AAOS Pediatric Orthopedics (Set 1): DDH, Scoliosis & Growth Plate Injuries | 2024 Board Review
Key Takeaway
This high-yield Set 1 question bank for AAOS and ABOS exams thoroughly covers core pediatric orthopedic topics. Questions address Developmental Dysplasia of the Hip (DDH) diagnosis and treatment, scoliosis management, and Salter-Harris growth plate injuries, crucial for OITE and board review.
AAOS Pediatric Orthopedics (Set 1): DDH, Scoliosis & Growth Plate Injuries | 2024 Board Review
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The inheritance of the deformity shown in Figure 1 is most commonly
Explanation
Question 2
Examination of a 12-year-old girl with bilateral anterior knee pain reveals excessive femoral anteversion and excessive external tibial torsion. The patient has no patellofemoral instability. Nonsurgical management consisting of muscle strengthening and nonsteroidal medication has failed to relieve the patient's pain. Treatment should now consist of
Explanation
Question 3
Which of the following patients with cerebral palsy is considered the ideal candidate for a selective dorsal rhizotomy?
Explanation
Question 4
A 3-year-old boy sustains a complete paralysis following a high thoracic spinal cord injury consistent with a SCIWORA-type injury (spinal cord injury without radiographic abnormality). Subsequent progressive spinal deformity will develop in what percent of patients with this injury?
Explanation
Question 5
A 12-year-old girl has progressive development of cavus feet. Examination reveals slightly diminished vibratory sensation on the bottom of the foot. Reflexes are 1+ at the knees and ankles. Motor examination shows that all muscles are 5/5 in the foot, except the peroneal and anterior tibial muscles are rated as 4+/5. Which of the following studies is considered most diagnostic?
Explanation
Question 6
A 2-year-old girl was born with the toe deformity shown in Figure 2. She has difficulty wearing shoes despite having adequate room in the toe box. Management at this time should consist of
Explanation
Question 7
Figure 3 shows the radiograph of an asymptomatic 10-year-old boy. Management should consist of
Explanation
Question 8
A 12-year-old girl has had lower back pain for the past 6 months that interferes with her ability to participate in sports. She denies any history of radicular symptoms, sensory changes, or bowel or bladder dysfunction. Examination reveals a shuffling gait, restriction of forward bending, and tight hamstrings. Radiographs show a grade III spondylolisthesis of L5 on S1, with a slip angle of 20 degrees. Management should consist of
Explanation
Question 9
Figures 4a through 4c show the clinical photographs and radiographs of a 12-month-old boy who has progressive difficulty wearing shoes because of the length of the second toe, as well as width of the forefoot. Management should consist of
Explanation
Question 10
Figures 5a and 5b show the radiographs of an 11-year-old boy who felt a pop and immediate pain in his right knee as he was driving off his right leg to jam a basketball. Examination reveals that the knee is flexed, and the patient is unable to actively extend it or bear weight on that side. There is also a large effusion. Management should include
Explanation
Question 11
A 2-year-old child has been referred for management of congenital kyphosis. Neurologic examination is normal, and radiographs show a type I congenital kyphosis. Which of the following anomalies is seen in the MRI scan shown in Figure 6?
Explanation
Question 12
A 15-year-old boy with a type I hereditary sensory motor neuropathy (Charcot-Marie-Tooth disease) reports recurrent ankle sprains and significant pain in the hindfoot and midfoot despite orthotic management. Examination reveals that he walks with a drop foot and has dynamic clawing of the toes. Clinical photographs of the left foot are shown in Figure 7. Management should consist of
Explanation
Question 13
Figures 8a through 8d show the radiographs and CT scans of a 14-year-old girl who has a painful, rigid planovalgus foot. Management consisting of arch supports and anti-inflammatory drugs failed to provide relief. A below-knee walking cast resulted in pain resolution, but she now reports that the pain has recurred. Management should now consist of
Explanation
Question 14
Figures 9a and 9b show the spinal radiographs of a 3-year-old child with short limb dwarfism. The lateral radiograph is obtained with maximal lumbar extension. Management should consist of
Explanation
Question 15
A 10-year-old boy with severe hemophilia A (factor VIII) sustained an injury to his right forearm 2 hours ago when a classmate fell on his arm during a scuffle. Examination reveals moderate swelling in the forearm, decreased sensation in the distribution of the median and ulnar nerves, and pain on passive extension of the fingers. What is the most appropriate sequence of treatment?
