Choosing mm Nonabsorbable Radiolucent for AC Joint Repair

Key Takeaway
For anyone wondering about Choosing mm Nonabsorbable Radiolucent for AC Joint Repair, Acromioclavicular (AC) joint injuries involve damage to the AC and coracoclavicular ligaments, often from direct trauma, causing dislocation and pain. These common shoulder injuries affect crucial static and dynamic stabilizers. Surgical repair and reconstruction may utilize specific materials, such as 1.5 mm nonabsorbable radiolucent sutures or fixation devices, to restore joint stability and function.
Comprehensive Introduction and Patho-Epidemiology
Epidemiology and Mechanism of Injury
Acromioclavicular (AC) joint injuries represent a significant proportion of shoulder girdle trauma, accounting for approximately 9% of all shoulder injuries evaluated in acute care settings. These injuries are predominantly observed in young, active populations, particularly collision athletes such as rugby, football, and hockey players, as well as individuals involved in high-velocity trauma like cycling or equestrian accidents. The classical mechanism of injury involves a direct blow to the lateral aspect of the acromion with the arm in an adducted position. This force vector drives the acromion inferiorly and medially, while the clavicle remains stabilized by the sternoclavicular joint and the strong cervical musculature, resulting in a shearing force across the AC joint.


Indirect mechanisms, though less common, typically occur via a fall onto an outstretched hand (FOOSH) or elbow. In this scenario, the force is transmitted axially up the arm, driving the humeral head superiorly into the acromion and subsequently stressing the AC joint capsule and ligaments. While direct trauma typically results in predictable, sequential failure of the suspensory ligaments, indirect trauma can present with concomitant glenohumeral pathology, such as superior labral anterior-posterior (SLAP) tears or rotator cuff contusions, which must be carefully ruled out during the initial clinical evaluation.
Understanding the epidemiology and mechanism of injury is paramount for the orthopedic surgeon, as it directly informs the index of suspicion for associated injuries. High-energy direct impacts should prompt a thorough evaluation for pneumothorax, rib fractures, and neurovascular compromise, particularly involving the brachial plexus. Furthermore, the chronicity of the injury plays a critical role in surgical decision-making, as acute repairs utilizing millimeter (mm) nonabsorbable radiolucent constructs rely heavily on the healing potential of native tissues, whereas chronic reconstructions often necessitate biological augmentation via allograft or autograft tissue.
Pathogenesis and Sequential Failure Sequence
The pathogenesis of AC joint separation follows a well-documented, sequential continuum of soft tissue failure that correlates directly with the magnitude of the applied force. The initial stage of failure involves the acromioclavicular capsular ligaments. Because these ligaments are the primary restraints to anteroposterior translation, their isolated disruption (Type II injury) allows for horizontal instability while vertical stability is maintained by the intact coracoclavicular (CC) ligaments. The superior and posterior AC capsular ligaments are particularly robust, and their disruption is a prerequisite for subsequent posterior displacement of the clavicle.


As the deforming force continues, the energy is transferred medially to the CC ligament complex. The trapezoid ligament, positioned anterolaterally, and the conoid ligament, positioned posteromedially, fail under extreme tensile loads. The conoid ligament, which possesses the highest in situ forces during superior loading, is often the first of the CC complex to rupture. Complete disruption of both the AC and CC ligaments characterizes a Type III injury, resulting in gross vertical instability and the classic clinical presentation of a "high-riding" clavicle—though biomechanically, it is the scapula that has ptosed inferiorly due to the loss of its clavicular strut and the weight of the upper extremity.
In the most severe manifestations of this trauma (Types IV, V, and VI), the deforming forces exceed the capacity of the ligamentous structures and propagate into the dynamic stabilizers, specifically the deltotrapezial fascia. Disruption of this aponeurotic sleeve allows the distal clavicle to buttonhole through the musculature (Type V) or displace posteriorly into the trapezius muscle belly (Type IV). The recognition of this sequential pathogenesis is critical for modern surgical interventions; anatomical reconstruction must address not only the CC ligaments using mm nonabsorbable radiolucent tapes but also meticulously repair the AC capsule and imbricate the deltotrapezial fascia to restore both static and dynamic stability.


