AAOS Pediatric Orthopedic MCQs (Set 3): Scoliosis, DDH & Fractures | 2004 Board Review

Key Takeaway
This high-yield question set (Set 3) for the AAOS/ABOS exams focuses on core pediatric orthopedic topics. It covers the diagnosis, classification, and management of adolescent idiopathic scoliosis, developmental dysplasia of the hip (DDH), and common Salter-Harris growth plate fractures. Ideal for 2004 board review and OITE preparation.
AAOS Pediatric Orthopedic MCQs (Set 3): Scoliosis, DDH & Fractures | 2004 Board Review
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 10-year-old boy with an L1 myelomeningocele has a low-grade fever and a swollen thigh that is warm to touch and erythematous. AP and lateral radiographs are shown in Figures 24a and 24b. Management should consist of
Explanation
Question 2
A 6-year-old African-American boy with sickle cell disease has had pain and limited use of his right arm for the past 3 days. History reveals that he sustained a humeral fracture approximately 3 years ago. A lateral radiograph is shown in Figure 25. Based on these findings, a presumptive diagnosis of chronic osteomyelitis is made. What are the two most likely organisms?

Explanation
Question 3
A 7-year-old child is unresponsive, tachycardic, and has a systolic blood pressure of 50 mm Hg after being struck by a car. The patient is intubated and venous access is obtained. The secondary survey reveals an unstable pelvis. Despite adequate resuscitation, the patient continues to be hemodynamically unstable. What is the best course of action?
Explanation
Question 4
A 3-year-old boy with severe cerebral palsy is unable to sit independently and does not crawl. Examination reveals a 40-degree hip flexion contracture by the Thomas test and 25 degrees of passive abduction. A radiograph of the pelvis shows subluxation of both hips, with a migration index of 30%. Management should consist of
Explanation
Question 5
The parents of a 3-year-old girl who has had pain and swelling in the right ankle for the past 3 months now report that she has a limp and that the right knee and both ankles are painful and swollen. The limp and difficulty walking are most severe in the morning when the child first gets out of bed and are also more severe after extended walking. The parents deny fever, chills, weight loss, or night pain. Examination shows mild swelling and slightly restricted motion of the right knee and both ankles but is otherwise normal. In addition to initiation of treatment, the child should be referred to which of the following specialists?
Explanation
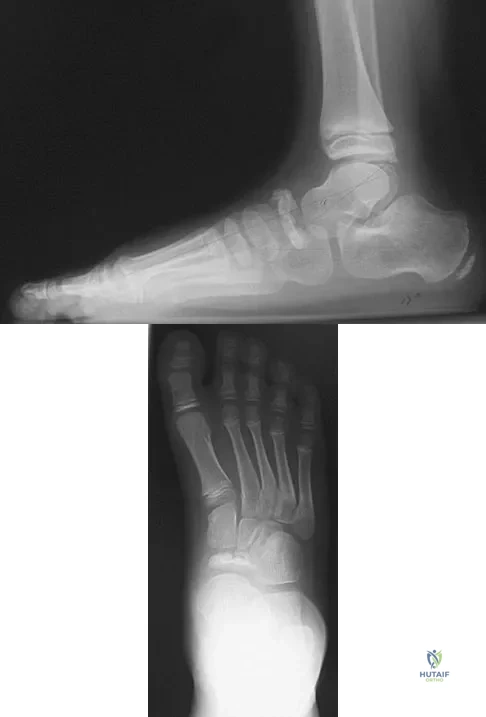
Question 6
A 9-year-old boy has pain over the midfoot medially with activity. Based on the findings shown in Figures 26a and 26b, which of the following is considered the most effective short-term management?
Explanation
Question 7
During the first 2 years of life, which of the following actions is most responsible for increasing structural stability of the physis?
Explanation
Question 8
Because the patient shown in Figure 27 can no longer fit in shoes, treatment of the deformity should consist of

Explanation
Question 9
Examination of a 9-year-old girl who injured her left elbow in a fall reveals tenderness and swelling localized to the medial aspect of the elbow. Motor and sensory examinations of the hand are normal, and circulation is intact. A radiograph is seen in Figure 28. Management should consist of

