ORIF of Nonarticular Scapular Fractures: An Intraoperative Masterclass
Key Takeaway
This masterclass details Open Reduction and Internal Fixation (ORIF) of nonarticular scapular fractures, including glenoid neck, acromial, and coracoid processes. We cover comprehensive anatomy, precise patient positioning, and step-by-step intraoperative execution from incision to fixation. Learn critical pearls, pitfalls, and post-operative care, ensuring optimal outcomes for high-energy trauma patients.
Comprehensive Introduction and Patho-Epidemiology
Good morning, colleagues. Welcome to the operating theater. Today, we are undertaking a definitive exploration into a fascinating, structurally complex, and often technically demanding injury: nonarticular scapular fractures. Historically, the vast majority of these injuries—particularly isolated scapular body and spine fractures—were managed nonoperatively. The rationale was rooted in the scapula’s rich vascular envelope, which promotes rapid fracture union, and the extensive compensatory motion of the surrounding shoulder girdle, which can mask minor malunions. However, modern orthopedic traumatology recognizes a significant subset of these fractures that invariably demand surgical intervention to prevent debilitating long-term sequelae.
These injuries are almost exclusively the result of massive, high-energy blunt trauma, such as high-speed motor vehicle collisions, motorcycle accidents, or falls from significant heights. Because the scapula is deeply invested in a thick muscular envelope, it takes an immense transfer of kinetic energy to fracture it. Consequently, the scapula acts as a sentinel injury; we must maintain a hyper-vigilant posture regarding associated, potentially life-threatening trauma. Up to 90% of patients with scapular fractures present with concomitant injuries, including ipsilateral rib fractures, pneumothoraces, pulmonary contusions, brachial plexus traction injuries, and closed head trauma. The orthopedic surgeon must not operate in a vacuum; clearance from general trauma and neurosurgery is a prerequisite before proceeding to the orthopedic theater.
Epidemiologically, scapular fractures are relatively rare, representing approximately 1% of all skeletal fractures and roughly 3% to 5% of all shoulder girdle injuries. Of these, nonarticular fractures—encompassing the glenoid neck, scapular spine, scapular body, acromial process, and coracoid process—account for the overwhelming majority (upwards of 90%). While nonunion of the scapula is an exceedingly rare phenomenon due to the robust blood supply from the subscapular and suprascapular arterial networks, malunion is common in nonoperatively treated displaced fractures.
The modern paradigm shift toward Open Reduction and Internal Fixation (ORIF) in displaced nonarticular fractures is driven by the recognition of the severe morbidity associated with malunion. A severely medially translated or angulated glenoid neck fracture alters the resting tension of the rotator cuff, leading to profound weakness, altered glenohumeral kinematics, secondary impingement syndromes, and debilitating scapulothoracic dyskinesia. Our imperative today is to meticulously restore the three-dimensional structural integrity of the scapula, thereby re-establishing the biomechanical foundation necessary for optimal, pain-free long-term upper extremity function.
Detailed Surgical Anatomy and Biomechanics
Before we make a single incision, an exhaustive, three-dimensional mastery of scapular osteology, muscular intervals, and surrounding neurovascular topography is absolutely paramount. The scapula is a flat, structurally complex, triangular bone that serves as the critical keystone of the shoulder girdle, providing origins and insertions for 17 distinct muscles. It acts as the posterior dynamic anchor connecting the appendicular skeleton of the upper extremity to the axial skeleton. The bone is characterized by a very thin, translucent central body flanked by thick, heavily corticated pillars—specifically the lateral border, the scapular spine, and the base of the coracoid. These thick cortical pillars dictate our surgical fixation strategy, as they are the only regions capable of providing adequate purchase for our screws.
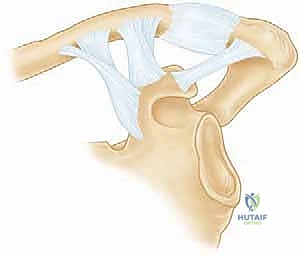
The Superior Shoulder Suspensory Complex (SSSC)
The biomechanical cornerstone of our understanding of these injuries is the Superior Shoulder Suspensory Complex (SSSC), a concept elegantly described by Goss. The SSSC is a vital osteoligamentous ring that effectively suspends the entire upper extremity from the axial skeleton. The ring is composed of the glenoid process, the coracoid process, the coracoclavicular (CC) ligaments, the distal clavicle, the acromioclavicular (AC) joint, and the acromial process.