Natural History and Prognostic Indicators
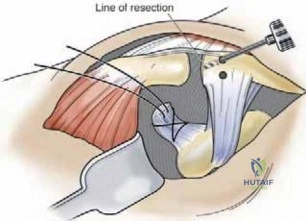
The natural history of AC joint injuries is highly dependent on the initial grade of the separation, the patient's functional demands, and the integrity of the dynamic muscular stabilizers. For low-grade injuries (Types I and II), the natural history is generally favorable. The vast majority of patients achieve full, painless range of motion and return to pre-injury activity levels with conservative management. However, orthopedic surgeons must remain vigilant, as up to 27% of patients with Type I and II injuries may develop persistent symptoms. These sequelae typically manifest as post-traumatic osteolysis of the distal clavicle, late-onset AC joint arthrosis, or chronic localized pain exacerbated by cross-body adduction, occasionally necessitating delayed distal clavicle excision.
The natural history of Type III injuries remains one of the most vigorously debated topics in orthopedic sports medicine. Most current literature, including surveys of elite professional sports physicians, indicates that approximately 80% of athletes with Type III separations treated nonoperatively achieve complete pain relief and functional restoration. Studies have repeatedly failed to demonstrate a statistically significant difference in the timing of return to play or overall functional scoring between operative and nonoperative cohorts at mid-term follow-up. However, subtle deficits, such as a reported 17% decrease in bench press strength and alterations in scapulothoracic kinematics (scapular dyskinesia), may persist, making conservative management less ideal for overhead athletes or heavy manual laborers.


Conversely, the natural history of high-grade injuries (Types IV, V, and VI) is unequivocally poor if left untreated. Patients with neglected high-grade separations universally develop chronic pain, severe scapular dyskinesia, impingement-like symptoms due to altered glenohumeral mechanics, and profound weakness in overhead activities. The persistent displacement of the distal clavicle through the disrupted deltotrapezial fascia prevents spontaneous healing of the ligamentous structures. Consequently, these high-grade injuries mandate operative intervention to restore the anatomical alignment of the shoulder girdle and prevent long-term, debilitating morbidity.
Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Configuration
The acromioclavicular joint is a complex diarthrodial articulation that serves as the sole osseous link between the axial skeleton (via the sternoclavicular joint) and the upper extremity. The articular surfaces of the distal clavicle and the medial acromion are incongruent, varying significantly in their obliquity and orientation. The joint orientation typically slopes medially and inferiorly, which inherently predisposes the clavicle to superior displacement under shear forces. Both articular surfaces are covered by hyaline cartilage, which transitions to fibrocartilage as individuals age, a physiological adaptation to the high compressive and shear loads experienced at this pivot point.