Explanation
Question 10
A 2-year-old child has refused to bear weight on his leg for the past 2 days. His parents report that he will crawl, has no fever, and has painless full range of motion of his hip and knee. Examination reveals no deformity or bruising, but there is mild swelling and tenderness over the anterior tibia. C-reactive protein, WBC count, and erythrocyte sedimentation rate studies are normal. Radiographs are negative. What is the best course of action?
Explanation
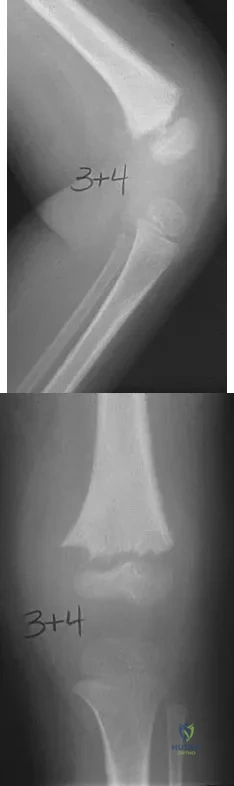
Question 11
A 7-year-old girl sustains the fracture shown in Figure 29a. Casting results in uneventful healing. Ten months later, the patient has a progressive valgus deformity of the right lower extremity. A radiograph is shown in Figure 29b. Management should now consist of

Explanation
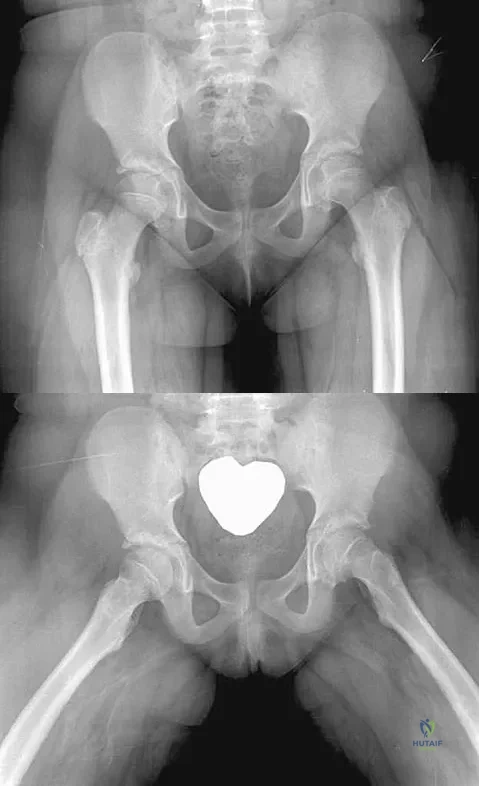
Question 12
An obese 10-year-old boy has had left groin pain and a limp for the past 2 months. Examination reveals decreased abduction and internal rotation. Laboratory studies show normal renal function and an elevated thyroid-stimulating hormone (TSH) level. AP and frog lateral radiographs of the pelvis are shown in Figures 30a and 30b. What is the best course of action?
Explanation
Question 13
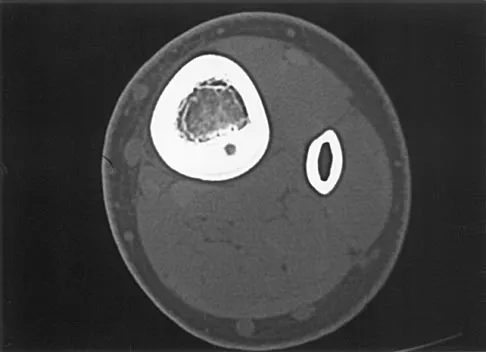
A 7-year-old boy has had chronic left leg pain that is worse at night but is not activity related. Use of nonsteroidal anti-inflammatory drugs for the past 6 months has failed to provide relief. A CBC count with differential, erythrocyte sedimentation rate, and C-reactive protein are within normal limits. Radiographs and a CT scan are shown in Figures 31a through 31c. Management should consist of

Explanation
Question 14
In patients with neurofibromatosis, what is the most important sign of impending rapid progression of a spinal deformity?
Explanation
Question 15
The fracture shown in Figure 32 is strongly indicative of what diagnosis?