This ring is supported by two critical struts: the superior strut is the middle third of the clavicle, and the inferior strut is the junction of the lateral scapular body and the medial glenoid neck. A single disruption of this ring (e.g., an isolated, non-displaced clavicle fracture) is generally stable. However, a double disruption—such as a displaced glenoid neck fracture coupled with an ipsilateral clavicle fracture (the classic "floating shoulder")—destabilizes the entire suspensory mechanism. In these scenarios, the weight of the arm and the unopposed pull of the pectoralis major and latissimus dorsi muscles cause the glenohumeral joint to translate inferiorly and medially. Operative stabilization of at least one, and often both, of these disruptions is mandatory to restore the integrity of the SSSC.
Muscular Intervals and Surgical Corridors
Navigating the scapula requires precise exploitation of internervous and intermuscular planes to minimize iatrogenic morbidity. For posterior approaches to the glenoid neck and lateral border, we utilize the classic internervous plane between the infraspinatus muscle (innervated by the suprascapular nerve) and the teres minor muscle (innervated by the axillary nerve). The infraspinatus is a massive, bipennate muscle that must be meticulously elevated from the scapular fossa if medial access is required.
For anterior access to the coracoid process and the anterior glenoid neck, the standard deltopectoral interval is developed. This utilizes the internervous plane between the deltoid (axillary nerve) and the pectoralis major (medial and lateral pectoral nerves). Deep to this, the rotator interval—the space between the subscapularis and supraspinatus tendons—can be opened to access the intra-articular aspect of the glenoid or the base of the coracoid. Understanding these planes ensures we can achieve extensile exposure without denervating the dynamic stabilizers of the shoulder.
Neurovascular Structures at Risk
Vigilance regarding neurovascular anatomy is the hallmark of a master surgeon; the scapula is surrounded by unforgiving structures. The suprascapular nerve is at extreme risk during superior and posterior approaches. It courses through the suprascapular notch (inferior to the superior transverse scapular ligament), provides motor branches to the supraspinatus, and then sharply winds around the base of the scapular spine through the spinoglenoid notch to innervate the infraspinatus. Dissection or hardware placement at the base of the scapular spine or the superior glenoid neck must strictly respect this nerve's trajectory.
The axillary nerve and the posterior circumflex humeral artery exit the axilla posteriorly through the quadrangular space, bounded by the teres minor superiorly, teres major inferiorly, long head of the triceps medially, and the surgical neck of the humerus laterally. During the posterior approach, aggressive distal and lateral retraction of the teres minor can place critical stretch or direct compressive forces on the axillary nerve. Furthermore, when placing plates along the lateral border of the scapula, we must remain aware of the circumflex scapular artery, which wraps around the lateral border and can cause brisk hemorrhage if inadvertently lacerated.
Exhaustive Indications and Contraindications
The decision-making process for operative intervention in nonarticular scapular fractures has evolved significantly. We no longer rely solely on clinical gestalt; we utilize strict radiographic parameters that correlate with poor functional outcomes if left unreduced. The primary goal is to prevent the biomechanical disaster of a medialized, anteverted, or inferiorly tilted glenoid, which fundamentally alters the vector forces of the rotator cuff and deltoid.
The indications for operative management of glenoid neck fractures include translational displacement of the glenoid fragment greater than or equal to 10 to 15 millimeters, or angulation exceeding 40 degrees in either the coronal or sagittal plane. Furthermore, a glenohumeral polar angle (GPA) of less than 22 degrees indicates severe inferior tilt of the glenoid, which drastically increases the risk of inferior glenohumeral instability and warrants fixation. Anatomic neck fractures, which occur lateral to the base of the coracoid, are inherently unstable because they disconnect the glenoid from all ligamentous suspensory attachments, making them absolute indications for surgery.