Interposed between these articular surfaces is an intra-articular meniscus-like structure. In the first two decades of life, this fibrocartilaginous disc is typically complete, aiding in load distribution and joint congruency. However, by the fourth decade, it undergoes rapid, physiological degeneration, often becoming a meniscoid remnant. This predictable degeneration explains the high prevalence of asymptomatic AC joint arthrosis seen on routine radiographs in older populations. The entire articulation is enveloped by a joint capsule lined with synovium, which provides proprioceptive feedback and secretes synovial fluid for chondral nutrition.
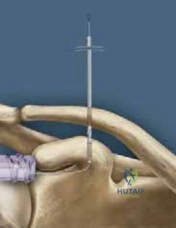
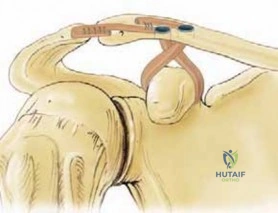
Biomechanically, the AC joint is not a static hinge but a highly dynamic pivot point that accommodates substantial rotational and translational movements. As the arm is elevated, the clavicle must rotate posteriorly up to 40 degrees along its longitudinal axis to allow the scapula to upwardly rotate and protract around the thoracic wall. Furthermore, the joint translates in both the anteroposterior and superoinferior planes. Rigid fixation techniques across the AC joint (such as traditional screw fixation) artificially restrict this obligatory rotation, leading to hardware failure or clavicular fracture. This biomechanical reality underscores the modern preference for suspensory, nonabsorbable radiolucent constructs that permit physiological micromotion while maintaining reduction.
Static Stabilizers: The Ligamentous Complex
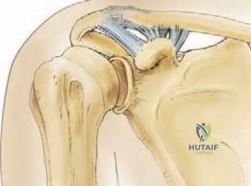
The static stability of the AC joint is governed by two distinct ligamentous complexes: the acromioclavicular (AC) ligaments and the coracoclavicular (CC) ligaments. The AC capsular ligaments are composed of superior, inferior, anterior, and posterior bundles. Biomechanical studies have definitively shown that the AC ligaments are the primary restraints to anteroposterior translation of the distal clavicle. Specifically, the superior and posterior capsular ligaments are the most robust; their integrity is absolutely critical to prevent posterior displacement of the clavicle into the trapezius and abutment against the scapular spine.
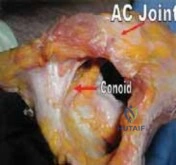
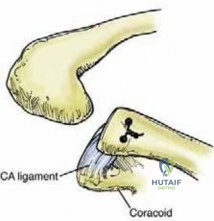
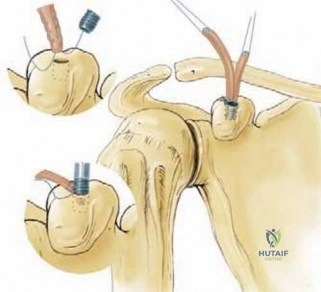
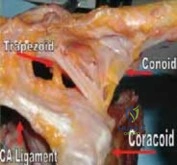
The coracoclavicular (CC) ligament complex, consisting of the conoid and trapezoid ligaments, provides the primary restraint against vertical translation (superior-inferior displacement). The anatomical footprint of these ligaments is of paramount importance when planning anatomical reconstruction. The coracoclavicular space typically spans 1.1 to 1.3 cm. The conoid ligament is a stout, inverted cone-shaped structure that originates from the posteromedial aspect of the coracoid base and inserts onto the conoid tubercle of the clavicle, located approximately 4.5 cm medial to the AC joint. It is the primary restraint against superior and anterior loading.
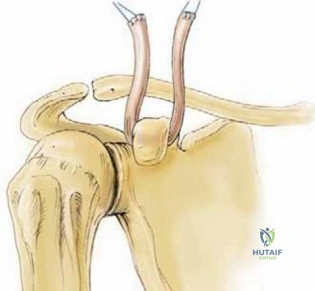
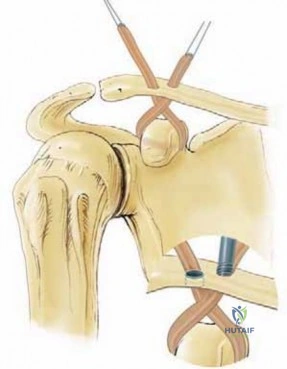
The trapezoid ligament originates anterior and lateral to the conoid on the coracoid process and inserts onto the trapezoid line on the inferior surface of the clavicle, approximately 3.0 cm medial to the distal articular surface. The trapezoid acts as the primary restraint to axial compression, resisting medial displacement of the scapula relative to the clavicle. Both ligaments sit posterior to the pectoralis minor attachment on the coracoid process. When utilizing mm nonabsorbable radiolucent tapes for reconstruction, surgeons must carefully replicate this anatomical divergence—often utilizing two separate clavicular tunnels to recreate the distinct biomechanical vectors of the conoid and trapezoid bundles.

