieved, typically beyond 6 months.
Phase IV: Return to Sport/Full Activity (Months 6+)
Goals:
* Unrestricted return to desired activities, including contact sports.
* Maintain strength and flexibility.
Management:
* Gradual Return: Patient is cleared for full activity when criteria are met (e.g., full pain-free ROM, symmetrical strength (>90% contralateral limb), no tenderness, surgeon clearance).
* Maintenance Program: Continue a regular exercise program to maintain strength, flexibility, and prevent recurrence.
General Considerations:
* The timeline is approximate and should be individualized based on patient healing, pain levels, and progress.
* Close communication between the surgeon and physical therapist is essential.
* Patient education regarding the importance of adherence to the protocol and avoiding premature return to high-impact activities is paramount to prevent re-injury or complications.
Summary of Key Literature and Guidelines
The management of AC joint injuries has been a subject of extensive research and ongoing debate, particularly concerning Rockwood Type III injuries. A robust body of literature guides current practice.
Management of Rockwood Type III Injuries
The most significant controversy revolves around the optimal treatment for Rockwood Type III AC joint dislocations.
- Non-Operative vs. Operative for Type III: Early studies often favored conservative management due to comparable functional outcomes and lower complication rates compared to older, less robust surgical techniques. However, systematic reviews and meta-analyses, particularly those involving randomized controlled trials, have provided a more nuanced view.
- Some studies suggest no significant long-term difference in functional scores (e.g., Constant score, ASES score) between operative and non-operative groups for Type III injuries in the general population.
- Conversely, some evidence points to better outcomes in terms of endurance, return to pre-injury activity levels, and cosmetic appearance with surgical fixation in high-demand athletes and laborers.
- A prevailing consensus is that for Type III injuries, a trial of conservative management is often appropriate for most patients, with surgical intervention reserved for those who fail to improve, have high functional demands, or desire a more anatomical restoration.
- Chronic Type III Injuries: For patients with chronic symptomatic Type III instability, surgical reconstruction is generally recommended, often involving both CC ligament reconstruction and distal clavicle excision if arthritic changes are present.
Evolution of Surgical Techniques
The literature reflects a clear shift from older, less reliable techniques (e.g., AC pinning, simple CC screws) to more biomechanically sound and anatomically reconstructive procedures.
- Hook Plates: While providing rigid temporary fixation, studies consistently highlight the necessity of a second surgery for hardware removal due to high rates of complications such as subacromial impingement, osteolysis, and plate breakage. Their role is increasingly limited to specific scenarios or as a temporary measure.
- Coracoclavicular Ligament Reconstruction: Anatomic CC reconstruction (ACCR) using suture button devices (e.g., TightRope system) or biological grafts (autograft or allograft) has demonstrated superior biomechanical properties and improved clinical outcomes compared to non-anatomic reconstructions.
- Studies comparing suture button fixation to hook plates often show comparable clinical outcomes with lower reoperation rates (due to avoidance of routine hardware removal) for the suture button group.
- Biological augmentation with tendon grafts is often favored for chronic injuries or revisions, offering a more durable reconstruction, though donor site morbidity (for autografts) and graft incorporation issues are considerations.
Distal Clavicle Excision (Mumford Procedure)
The Mumford procedure, involving resection of the distal clavicle, remains a reliable option for symptomatic distal clavicle osteolysis and post-traumatic AC joint arthritis. It can be performed open or arthroscopically, with comparative studies showing similar efficacy but potentially faster recovery with arthroscopic techniques. It is often combined with CC reconstruction in chronic AC joint instability with associated degenerative changes.
Key Literature and Guidelines
- Rockwood and Matsen's The Shoulder: Remains the definitive textbook, providing extensive detail on classification, diagnosis, and surgical techniques for AC joint injuries.
- AAOS Clinical Practice Guidelines: While often broad, they emphasize evidence-based decision-making. Specific guidelines for AC joint injuries often highlight the controversy of Type III management and the need for individualized patient assessment.
- Randomized Controlled Trials (RCTs) and Meta-Analyses: Recent high-level evidence has clarified many aspects of AC joint management, demonstrating the efficacy of modern reconstructive techniques, especially for higher-grade injuries, and informing the ongoing debate regarding Type III injuries.
- Biomechanics Studies: Extensive research elucidating the role of AC and CC ligaments and the biomechanical characteristics of various fixation constructs continues to drive innovation in surgical techniques.
In conclusion, the management of AC joint injuries requires a comprehensive approach, combining a deep understanding of anatomy and biomechanics with evidence-based clinical decision-making. While conservative management remains paramount for lower-grade injuries, advancements in surgical techniques, particularly anatomic CC reconstruction, offer reliable and reproducible outcomes for complex and higher-grade dislocations, enhancing the potential for effective healing and restoration of function.
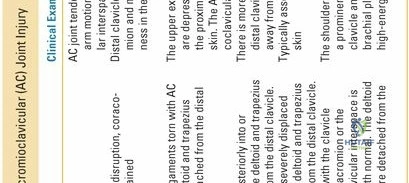
Clinical & Radiographic Imaging