Explanation
Question 16
Figures 33a and 33b show the radiographs of a 10-year-old girl who reports a 4-month history of medial foot pain after she was kicked while playing soccer. The pain is worse with activity and partially relieved by rest. Examination reveals tenderness directly over a prominent navicular tuberosity. Management should consist of

Explanation
Question 17
An 18-month-old child with obstetrical palsy has a maximum external rotation as shown in Figure 34. The parents should be advised that without surgical treatment the likelihood that glenoid dysplasia will develop is approximately what percent?

Explanation
Question 18
A 10-year-old boy has a painful, swollen knee after falling off his bicycle. Examination reveals no other injuries. Radiographs are shown in Figures 35a and 35b. Initial management of this fracture should consist of

Explanation
Question 19
Figures 36a and 36b show the radiographs of a 3-year old child who has a congenital upper extremity deformity. Which of the following features would be a major contraindication to a centralization procedure?

Explanation
Question 20
Examination of a 4-year old child with obstetrical palsy reveals weak deltoids, pectoralis major strength of 4-5, and normal hand function. External rotation of the shoulder is limited. What is the most appropriate surgical procedure to restore external rotation?
Explanation
Question 21
A 7-month-old girl has had a severe flatfoot deformity since birth. The talar head is prominent in the medial plantar arch of the foot. No other deformities of the spine or extremities are present. Motor and sensory examinations of the extremities are normal. Figures 37a through 37c show simulated weight-bearing AP and lateral radiographs and a planter flexion lateral view. What is the most likely diagnosis?

Explanation
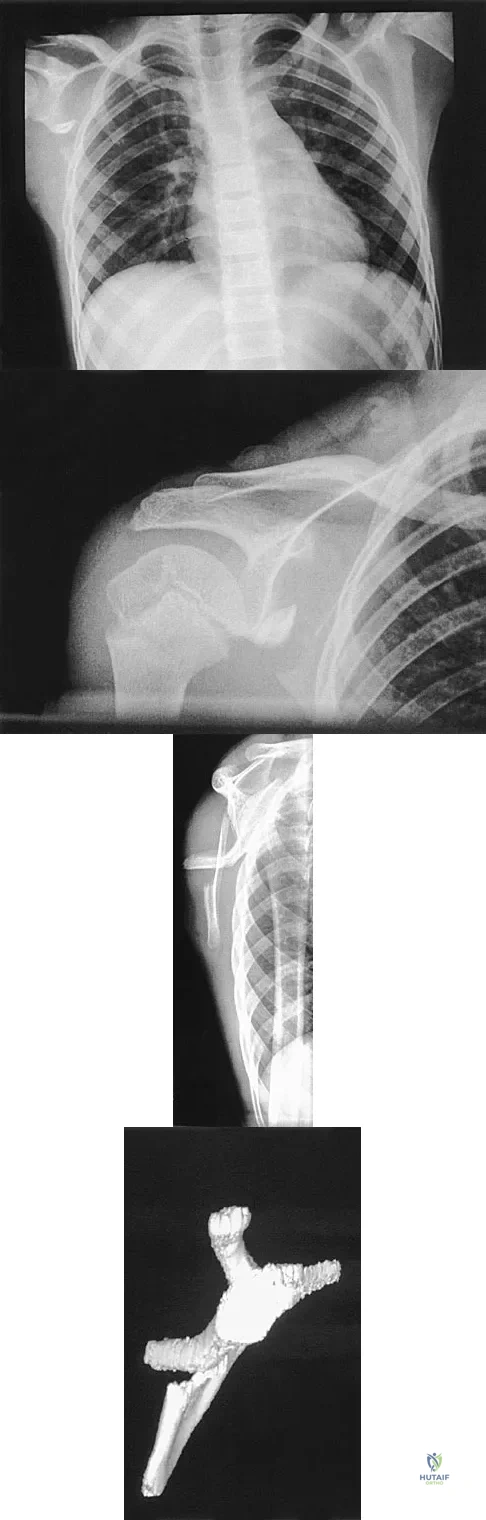
Question 22
A 12-year-old boy has severe left shoulder pain after being struck by an automobile. A chest radiograph, AP and lateral radiographs, and a CT scan with three-dimensional reconstruction of the scapula are shown in Figures 38a through 38d. Management should consist of
Explanation
Question 23
Figure 39 shows the radiograph of a 4-month old infant who has been undergoing weekly casting since birth for a congenital equinovarus deformity. Management should now consist of

Explanation
Question 24
A 1-year-old infant has the hand deformities shown in Figure 40. What pathologic process is the most likely cause of these deformities?