Dynamic Stabilizers and Neurovascular Anatomy
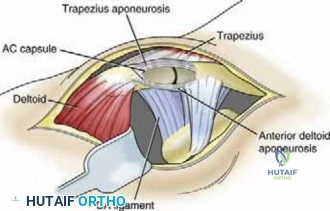
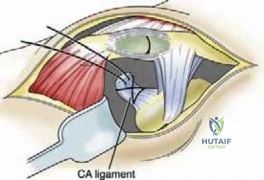
Beyond the static ligamentous restraints, the dynamic stabilizers of the AC joint play an indispensable role in maintaining shoulder girdle integrity. The deltoid and trapezius muscles interdigitate over the superior aspect of the clavicle and acromion to form the deltotrapezial aponeurosis. This strong fascial sleeve acts as a dynamic compressor of the AC joint. In high-grade separations (Types IV-VI), this fascia is invariably torn, stripping away from the distal clavicle. Failure to meticulously repair and imbricate this fascial layer during surgery significantly increases the risk of recurrent instability, regardless of the strength of the underlying nonabsorbable radiolucent fixation.
The neurovascular anatomy surrounding the AC and CC joints demands meticulous respect during surgical exposure and instrumentation. The AC joint itself receives dual innervation from the lateral pectoral nerve and the suprascapular nerve. This dual innervation explains the often diffuse and confusing clinical presentation of AC joint pain, which can radiate anteromedially (mimicking pectoralis or glenohumeral pathology) or posteriorly. Diagnostic local anesthetic injections are highly specific because they directly address this complex terminal innervation.
Surgically, the most critical neurovascular structure at risk during CC ligament reconstruction is the musculocutaneous nerve, which typically enters the conjoined tendon 3 to 5 cm distal to the coracoid tip, though anatomical variants exist where it lies much closer. Furthermore, the suprascapular nerve and artery course through the suprascapular notch, located just medial to the base of the coracoid. When dissecting the posteromedial aspect of the coracoid to pass shuttling relays for nonabsorbable radiolucent tapes, the surgeon must stay strictly subperiosteal and avoid plunging instruments medially, which could result in catastrophic neurovascular injury.
Exhaustive Indications and Contraindications
Clinical Evaluation and Diagnostic Triage
The clinical evaluation of a suspected AC joint injury begins with a detailed history, specifically focusing on the mechanism of injury, hand dominance, occupation, and athletic demands. Patients typically present supporting the injured extremity with their contralateral hand to offload the weight of the arm, which exacerbates pain by stretching the injured CC ligaments. Point tenderness directly over the AC joint is the most sensitive clinical finding. The surgeon must carefully palpate the entire clavicle, the sternoclavicular joint, and the coracoid process to rule out concomitant fractures.


Provocative testing is essential for diagnostic triage. The cross-arm adduction test is performed by elevating the arm to 90 degrees and actively adducting it across the patient's body; pain localized to the AC joint is highly indicative of pathology, whereas posterior pain may suggest posterior capsular tightness or impingement. The Paxinos test, performed by applying anterior pressure to the posterolateral acromion while simultaneously applying posterior pressure to the mid-clavicle, creates a shearing force that elicits pain in the presence of AC joint disruption. The O'Brien active compression test may also be positive, but the surgeon must ensure the pain is localized to the superior AC joint rather than deep within the glenohumeral joint, which would suggest a SLAP lesion.
Because of the overlapping innervation by the lateral pectoral and suprascapular nerves, differentiating AC joint pain from intrinsic glenohumeral or subacromial pathology can be challenging. In ambiguous cases, particularly chronic Type II or low-grade Type III injuries, a targeted intra-articular injection of a local anesthetic (e.g., 1% lidocaine) into the AC joint serves as an excellent diagnostic tool. Complete, albeit temporary, resolution of symptoms confirms the AC joint as the primary pain generator, thereby guiding the decision matrix toward either conservative rehabilitation or surgical intervention.
Operative Rationale Based on Rockwood Classification
The Rockwood classification system remains the gold standard for categorizing AC joint injuries and directly dictates the operative rationale. Type I injuries (sprain of the AC ligaments, intact CC ligaments, normal radiographs) and Type II injuries (ruptured AC ligaments, sprained CC ligaments, horizontal instability but vertical stability) are almost universally managed nonoperatively. Surgery is contraindicated in the acute setting for these grades, though delayed distal clavicle excision may be indicated if post-traumatic arthrosis develops.