Explanation
Question 16
Figures 10a and 10b show the radiographs of an athletic 9-year-old boy who has activity-related anterior knee pain with intact active knee extension. Examination reveals tenderness to palpation over the inferior pole of the patella. There is no effusion or ligamentous instability. Initial management should consist of
Explanation
Question 17
A 2-week-old infant has been referred for evaluation of nonmovement of the left hip. History reveals that the patient was delivered 6 weeks premature by cesarean section. Examination reveals no fever, and there is mild swelling of the thigh. Passive movement of the hip appears to elicit tenderness and very limited hip motion. A radiograph of the pelvis shows mild subluxation of the left hip. The next step in evaluation should consist of
Explanation
Question 18
Figure 11 shows the lateral radiograph of a 16-year-old boy who has been unable to participate in sports activities because of pain in the anterior aspect of the knee. He states that the pain is aching in nature and is located in the region of the tibial tuberosity. He denies having joint effusion or symptoms of instability. Management should consist of
Explanation
Question 19
A 10-lb, 2-oz infant who was born via a difficult breech delivery 12 hours ago is now being evaluated for hip pain. Although the infant is resting comfortably, examination reveals that the patient is not moving the right lower extremity and manipulation of the right hip causes the infant to cry. The Galeazzi sign is positive. An AP radiograph of the pelvis shows proximal and superior migration of the right proximal femoral metaphysis. What is the most likely diagnosis?
Explanation
Question 20
A 10-year-old girl has been referred for evaluation of a prominence at the lower cervical spine. The patient is asymptomatic, and the examination reveals no evidence of neurologic abnormality. A radiograph and CT scans are shown in Figures 12a through 12c. What is the most likely diagnosis?
Explanation
Question 21
Which of the following types of iliac osteotomy provides the greatest potential for increased coverage?
Explanation
Question 22
The mother of a 26-month-old boy reports that he has been unwilling to bear weight on his left lower extremity since he awoke this morning. She denies any history of trauma. He has a temperature of 99.4 degrees F (37.4 degrees C), and examination reveals that abduction of the left hip is limited to 30 degrees. Laboratory studies show a WBC of 11,000/mm3 and an erythrocyte sedimentation rate of 22 mm/h. A radiograph of the pelvis is shown in Figure 13. Management should consist of
Explanation
Question 23
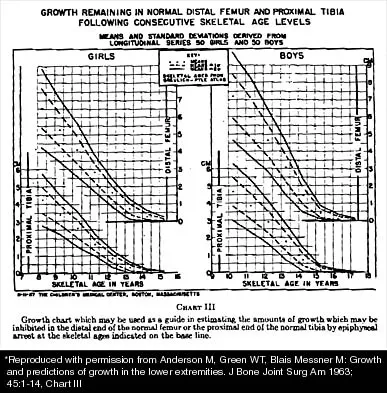
A 10-year-old girl with a monoarticular pattern of juvenile rheumatoid arthritis (JRA) has had a 3-cm limb-length discrepancy since age 8 years when inflammation in the right knee came under good medical control. Because her right leg is longer, the patient states that she would like her legs to be close to equal in length in the future. A growth-remaining chart is shown in Figure 14. Management should consist of
Explanation
Question 24
A 14-year-old girl with polyarticular juvenile rheumatoid arthritis (JRA) has severe neck pain and reports the onset of urinary incontinence. A lateral radiograph and lateral tomogram of the cervical spine are shown in Figures 15a and 15b. An MRI scan of the upper cervical spine is shown in Figure 15c. Management should consist of
Explanation
Question 25
Figures 16a and 16b show the radiographs of an otherwise healthy 3 1/2-year-old boy who has an isolated deformity of the left leg. Definitive primary treatment of this condition should consist of
Explanation
Question 26
A 3-month-old female with developmental dysplasia of the hip (DDH) is being treated with a Pavlik harness. During a follow-up visit, the mother notes the child is no longer kicking her left leg. Examination reveals absent active knee extension on the left. What is the most appropriate next step in management?