| Operative Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|
| Glenoid neck translation > 10-15 mm | Hemodynamic instability / severe polytrauma | Advanced age with low functional demand |
| Glenoid neck angulation > 40 degrees | Active infection at the surgical site | Severe osteoporosis compromising fixation |
| Double disruption of the SSSC ("Floating Shoulder") | Pre-existing complete brachial plexus palsy | Heavy smoking history (risk of nonunion) |
| Displaced acromial fracture reducing subacromial space | Severe soft tissue compromise (crush/burns) | Non-compliant patient |
| Displaced coracoid fracture with CC ligament tear | Medical comorbidities precluding anesthesia | Isolated scapular body fracture (minimal displacement) |
Acromial and coracoid process fractures require fixation when their displacement threatens the subacromial space or the integrity of the SSSC. A displaced acromial fracture that tilts inferiorly will inevitably lead to mechanical subacromial impingement and subsequent rotator cuff tearing. Coracoid fractures, particularly those at the base associated with AC joint dislocation or distal clavicle fractures, disrupt the coracoclavicular ligamentous complex and must be rigidly fixed, typically with lag screws, to restore the anterior suspensory strut.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the absolute cornerstone of a successful intraoperative outcome. The complex, undulating three-dimensional anatomy of the scapula makes relying solely on two-dimensional radiographs a fool's errand. While we always obtain a true AP (Grashey view), a true axillary, and a scapular Y view, these are merely screening tools.
A high-resolution CT scan with fine 1mm cuts and 3D surface-rendered reconstructions with the humerus digitally subtracted is mandatory. This allows us to mentally rotate the scapula, map the fracture lines precisely, identify comminution zones, and measure exact angulation and translation. Furthermore, the 3D CT scan is instrumental for preoperative templating. We can use 3D-printed models of the patient's contralateral (uninjured) scapula to pre-contour our 3.5-mm pelvic reconstruction plates or dedicated anatomic scapular plates prior to sterilization. Pre-contouring saves invaluable tourniquet time and prevents the frustration of attempting to bend thick plates in a bloody, restricted surgical field.
Patient Positioning: Lateral Decubitus vs. Beach Chair
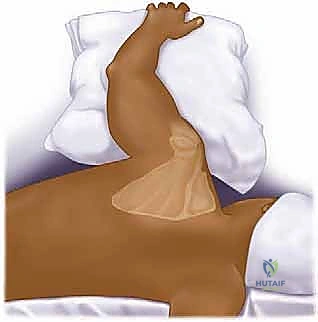
The choice of patient positioning dictates our surgical approach and must be executed flawlessly. For posterior approaches to the glenoid neck and scapular body, the lateral decubitus position is utilized. The patient is placed on their uninjured side, supported by a rigid beanbag. An axillary roll is placed under the dependent thorax to protect the contralateral neurovascular bundle, and all bony prominences (fibular head, greater trochanter) are meticulously padded. The injured upper extremity is prepped and draped completely free. This allows the surgical assistant to apply axial traction, internal/external rotation, and abduction to manipulate the fracture fragments via ligamentotaxis.

The C-arm fluoroscopy unit is brought in from the anterior aspect of the patient, with the monitor positioned at the foot of the bed. The surgeon stands posterior to the patient. It is critical to ensure that true AP and scapular Y views can be obtained without compromising the sterile field before making the incision.
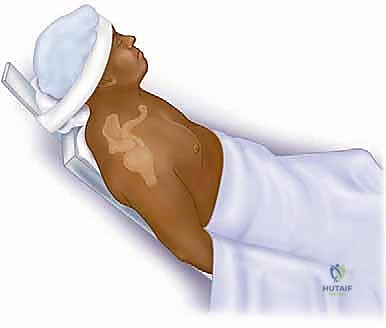
Conversely, if we are addressing an isolated anterior glenoid neck fracture, a coracoid fracture, or performing a combined procedure requiring access to the clavicle and anterior shoulder, the beach chair position is preferred. The patient is elevated to approximately 45-60 degrees, with the head secured in a neutral position to avoid cervical spine hyperextension or lateral flexion, which could stretch the brachial plexus. The arm is draped free and often supported by a pneumatic arm positioner.
Step-by-Step Surgical Approach and Fixation Technique
Let us proceed with the surgical execution. We will detail the classic posterior approach, often referred to as the modified Judet or the Brodsky approach, which offers the most versatile exposure for complex nonarticular scapular neck and body fractures.
The Posterior Approach and Soft Tissue Dissection
We begin by palpating and marking our osseous landmarks: the entire length of the scapular spine, the posterolateral corner of the acromion, and the lateral border of the scapula. The incision is curvilinear, starting at the posterolateral acromion, extending medially along the scapular spine, and curving inferiorly along the lateral border of the scapula.

The crucial first deep step is the mobilization of the deltoid muscle. We incise the deep fascia and meticulously detach the posterior and middle heads of the deltoid from the scapular spine and acromion. This must be done strictly subperiosteally. We leave a robust cuff of periosteum and fascia attached to the bone to facilitate a strong, watertight repair during closure. Failure to securely repair the deltoid origin will result in catastrophic postoperative deltoid dehiscence and profound weakness. The deltoid is then reflected laterally and distally, exposing the underlying rotator cuff musculature.