Type III injuries (complete disruption of AC and CC ligaments, 25-100% superior translation of the clavicle relative to the acromion) represent a clinical gray area. The operative rationale here is highly individualized. Indications for surgery in Type III injuries include elite overhead athletes, heavy manual laborers who require maximal shoulder torque, patients with severe scapulothoracic dyskinesia, and those who have failed a minimum of 3 to 6 months of comprehensive nonoperative rehabilitation. Relative contraindications include sedentary patients, those with significant medical comorbidities, or poor soft-tissue envelopes.
Types IV, V, and VI are absolute indications for surgical intervention due to the severe disruption of the deltotrapezial fascia and gross instability. Type IV injuries involve posterior displacement of the clavicle into the trapezius muscle, often tenting the posterior skin. Type V injuries are characterized by severe inferior drooping of the scapula, resulting in a CC distance increase of 100% to 300%. Type VI, the rarest form, involves inferior dislocation of the clavicle to a subacromial or subcoracoid position. In these high-grade injuries, nonoperative management is contraindicated as it invariably leads to chronic pain, severe weakness, and degenerative changes of the shoulder girdle.
Decision-Making Matrix for Acromioclavicular Interventions
| Injury Grade (Rockwood) | Ligamentous Status | Fascial Status | Primary Management Strategy | Indications for Operative Intervention |
|---|---|---|---|---|
| Type I | AC sprained, CC intact | Intact | Nonoperative (Sling, NSAIDs, PT) | Failure of prolonged conservative care (late arthrosis) |
| Type II | AC torn, CC sprained | Intact | Nonoperative (Early mobilization) | Chronic horizontal instability; distal clavicle osteolysis |
| Type III | AC torn, CC torn | Intact | Individualized (Usually Nonoperative) | Elite athletes, heavy laborers, chronic symptomatic instability >3 months |
| Type IV | AC torn, CC torn | Disrupted | Operative Reconstruction | Acute or chronic presentation (Posterior displacement) |
| Type V | AC torn, CC torn | Severely Disrupted | Operative Reconstruction | Acute or chronic presentation (>100% vertical displacement) |
| Type VI | AC torn, CC torn | Disrupted | Operative Reconstruction | Acute presentation (Inferior dislocation) |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging and Radiographic Templating
Accurate preoperative planning relies heavily on a comprehensive radiographic evaluation. Standard glenohumeral views are often insufficient due to the superficial location of the AC joint, which leads to over-penetration and loss of bony detail. The standard AC joint series must include an anteroposterior (AP) view, a supraspinatus outlet view, an axillary view, and a Zanca view. The Zanca view is the most critical imaging modality; it is obtained by tilting the x-ray beam 10 to 15 degrees cephalad and utilizing approximately 50% of the standard penetration strength. This specific angulation removes the overlapping shadow of the scapular spine, providing an unobstructed view of the AC articulation and the distal clavicle.

The axillary view is mandatory to evaluate anteroposterior translation and is the definitive radiograph for diagnosing a Type IV posterior dislocation. Furthermore, the surgeon must carefully evaluate the coracoid process. If a patient presents with a clinically obvious AC separation but the coracoclavicular interspace appears normal on the Zanca view, a concomitant coracoid base fracture must be highly suspected. In such cases, a Stryker notch view is obtained to visualize the coracoid base. Advanced imaging, such as MRI, is rarely required for the diagnosis of the AC separation itself but is invaluable when concomitant intra-articular pathology (e.g., SLAP tears, rotator cuff tears) is clinically suspected.
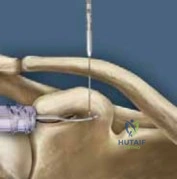
Radiographic templating involves measuring the native coracoclavicular distance on the contralateral, uninjured shoulder (typically 1.1 to 1.3 cm) to establish a reduction goal. The surgeon must also evaluate the width of the clavicle and the morphology of the coracoid to ensure adequate bone stock for drilling. When planning to use mm nonabsorbable radiolucent tapes and cortical buttons, the surgeon must ensure the clavicle is robust enough to accommodate a 4.0 mm or 4.5 mm drill hole without creating a catastrophic stress riser that could lead to an iatrogenic fracture.

Material Selection: The Shift to Nonabsorbable Radiolucent Fixation
Historically, AC joint stabilization relied on rigid metallic implants such as the Bosworth screw or the hook plate. While these provided excellent initial mechanical stability, they were fraught with complications. Rigid fixation across a dynamic joint inherently limits the obligatory 40 degrees of clavicular rotation during arm elevation, leading to hardware breakage, screw pullout, or the necessity for a mandatory secondary surgery for hardware removal. Furthermore, metallic implants cause significant artifact on postoperative imaging, complicating the assessment of reduction and healing.
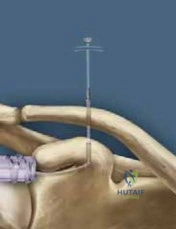
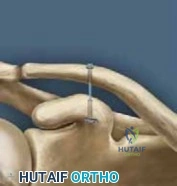
The modern paradigm has shifted decisively toward suspensory fixation utilizing mm-width nonabsorbable radiolucent materials. These constructs typically consist of ultra-high-molecular-weight polyethylene (UHMWPE) tapes or heavy sutures (e.g., #2 or #5 coreless sutures) deployed between metallic or PEEK (polyetheretherket
Clinical & Radiographic Imaging Archive