Explanation
Question 25
A 13-year-old girl with hallux valgus reports pain after playing basketball. Radiographs show a hallux valgus angle of 20 degrees, an intermetatarsal angle of 11 degrees, a distal metatarsal articular angle of 10 degrees, and a congruent joint. Management should consist of
Explanation
Question 26
A 9-month-old boy is being evaluated for progressive infantile idiopathic scoliosis. Radiographs demonstrate a left thoracic curve of 35 degrees and a rib-vertebra angle difference (RVAD) of 25 degrees. What is the most appropriate initial management?
Explanation
Question 27
A 6-week-old infant with developmental dysplasia of the hip (DDH) is placed in a Pavlik harness. Two weeks later, the parents report that the infant is no longer actively kicking the right leg. On examination, the knee lacks active extension. Which of the following is the most likely cause of this complication?
Explanation
Question 28
A 5-year-old boy sustains a completely displaced, extension-type supracondylar humerus fracture. Upon presentation, his hand is pink and well-perfused, but the radial pulse is absent. Following closed reduction and percutaneous pinning, the fracture is perfectly aligned, but the radial pulse remains absent while the hand remains pink. What is the most appropriate next step in management?
Explanation
Question 29
A 3-year-old girl is diagnosed with congenital scoliosis. Which of the following vertebral anomalies carries the highest risk for rapid curve progression and typically requires early surgical intervention?

