Unraveling 10 Pediatric Cases: Surgical Reduction and Internal Fixation

Key Takeaway
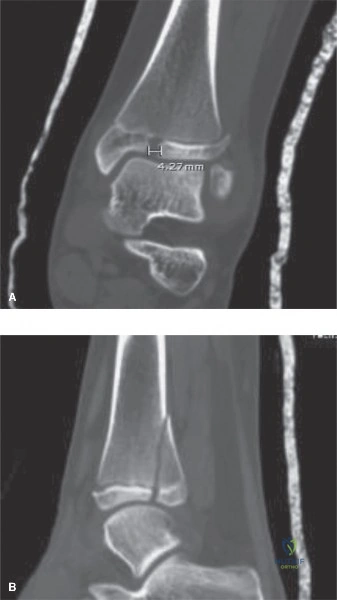
Your ultimate guide to Unraveling 10 Pediatric Cases: Surgical Reduction and Internal Fixation starts here. A Tillaux fracture is an adolescent transitional ankle fracture of the distal tibial epiphysis, where the AITFL attaches, classified as Salter-Harris III because the fracture exits the physis into the epiphysis. For displaced fractures, **surgical reduction and internal** fixation is often required to ensure proper alignment, stability, and growth plate integrity, preventing long-term complications.
You are in the trauma bay. An 8-year-old child presents after a high-speed MVC with a "floating elbow" and a femoral shaft fracture. You see this radiograph of the elbow. Describe your findings and the immediate clinical implications.
Candidate: The radiograph shows a Gartland Type III extension-type supracondylar humerus fracture. I would check the neurovascular status immediately, specifically the Anterior Interosseous Nerve (AIN) and the radial pulse. Given the high-energy nature and the "floating elbow," I am concerned about compartment syndrome.
Failure to mention the "puckering sign" or the specific implications of the pediatric physeal status. Many candidates focus solely on the fracture classification and ignore the "Rule of Twos" or the potential for growth disturbances.
Identify the injury as a Gartland Type III supracondylar humerus fracture. Discuss the clinical "puckering sign" (tethering of the skin) as a surrogate for soft tissue entrapment. Systematically address: 1) Vascular assessment (pink/pulseless vs. perfused), 2) Neurological deficit (specifically AIN palsy), 3) The significance of the "floating elbow" (high energy, increased risk of compartment syndrome), and 4) The treatment goal: anatomical reduction to restore Baumann’s angle to prevent cubitus varus.
Regarding the lateral condyle fracture shown here, what is the critical factor in deciding between operative and non-operative management, and what are the consequences of a wrong decision?

Candidate: The critical factor is the displacement of the fracture. If it is displaced more than 2mm, it requires ORIF. If it is less than 2mm, you can treat it non-operatively with close follow-up.
Ignoring the "cartilaginous hinge." A candidate who doesn't mention the stability of the cartilaginous hinge (as seen on MRI or arthrogram) when the displacement is equivocal is missing the nuance of modern pediatric management.
Structure the answer by Milch classification. Emphasize that >2mm displacement requires ORIF to prevent nonunion, growth arrest, and tardy ulnar nerve palsy. Mention that for stable patterns, we use serial radiographs to ensure the displacement does not increase, as the fragment can be pulled by the common extensor origin.
We are planning fixation for the supracondylar fracture in our index patient. Look at this pin configuration. What are the pros and cons of this approach, and how does it compare to a medial-lateral crossed configuration?
Candidate: This shows lateral-entry K-wires. It is safer because it avoids the ulnar nerve, which is at risk with a medial pin. Crossed pins are structurally more stable but carry a risk of iatrogenic nerve injury.
Failing to mention the geometry of the pin placement. A candidate must note that the lateral pins must be divergent and achieve bicortical purchase in the proximal fragment to provide adequate stability.
Compare the biomechanical stability vs. safety profile. Crossed pins (medial/lateral) provide superior torsional stability. However, lateral-only divergent pinning is standard practice due to the unacceptable risk of ulnar nerve palsy with medial entry. High-scoring candidates will mention the "mini-open" medial approach to visualize the nerve if a medial pin is absolutely required for stability.