Next, we identify the internervous plane between the infraspinatus and teres minor. Using blunt dissection with a Cobb elevator or a finger, we separate these muscles. The teres minor is retracted inferiorly, taking immense care not to place excessive traction on the axillary nerve exiting the quadrangular space just inferior to our retractor. The infraspinatus is elevated superiorly and medially from the scapular fossa. We elevate only as much muscle as necessary to expose the fracture lines, preserving the vascular supply to the thin scapular body.

Fracture Reduction and Provisional Stabilization
With the fracture exposed, we thoroughly debride the fracture hematoma and any interposed soft tissue or periosteum using a pituitary rongeur and curettes. Reduction of the glenoid neck is often challenging due to the powerful deforming forces of the surrounding musculature. We frequently utilize 5.0mm Schanz pins placed percutaneously into the glenoid fragment and the lateral border of the scapula to act as "joysticks."
By applying lateral and superior traction on the glenoid Schanz pin while manipulating the arm, we can disimpact the fracture. Dental picks and Weber clamps are used to fine-tune the reduction of the cortical edges. Once anatomic reduction is achieved, it is provisionally stabilized with multiple 2.0mm or 2.4mm Kirschner wires (K-wires). We immediately verify our reduction under multi-planar fluoroscopy, ensuring restoration of the glenohumeral polar angle and correction of any medial translation.
Definitive Plate Fixation
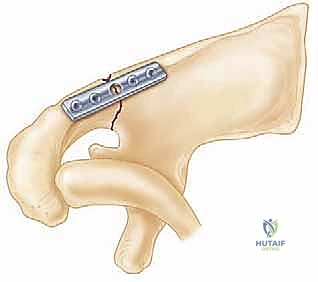
Definitive fixation relies on the biomechanical principle of restoring the lateral pillar of the scapula. We typically utilize pre-contoured 3.5mm extra-articular pelvic reconstruction plates or modern, anatomically specific locking scapula plates. The primary plate is applied strictly along the thick lateral border of the scapula.

Screw trajectory is critical. When placing screws into the superior fragment (the glenoid), they must be directed parallel to the articular surface to avoid intra-articular penetration. We frequently use fluoroscopy to confirm that our drill bit does not breach the subchondral bone of the glenoid fossa. Screws placed into the inferior fragment (the lateral border) must be directed directly down the dense cortical pillar. The central body of the scapula is paper-thin and will not hold screws; attempting to place standard screws here is futile and risks plunging into the thoracic cavity.

If the fracture pattern is highly comminuted or involves a medial extension that remains unstable, a second, orthogonal plate may be applied along the scapular spine. When plating the scapular spine, extreme caution must be exercised at the spinoglenoid notch to avoid entrapment or laceration of the suprascapular nerve.
Following rigid fixation, the wound is copiously irrigated. The deltoid origin is meticulously repaired using heavy, non-absorbable sutures passed through transosseous drill holes in the scapular spine and acromion. This is arguably the most critical step of the closure. The superficial fascia and skin are closed in layers over a closed suction drain to prevent postoperative hematoma formation.
Anterior Approach for Coracoid Fractures
For displaced coracoid fractures, an anterior approach is utilized. A standard deltopectoral incision is made, and the cephalic vein is retracted laterally with the deltoid. The clavipectoral fascia is incised, exposing the conjoint tendon and the fractured base of the coracoid.
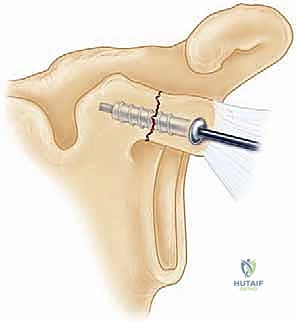
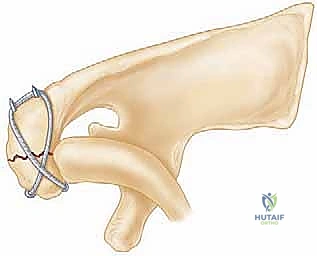
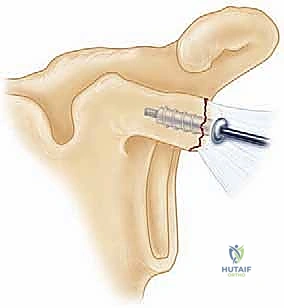
The musculocutaneous nerve, entering the conjoint tendon distally, must be protected. The fracture is reduced anatomically using a pointed reduction clamp. Fixation is typically achieved using one or two 3.5mm or 4.0mm partially threaded cannulated lag screws directed from anterior to posterior into the base of the coracoid and the superior glenoid neck. Washers are frequently used to prevent the screw heads from sinking into the relatively osteopenic bone of the coracoid tip.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, ORIF of scapular fractures carries a distinct complication profile due to the high-energy nature of the injury and the complex regional anatomy. The surgeon must be prepared to identify and manage these complications promptly.