Explanation
Question 30
A 2-year-old girl presents with a limp. Radiographs reveal a previously undiagnosed left-sided developmental dysplasia of the hip (DDH) with complete dislocation. What is the most appropriate definitive management?
Explanation
Question 31
A 4-year-old boy falls off monkey bars and sustains a displaced lateral condyle fracture of the humerus. Which of the following complications is most specifically associated with a failure of this fracture to unite?
Explanation
Question 32
A 12-year-old girl presents with adolescent idiopathic scoliosis. She is pre-menarchal. Her Risser sign is 1. Radiographs show a right thoracic curve of 34 degrees. What is the most widely accepted standard of care?
Explanation
Question 33
During open reduction for developmental dysplasia of the hip (DDH) through an anterior approach, several anatomic structures can block concentric reduction. Which structure typically causes the 'hourglass' constriction of the joint capsule?
Explanation
Question 34
A 3-year-old boy sustains an isolated, closed, length-stable diaphyseal femur fracture after a low-energy fall. He has no other injuries. What is the preferred treatment?
Explanation
Question 35
A 14-year-old boy with Duchenne muscular dystrophy develops a progressive 60-degree thoracolumbar scoliosis with significant pelvic obliquity. What is the most appropriate surgical approach?
Explanation
Question 36
When interpreting an infant hip ultrasound for DDH using the Graf method, the alpha angle is measured. What does the alpha angle specifically quantify?
Explanation
Question 37
A 13-year-old girl presents with ankle pain after twisting her leg. Radiographs reveal a Salter-Harris III fracture of the anterolateral aspect of the distal tibial epiphysis (Tillaux fracture). What is the pathomechanics of this injury?
Explanation
Question 38
A 13-year-old boy with adolescent idiopathic scoliosis presents with an atypical curve pattern (a sharp left-sided thoracic curve). He also reports mild headaches. Which of the following is the most appropriate next step in evaluating this patient?
Explanation
Question 39
Which of the following positions during spica casting for DDH places the infant at the highest risk for developing avascular necrosis of the femoral head?
Explanation
Question 40
An 8-year-old boy sustains a supracondylar fracture of the humerus. Six months later, he demonstrates a prominent cubitus varus deformity. What is the primary underlying cause of this malalignment?
Explanation
Question 41
A 7-year-old girl with a progressive 55-degree congenital scoliosis undergoes a posterior-only spinal fusion without instrumentation. Three years later, her curve has worsened significantly. What is the phenomenon responsible for this progression?
Explanation
Question 42
Which of the following is the most pathognomonic radiographic sign of non-accidental trauma (child abuse) in an infant?
Explanation
Question 43
A 14-year-old boy sustains a triplane fracture of the distal tibia. Radiographically, the fracture appears as a Salter-Harris type III fracture on the anteroposterior (AP) view. What does it resemble on the lateral view?
Explanation
Question 44
During a Pemberton pericapsular osteotomy for DDH, the osteotomy cut is directed toward and hinges on which of the following structures?
Explanation
Question 45
An 8-year-old boy falls on an outstretched hand and sustains an isolated plastic deformation of the ulna. On careful examination, he is unable to supinate his forearm and has pain at the elbow. What must be ruled out radiographically?
Explanation
Question 46
A 2-month-old infant is diagnosed with developmental dysplasia of the hip (DDH). In which of the following scenarios is the use of a Pavlik harness absolutely contraindicated?
Explanation
Question 47
A 13-year-old girl with adolescent idiopathic scoliosis (AIS) presents for evaluation. Her menarche was 6 months ago. Radiographs reveal a right thoracic curve of 35 degrees and a Risser stage of 0. What is the most appropriate management?
Explanation
Question 48
A 5-year-old boy sustains a severe extension-type supracondylar humerus fracture. On presentation, his hand is warm and pink, but the radial pulse is not palpable. After closed reduction and percutaneous pinning, the hand remains well-perfused with an oxygen saturation of 99%, but the pulse remains non-palpable. What is the next best step in management?
Explanation
Question 49
A 12-year-old non-ambulatory boy with Duchenne muscular dystrophy presents with a progressive neuromuscular scoliosis of 35 degrees. His forced vital capacity (FVC) is currently 45% of predicted. What is the most appropriate recommendation regarding his spinal deformity?
Explanation
Question 50
A 14-year-old boy sustains a juvenile Tillaux fracture of the ankle.
What is the characteristic mechanism of injury for this fracture pattern?
Explanation
Question 51
A 13-year-old girl sustains a twisting injury to her ankle. Radiographs reveal a triplane fracture. Which of the following best describes the typical Salter-Harris classification appearances on orthogonal radiographs?
Explanation
Question 52
An infant is being treated with a Pavlik harness for developmental dysplasia of the hip. At the 2-week follow-up, the parents report that the child has stopped extending the knee on the treated side. What is the most likely cause of this complication?
Explanation
Question 53
A 6-year-old boy falls from the monkey bars and sustains a lateral condyle fracture of the distal humerus. Radiographs show a Milch Type II fracture with 3 mm of displacement. What is the most appropriate management?
Explanation
Question 54
A 4-year-old child presents with a congenital spinal deformity. Radiographs demonstrate a fully unsegmented unilateral bar with a contralateral hemivertebra at the same level. What is the expected natural history of this specific deformity?
Explanation
Question 55
A 7-year-old boy with neurofibromatosis type 1 (NF1) presents with a progressive, short, sharp angular thoracic scoliosis. Radiographs demonstrate penciling of the ribs and severe apical wedging. What is the recommended surgical approach if operative intervention is deemed necessary?
Explanation
Question 56
A 7-year-old boy sustains a forearm injury. Radiographs show a plastic deformation of the ulna and an anterior dislocation of the radial head. According to the Bado classification, what type of Monteggia lesion is this?
Explanation
Question 57
A 3-year-old girl presents with a painless limp. Examination reveals a positive Trendelenburg sign on the right. Radiographs confirm an untreated, complete right-sided developmental dislocation of the hip (DDH). What is the most appropriate initial definitive management?
Explanation
Question 58
A 14-year-old patient with Marfan syndrome requires surgical correction for a rigid 65-degree scoliotic curve. During preoperative planning, an MRI of the spine is obtained. Which of the following findings is most commonly associated with Marfan syndrome and complicates surgical hardware placement?
Explanation
Question 59
An 8-year-old boy falls on an outstretched hand and sustains a fracture of the radial neck. Radiographs demonstrate 50 degrees of angulation.
What is the most appropriate initial step in management?

