Pediatric Orthopaedic Case Study: Late-Presenting Infant DDH - Clinical & Diagnostic Insights
Key Takeaway
Late-presenting Developmental Dysplasia of the Hip (DDH) in infants often presents with a new limp, gluteal fold asymmetry, and a positive Galeazzi sign. A critical finding is marked restriction of passive hip abduction. Barlow and Ortolani maneuvers are typically negative, emphasizing thorough clinical examination and imaging for accurate diagnosis.
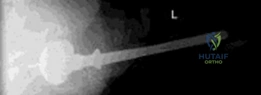
You are presented with this 8-month-old female in the clinic. She was delivered full-term, vaginally. The parents report a limp since she started cruising. A newborn check was reported as normal. Based on the radiographic findings below, describe your findings and formulate a management plan.
Candidate: The radiograph shows a right-sided hip dislocation. The ossific nucleus is absent on the right, Shenton's line is broken, and the metaphysis is in the superolateral quadrant (Tonnis Grade IV). Given the child is 8 months old, a Pavlik harness is unlikely to work. I would perform an examination under anesthesia (EUA), arthrogram, and likely an open reduction, as the soft tissue contractures (specifically the adductor and psoas) will likely prevent closed reduction.
Candidates often suggest "trying" a Pavlik harness or closed reduction without first addressing the high likelihood of failure at 8 months. They may also forget to mention the essential intraoperative steps like the arthrogram or the specific anatomical obstacles (pulvinar, transverse acetabular ligament, limbus) that necessitate open reduction.
The candidate systematically identifies the Tonnis Grade IV dislocation, the absent ossific nucleus, and the elevated acetabular index. They justify the move to open reduction by highlighting the failure of non-operative measures in this age group due to established soft tissue pathology (e.g., adductor/iliopsoas contractures). They explicitly state: "My plan is an EUA, adductor tenotomy, and arthrography. If the medial dye pool is >5mm, I would proceed to an anterior open reduction to remove the pulvinar and excise the ligamentum teres, followed by a capsulorrhaphy and spica cast in the 'human position'."
During the anterior open reduction, you have released the iliopsoas and the adductor longus, but the femoral head remains reluctant to reduce into the acetabulum. What are the potential intra-articular obstacles you must address?
Candidate: The obstacles include the hypertrophied ligamentum teres, the redundant fibrofatty tissue in the acetabulum (the pulvinar), the inverted limbus (labrum), and a tight transverse acetabular ligament.
Failing to mention the labrum or the transverse acetabular ligament. Suggesting excision of the labrum is a major error; it must be everted, not excised, to ensure future acetabular growth.
Structure the answer by "Soft Tissue" and "Bony/Ligamentous" barriers. Identify the pulvinar (fibrofatty tissue), the hypertrophied ligamentum teres, and the transverse acetabular ligament (which requires radial incision). Crucially, emphasize that the labrum (limbus) must be everted to facilitate a concentric reduction without damaging the potential for acetabular modeling.
You have achieved a stable, concentric reduction. How do you assess the "Safe Zone" post-reduction, and why is this critical in preventing long-term complications?
Candidate: The Ramsey safe zone is the range of hip abduction where the hip remains stable without being at risk of dislocation. It is critical because excessive abduction can lead to avascular necrosis (AVN) of the femoral head by compressing the medial circumflex femoral artery against the acetabular rim.
Neglecting to mention the vascular risk. The "Safe Zone" is not just about stability; it is about balancing stability against the risk of iatrogenic osteonecrosis.
Define the Safe Zone as the arc between the point of redislocation (in adduction) and the point of maximum safe abduction. Explain that to avoid AVN, we aim for a "middle ground" of positioning. If the hip requires extreme abduction (>60°) to stay stable, it indicates that the reduction is not truly stable or that soft tissue interposition remains, necessitating further surgical release (like an adductor tenotomy) rather than forced, extreme positioning in a cast.