Explanation
Question 27
A 6-week-old female infant undergoes a screening hip ultrasound. The alpha angle is 45 degrees and the beta angle is 80 degrees, indicating a laterally displaced cartilage roof. What is the most appropriate next step in management?
Explanation
Question 28
A 13-year-old boy sustains an ankle injury resulting in a juvenile Tillaux fracture. Which of the following describes the normal sequence of closure of the distal tibial physis, predisposing the patient to this specific fracture pattern?
Explanation
Question 29
A 12-year-old girl presents with a painless scoliotic deformity. Radiographs reveal a 35-degree left-sided thoracic curve. Neurologic examination is unremarkable. What is the most appropriate next step in evaluation?
Explanation
Question 30
Which of the following congenital spinal anomalies carries the highest risk of scoliotic curve progression and typically requires early surgical intervention?
Explanation
Question 31
A 6-week-old female is treated with a Pavlik harness for developmental dysplasia of the hip. At the 2-week follow-up, the mother notes the child is no longer kicking her leg on the affected side. On examination, there is decreased active knee extension. What is the most appropriate next step in management?
Explanation
Question 32
Which of the following ultrasound findings is most consistent with a normal infant hip at 6 weeks of age?
Explanation
Question 33
A 13-year-old girl with adolescent idiopathic scoliosis presents for evaluation. Radiographs reveal a right thoracic curve of 35 degrees. Her Risser sign is 1, and she is premenarcheal. What is the most appropriate management?
Explanation
Question 34
A 14-year-old boy sustains a Salter-Harris type III fracture of the medial malleolus. The horizontal component of the fracture typically propagates through which of the following anatomic zones of the physis?
Explanation
Question 35
An 18-month-old child presents with untreated developmental dysplasia of the right hip. Closed reduction is attempted but is unsuccessful due to soft tissue interposition. Which of the following structures is most commonly a block to closed reduction in this setting?
Explanation
Question 36
In the evaluation of infantile idiopathic scoliosis, which of the following radiographic parameters is the most reliable predictor of curve progression?
Explanation
Question 37
A 6-year-old girl is diagnosed with congenital scoliosis due to a fully segmented unilateral hemivertebra at T8. Which of the following imaging studies is most critical to obtain during her initial workup?
Explanation
Question 38
A 15-year-old boy undergoes posterior spinal fusion for adolescent idiopathic scoliosis. During deformity correction, somatosensory evoked potentials (SSEPs) are lost in the bilateral lower extremities, while motor evoked potentials (MEPs) remain intact. What is the most likely cause?
Explanation
Question 39
A 14-year-old girl presents with an acute distal tibial fracture. Radiographs show a Salter-Harris type III fracture of the anterolateral distal tibial epiphysis. What is the mechanism of injury and the deforming force?
Explanation
Question 40
A 5-year-old boy presents with a 40-degree left thoracic scoliosis. MRI reveals a syrinx extending from T4 to T10. Which of the following curve characteristics most strongly suggested the presence of an underlying neural axis abnormality?
Explanation
Question 41
Which pelvic osteotomy for DDH provides primarily anterior and lateral coverage by hinging on the pubic symphysis without changing the shape of the acetabulum?
Explanation
Question 42
A 12-year-old boy presents with a triplane fracture of the distal tibia. Which of the following best describes the typical fracture planes on radiographs?
Explanation
Question 43
A 9-year-old boy is found to have a physeal bar across the central 30% of his distal femoral physis following a previous Salter-Harris type II fracture. He has a 2 cm leg length discrepancy and 4 years of remaining growth. What is the most appropriate surgical management?