Explanation
Question 60
A 2-year-old boy is brought to the emergency department after tripping and falling while running on a carpet. Radiographs demonstrate a spiral fracture of the middle third of the femoral shaft. There are no signs of non-accidental trauma. What is the most appropriate treatment?
Explanation
Question 61
A 12-year-old obese boy presents with acute, severe hip pain and inability to bear weight after a minor twisting injury. Radiographs confirm a severe, unstable slipped capital femoral epiphysis (SCFE). What is the most devastating complication directly associated with the instability of this specific fracture pattern?
Explanation
Question 62
A 6-year-old girl sustains an extension-type Gartland III supracondylar humerus fracture. Upon initial clinical evaluation, she is unable to flex the interphalangeal joint of her thumb and the distal interphalangeal joint of her index finger. Which nerve is most likely injured?
Explanation
Question 63
During ultrasound screening for DDH in a 6-week-old infant, the Graf classification is utilized. What specifically does the alpha angle measure on the coronal ultrasound image?
Explanation
Question 64
A 6-month-old infant is diagnosed with infantile idiopathic scoliosis. Radiographs show a 25-degree left thoracic curve. Which of the following radiographic parameters indicates a high likelihood of curve progression?
Explanation
Question 65
A 4-month-old girl with developmental dysplasia of the hip (DDH) is being treated with a Pavlik harness. During a follow-up visit, the infant exhibits decreased spontaneous movement of the affected side's knee and no active knee extension. What is the most likely cause of this finding?
Explanation
Question 66
A 6-year-old boy falls on an outstretched hand and sustains an extension-type supracondylar humerus fracture, which is displaced posteromedially. Which nerve is most commonly at risk with this specific displacement pattern?
Explanation
Question 67
An 18-month-old girl is diagnosed with residual acetabular dysplasia following successful closed reduction of DDH. Her current acetabular index (AI) is 38 degrees. What is considered the upper limit of normal for the acetabular index at this age?
Explanation
Question 68
A 12-year-old boy with Duchenne muscular dystrophy (DMD) has a progressive scoliosis of 45 degrees. His forced vital capacity (FVC) is currently 40% of predicted. What is the most appropriate management?
Explanation
Question 69
A 13-year-old girl sustains an ankle injury. Radiographs show a Salter-Harris III fracture of the anterolateral aspect of the distal tibial epiphysis. What is the pathomechanics of this specific fracture?
Explanation
Question 70
A 3-year-old boy presents with a painless limp. Examination shows a positive Trendelenburg gait and Galeazzi sign on the right. Radiographs confirm an untreated right developmental dislocation of the hip. What is the most appropriate surgical management?
Explanation
Question 71
A 5-year-old boy undergoes open reduction and internal fixation for a displaced lateral condyle fracture of the humerus. Which of the following is the most common complication of this fracture despite anatomic reduction?
Explanation
Question 72
A newborn is noted to have congenital scoliosis secondary to a fully segmented hemivertebra at T8. Which of the following organ systems is most critical to evaluate for associated anomalies?
Explanation
Question 73
A 9-month-old infant is brought to the emergency department with a spiral fracture of the midshaft femur. The parents report the child caught his leg in the crib slats. What is the most appropriate next step in management?
Explanation
Question 74
A 13-year-old premenarcheal girl (Risser 0) presents with adolescent idiopathic scoliosis. Radiographs demonstrate a right thoracic curve of 32 degrees. What is the most appropriate treatment recommendation?
Explanation
Question 75
A newborn with arthrogryposis multiplex congenita is found to have bilateral rigid, dislocated hips. Which of the following statements regarding the management of these hips is most accurate?
Explanation
Question 76
A 2-year-old child presents with a sudden onset of limping and refusal to bear weight on the right leg. There is no history of significant trauma. Physical exam shows mild tenderness over the distal tibia. Initial AP and lateral radiographs are normal. What is the most appropriate initial management?
Explanation
Question 77
A 14-year-old gymnast presents with chronic low back pain exacerbated by extension. Radiographs show an L5-S1 isthmic spondylolisthesis with 25% slip (Grade 1). She has failed 6 months of conservative management. What is the most appropriate surgical treatment?
Explanation
Question 78