The most dreaded intraoperative complication is iatrogenic nerve injury. Suprascapular nerve palsy can occur due to aggressive medial retraction, direct drill penetration at the spinoglenoid notch, or entrapment beneath a plate. Axillary nerve injury is typically the result of overzealous inferior retraction of the teres minor during the posterior approach. Most nerve injuries are traction neuropraxias that resolve with time, but documented transections require microsurgical nerve grafting or subsequent tendon transfers (e.g., lower trapezius transfer for massive external rotation loss).
| Complication | Estimated Incidence | Prevention and Salvage Management |
|---|---|---|
| Iatrogenic Nerve Palsy (Suprascapular/Axillary) | 3% - 8% | Prevention: Respect safe zones; avoid aggressive retraction. Management: EMG at 6 weeks; if no recovery by 3-6 months, consider nerve exploration/grafting or tendon transfers. |
| Hardware Failure / Loss of Fixation | 2% - 5% | Prevention: Utilize locking plates in osteopenic bone; ensure screws purchase the thick lateral border/spine, not the thin body. Management: Revision ORIF with bone grafting. |
| Postoperative Infection | 1% - 4% | Prevention: Meticulous soft tissue handling; prophylactic antibiotics. Management: Aggressive I&D, hardware retention if stable, culture-directed IV antibiotics. |
| Post-Traumatic Shoulder Stiffness | 15% - 30% | Prevention: Rigid fixation allowing early passive ROM; meticulous capsular repair. Management: Aggressive physical therapy; arthroscopic capsular release if refractory at 6+ months. |
| Symptomatic Malunion | Rare with ORIF | Prevention: Anatomic reduction verified by intraoperative 3D fluoroscopy. Management: Corrective osteotomy (technically demanding, high complication rate). |
Hardware prominence is another frequent complaint, particularly over the scapular spine, given the thin subcutaneous tissue in this region. If the hardware becomes painful after radiographic union is achieved (typically after 9 to 12 months), elective hardware removal may be offered. Infection is relatively rare due to the robust vascularity of the posterior shoulder envelope, but deep infections require aggressive surgical debridement and prolonged culture-directed antibiotic therapy.
Phased Post-Operative Rehabilitation Protocols
The ultimate success of scapular fracture ORIF relies heavily on a structured, phased, and highly supervised postoperative rehabilitation protocol. The mechanical rigidity of our internal fixation must be perfectly balanced against the biologic healing requirements of the extensive soft tissue dissection, particularly the deltoid origin repair.
Phase I: Maximal Protection (Weeks 0 to 2)
Immediately postoperatively, the patient is placed in a supportive clinical sling. The primary goals are wound healing, pain control, and prevention of distal extremity edema. Patients are instructed to perform active range of motion (ROM) of the elbow, wrist, and hand. Pendulum exercises are initiated on postoperative day one. Absolute restrictions during this phase include no active shoulder motion, no lifting, and no sudden movements that could stress the deltoid repair.
Phase II: Controlled Passive and Active-Assisted Motion (Weeks 2 to 6)
At the two-week mark, assuming wound healing is satisfactory, formal physical therapy commences. The sling is gradually weaned for activities of daily living but worn in public and during sleep. We initiate gentle passive range of motion (PROM) and active-assisted range of motion (AAROM) in the supine position to eliminate gravity. Forward elevation is progressively increased, but active extension and active abduction are strictly prohibited, as these motions cause isometric contraction of the posterior and middle deltoid, jeopardizing our transosseous repair.
Phase III: Active Motion and Early Strengthening (Weeks 6 to 12)
Radiographs are obtained at 6 weeks to confirm early callus formation and hardware stability. Once confirmed, the sling is discontinued entirely. The patient progresses to full active range of motion (AROM) in all planes. Gentle isometric strengthening begins, focusing on the rotator cuff and periscapular stabilizers (rh