Explanation
Question 44
In a child with Duchenne muscular dystrophy, what is the most common indication for spinal fusion surgery for scoliosis?
Explanation
Question 45
An 8-year-old girl with Neurofibromatosis Type 1 presents with a sharp, short-segment thoracic scoliosis of 45 degrees. Radiographs show rib penciling and vertebral scalloping. What is the recommended treatment?
Explanation
Question 46
A newborn is examined in the nursery. The examiner places the infant's hips in 90 degrees of flexion and gently abducts them while applying an anteriorly directed force on the greater trochanter, resulting in a palpable "clunk." What is this provocative test called?
Explanation
Question 47
A 2-year-old boy presents with developmental dysplasia of the hip. A Pemberton osteotomy is planned. What is the primary hinge point for this osteotomy?
Explanation
Question 48
A 14-year-old girl with adolescent idiopathic scoliosis has a major thoracic curve of 55 degrees. On the lateral radiograph, her thoracic kyphosis is measured at +15 degrees. According to the Lenke classification, what is her sagittal modifier?
Explanation
Question 49
A 10-year-old boy sustains a Salter-Harris II fracture of the distal femur. What is the most common significant complication associated with this specific injury?
Explanation
Question 50
The "safe zone" of Ramsey in the treatment of DDH with a spica cast is defined as the position between:
Explanation
Question 51
A 6-week-old female infant, born in breech presentation, undergoes a screening hip ultrasound. The alpha angle is measured at 45 degrees, and the beta angle is 80 degrees. What is the most appropriate next step in management?
Explanation
Question 52
A 3-month-old infant is being treated with a Pavlik harness for developmental dysplasia of the hip. The parents report that the child has stopped kicking the affected leg. On examination, there is decreased active knee extension. Which of the following harness adjustments is required?
Explanation
Question 53
An 18-month-old girl presents with a painless limp and a positive Trendelenburg sign on the right. Radiographs reveal a dislocated right hip with a false acetabulum and breaking of Shenton's line.
What is the most appropriate definitive management?

Explanation
Question 54
Following closed reduction of a dysplastic hip in a 9-month-old, the surgeon applies a spica cast. To minimize the risk of avascular necrosis of the femoral head, the hip should NOT be placed in which of the following positions?
Explanation
Question 55
A 12-year-old girl presents with adolescent idiopathic scoliosis. She has a 20-degree right thoracic curve. She has not reached menarche. Which of the following radiographic parameters indicates the highest risk for curve progression?
Explanation
Question 56
A 13-year-old girl is evaluated for scoliosis. Radiographs show a 32-degree right thoracic curve. She is premenarchal, and her Risser grade is 1.
What is the most appropriate management?

Explanation
Question 57
A 6-month-old infant is diagnosed with infantile idiopathic scoliosis with a 25-degree left thoracic curve. The rib-vertebral angle difference (RVAD) of Mehta is measured at 25 degrees. What is the expected natural history of this condition?
Explanation
Question 58
Which of the following congenital spinal anomalies has the highest rate of progression and warrants early prophylactic in situ fusion?
Explanation
Question 59
A 4-week-old infant is treated with a Pavlik harness for a dislocated left hip. After 3 weeks of strict compliance, ultrasound reveals the hip remains completely dislocated. What is the most appropriate next step in management?
Explanation
Question 60
In the Lenke classification system for Adolescent Idiopathic Scoliosis, a proximal thoracic curve is defined as structural if the residual Cobb angle on a side-bending radiograph is at least:
Explanation
Question 61
A 12-year-old boy sustains a completely displaced Salter-Harris type II fracture of the distal femur. Which of the following factors is most strongly predictive of subsequent premature physeal closure?
Explanation
Question 62
On an anteroposterior pelvis radiograph of a 6-month-old female, the ossific nucleus of the right femoral head is located in the superolateral quadrant formed by Hilgenreiner's and Perkin's lines. What is the diagnosis?