Following closed reduction and spica casting for DDH, a 1-year-old child's radiograph demonstrates failure of the ossific nucleus to appear within 1 year post-reduction. The femoral head appears broad and the neck is short. This presentation is most consistent with which complication?
Explanation
Question 79
A 10-year-old boy sustains a completely displaced Salter-Harris II fracture of the proximal humerus. What is the most acceptable management for this injury?
Explanation
Question 80
In the evaluation of typical adolescent idiopathic scoliosis (AIS), which of the following is commonly observed regarding the sagittal profile of the thoracic spine?
Explanation
Question 81
An 8-year-old boy sustains a mid-diaphyseal both-bone forearm fracture. What is the maximum acceptable angulation that will still allow for functional remodeling without significant loss of forearm rotation?
Explanation
Question 82
A 6-week-old female infant born breech is evaluated for DDH. Ultrasound examination using the Graf method reveals an alpha angle of 65 degrees and a beta angle of 45 degrees. What is the most appropriate management?
Explanation
Question 83
A 12-year-old girl with adolescent idiopathic scoliosis (AIS) presents with a right thoracic curve. She is premenarcheal, Risser 0, and her curve measures 35 degrees on standing PA radiograph. Which of the following is the most appropriate next step in management?
Explanation
Question 84
A 6-week-old female infant, born in the breech presentation, is evaluated for developmental dysplasia of the hip (DDH). Ultrasound reveals an alpha angle of 48 degrees and a beta angle of 80 degrees on the left hip. The hip is stable on clinical exam. What is the most appropriate management?
Explanation
Question 85
A 6-year-old boy sustains a widely displaced, extension-type supracondylar humerus fracture. Upon presentation, his hand is pink and well-perfused, but he is unable to actively flex the interphalangeal joint of his thumb. Which nerve is most likely injured?
Explanation
Question 86
A 4-year-old girl is diagnosed with congenital scoliosis secondary to a fully segmented hemivertebra at T8. Prior to surgical intervention, which of the following imaging studies is most critical to perform?
Explanation
Question 87
A 3-year-old child presents with a neglected right developmental dysplasia of the hip (DDH). She undergoes an open reduction, pelvic osteotomy, and femoral shortening osteotomy. Which of the following is the most devastating complication specific to the surgical treatment of DDH?
Explanation
Question 88
A 13-year-old boy presents with ankle pain following a fall. Radiographs demonstrate a Salter-Harris III fracture of the anterolateral aspect of the distal tibial epiphysis. What is the deforming force and the structure responsible for this avulsion fracture?
Explanation
Question 89
A 12-year-old non-ambulatory boy with Duchenne muscular dystrophy (DMD) has a progressive thoracolumbar scoliosis measuring 45 degrees. His forced vital capacity (FVC) is currently 40% of predicted. What is the most appropriate management of his spinal deformity?
Explanation
Question 90
A 5-month-old infant with developmental dysplasia of the hip has been treated in a Pavlik harness for 4 weeks. Repeat ultrasound reveals that the left hip remains persistently dislocated. What is the most appropriate next step in management?
Explanation
Question 91
A 6-year-old girl falls on an outstretched arm and sustains a lateral condyle fracture of the distal humerus with 3 mm of displacement. If this fracture goes untreated, what is the most likely late complication?
Explanation
Question 92
An 8-month-old boy is diagnosed with infantile idiopathic scoliosis with a left-sided thoracic curve measuring 25 degrees. The rib-vertebral angle difference (RVAD) of Mehta is 12 degrees. What is the most likely natural history of this curve?
Explanation
Question 93
A neonate with arthrogryposis multiplex congenita is found to have bilateral teratologic hip dislocations. The hips are stiff and cannot be reduced on physical examination. What is the standard recommendation for management?
Explanation
Question 94
A 13-year-old boy sustains a Salter-Harris II fracture of the proximal humerus. Radiographs show 40 degrees of apex anterior angulation and 50% translation. What is the most appropriate treatment?
Explanation
Question 95
A 14-year-old boy presents with progressive thoracic kyphosis and back pain. Standing lateral radiographs reveal a thoracic kyphosis of 65 degrees and anterior wedging of 6 degrees across three consecutive vertebrae. He is Risser 2. What is the most appropriate initial treatment?
Explanation
Question 96
During the radiographic evaluation of a 2-year-old child for developmental dysplasia of the hip (DDH), the orthopedist draws a horizontal line connecting the bilateral triradiate cartilages. What is the name of this reference line?
Explanation
None