Explanation
Question 63
You are evaluating a 14-month-old boy with infantile idiopathic scoliosis. Which of the following radiographic parameters most reliably predicts the likelihood of curve progression?
Explanation
Question 64
A 9-year-old girl develops a localized physeal bar in the distal radius following a previous trauma. Advanced imaging shows the bar comprises 25% of the cross-sectional area of the physis, and she has roughly 3 cm of anticipated growth remaining. What is the most appropriate management?
Explanation
Question 65
A newborn with arthrogryposis multiplex congenita presents with rigid, bilateral dislocated hips. What is the generally recommended initial management for these hip dislocations?
Explanation
Question 66
A 3-year-old girl is diagnosed with congenital scoliosis secondary to a fully segmented hemivertebra in the lower thoracic spine. Which of the following diagnostic screening studies is most critical during her initial systemic evaluation?
Explanation
Question 67
A 13-year-old boy sustains a juvenile Tillaux fracture. This fracture pattern is primarily the result of the specific sequence of closure of the distal tibial physis. In what predictable sequence does the distal tibial physis normally close?
Explanation
Question 68
A 4-year-old girl is undergoing surgical treatment for late-presenting developmental dysplasia of the hip. The surgeon plans a redirectional pelvic osteotomy that hinges at the symphysis pubis to provide primarily anterolateral coverage. Which osteotomy is being described?
Explanation
Question 69
A 12-year-old premenarchal girl (Risser 0) is diagnosed with Adolescent Idiopathic Scoliosis. Her standing radiographs reveal a right thoracic curve of 32 degrees. Neurologic exam is normal. What is the most appropriate management?
Explanation
Question 70
A 14-year-old boy sustains a triplane fracture of the distal ankle. Which of the following Salter-Harris fracture patterns best describes the radiographic appearance in the sagittal and coronal planes, respectively?
Explanation
Question 71
You are evaluating a 6-week-old infant who has been in a Pavlik harness for 2 weeks for DDH. The parents report the infant has stopped kicking the left leg. On examination, the infant demonstrates absent active knee extension on the left side. What is the most likely diagnosis and appropriate initial management?
Explanation
Question 72
A 6-week-old female infant, born breech, undergoes a screening ultrasound of the hips. The alpha angle is measured at 48 degrees and the beta angle at 65 degrees. Dynamic stress views show subluxation. What is the most appropriate initial management?
Explanation
Question 73
A 6-year-old boy presents with a 35-degree right thoracic curve. An MRI of the entire spine is unremarkable. Which of the following is the most appropriate management for this patient?
Explanation
Question 74
A 13-year-old boy presents with an ankle injury after a twisting mechanism while playing soccer. CT imaging reveals a fracture with a sagittal component through the epiphysis, a coronal component through the posterior metaphysis, and a transverse component through the physis. Which mechanism of injury is most classically associated with this fracture pattern?
Explanation
Question 75
A 30-month-old girl presents with a painless limp. Examination reveals a positive Galeazzi sign and limited abduction of the left hip. Radiographs demonstrate a high dislocation of the left hip with a false acetabulum. She has had no prior treatment. What is the most appropriate definitive management?
Explanation
Question 76
Parents of a newborn diagnosed with congenital scoliosis are seeking counseling regarding the risk of curve progression. Which of the following vertebral anomalies carries the highest risk of rapid progression?
Explanation
Question 77
A 14-year-old girl sustains a juvenile Tillaux fracture (Salter-Harris III of the anterolateral distal tibial epiphysis). What underlying anatomic phenomenon explains why the fracture occurs specifically in this anterolateral location?
Explanation
Question 78
A 14-year-old girl is diagnosed with a 45-degree right thoracic scoliosis. She is premenarcheal, Risser 0, and has open triradiate cartilages on pelvic radiographs. Without treatment, what is the estimated risk of her curve progressing to greater than 50 degrees?
Explanation
Question 79
A 3-month-old infant is being treated for DDH with a Pavlik harness. During a follow-up visit, you notice the infant lacks active knee extension on the treated side, though the harness is holding the hips in 110 degrees of flexion. What is the most likely cause of this finding?
Explanation
Question 80
A 10-year-old boy falls from monkey bars and sustains a distal radius fracture. Radiographs demonstrate a fracture line that passes through the metaphysis, traverses the physis, and exits through the epiphysis into the radiocarpal joint. What Salter-Harris classification does this represent?
Explanation
Question 81
A 15-year-old girl undergoes a posterior spinal fusion for adolescent idiopathic scoliosis. On postoperative day 4, she develops significant abdominal distension, bilious emesis, and marked weight loss. Which anatomic structure is most likely directly compressing the obstructed bowel segment?
Explanation
Question 82
According to the American Academy of Pediatrics (AAP) guidelines, routine ultrasound screening for DDH at 6 weeks of age is universally recommended for which of the following asymptomatic infants?
Explanation
Question 83
A 7-year-old boy sustained a Salter-Harris IV fracture of the distal femur 2 years ago. He now presents with a 3 cm leg length discrepancy and a progressive valgus deformity. CT mapping reveals a central physeal bar occupying 40% of the cross-sectional area of the physis. What is the best treatment option?
Explanation
Question 84
A 12-year-old boy with Duchenne muscular dystrophy presents with a progressive 45-degree thoracolumbar scoliosis. His Forced Vital Capacity (FVC) is currently 40% of predicted. What is the most appropriate management plan?
Explanation
Question 85
A 5-month-old infant has been treated in a Pavlik harness for 4 weeks for a completely dislocated right hip. A repeat ultrasound shows the hip remains persistently dislocated. What is the most appropriate next step in management?
Explanation
Question 86
A 6-month-old boy is diagnosed with infantile idiopathic scoliosis. He has a 35-degree left thoracic curve. Radiographs demonstrate a rib-vertebral angle difference (RVAD, or Mehta's angle) of 25 degrees. What is the most appropriate management?
Explanation
Question 87
Which of the following pediatric lower extremity physeal fractures carries the highest historical rate of premature growth arrest?
Explanation
Question 88
A 6-week-old female infant presents with a positive Ortolani sign on the left hip. Ultrasound shows an alpha angle of 45 degrees. What is the most appropriate next step in management?
Explanation
Question 89
A 2-year-old girl is undergoing closed reduction and spica casting for late-presenting developmental dysplasia of the hip. Which of the following intraoperative positioning parameters represents the highest risk for developing avascular necrosis of the femoral head?
Explanation
Question 90
In evaluating a 12-year-old girl with adolescent idiopathic scoliosis, which of the following combinations of factors indicates the highest risk for curve progression?
Explanation
Question 91
A newborn is diagnosed with congenital scoliosis secondary to a fully segmented hemivertebra. Which of the following imaging studies is most critical to obtain during the initial comprehensive evaluation?
Explanation
Question 92
A 10-year-old boy sustains a Salter-Harris type II fracture of the distal femur. Despite anatomic closed reduction and casting, the patient is at significant risk for which of the following long-term complications?
Explanation
Question 93
A 12-year-old boy developed a distal tibial physeal bar following a previous fracture. A scanogram reveals a 2 cm leg length discrepancy and 15 degrees of varus angulation. Mapping shows the bar involves 20% of the cross-sectional area of the physis peripherally. What is the most appropriate treatment?
Explanation
Question 94
A 4-month-old girl with left developmental dysplasia of the hip has been treated in a Pavlik harness for 4 weeks. Repeat ultrasound shows failure of reduction with the femoral head remaining chronically dislocated. What is the most appropriate next step in management?
Explanation
Question 95
A 6-month-old boy is noted to have a 25-degree left thoracic curve. Radiographs indicate a rib-vertebral angle difference (RVAD) of Mehta of 25 degrees. What is the most appropriate management?
Explanation
Question 96
A 14-year-old boy sustains an ankle injury resulting in a Salter-Harris III fracture of the anterolateral distal tibia. Which of the following best describes the pathomechanics of this specific fracture pattern?
Explanation
None
