AAOS & ABOS Anatomy MCQs (Set 1): Upper Limb, Lower Limb & Spine | 2025 Board Prep
Key Takeaway
This high-yield Set 1 question bank for the AAOS/ABOS exams covers critical musculoskeletal anatomy. Questions focus on the intricate structures of the upper limb, lower limb, and spine, including bones, muscles, nerves, and vessels. Perfect for solidifying foundational knowledge for board certification and residency training.
AAOS & ABOS Anatomy MCQs (Set 1): Upper Limb, Lower Limb & Spine | 2025 Board Prep
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 65-year-old man with ankylosing spondylitis sustains an extension injury to his cervical spine. Two days later, a progressive neurologic deficit develops at the C6 level. An MRI scan is shown in Figure 1. What is the most likely diagnosis?
Explanation
Question 2
What are the most common portals for arthroscopic surgery of the ankle?
Explanation
Question 3
A patient who underwent primary total hip arthroplasty 7 years ago that resulted in excellent pain relief and a normal gait now reports pain and a limp. Postoperative and current AP radiographs are shown in Figures 2a and 2b. What is the most likely cause of the pathology seen?
Explanation
Question 4
The safest surgical approach to the insertion of the tibial posterior cruciate ligament uses the interval between which of the following muscles?
Explanation
Question 5
A 50-year-old man with no history of trauma reports new-onset back pain after doing some yard work the previous day. He reports pain radiating down his leg posteriorly and into the first dorsal web space of his foot. MRI scans are shown in Figures 3a through 3c. What nerve root is affected?
Explanation
Question 6
A 19-year-old wrestler has numbness along the radial aspect of the forearm after undergoing an open Bankart repair through an anterior deltopectoral approach. Motor weakness would be expected along with what other finding?
Explanation
Question 7
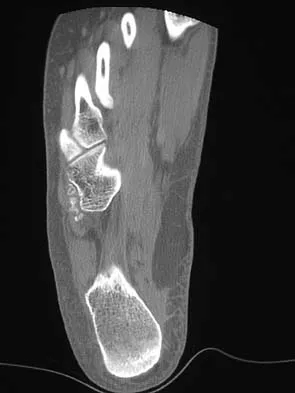
A 19-year-old man has had intermittent progressive knee pain with ambulation and pain at night following a rodeo accident 4 weeks ago. Figures 4a through 4e show the radiographs, a bone scan, CT scan, and T2-weighted MRI scan. What is the most likely diagnosis?
Explanation
Question 8
Figures 5a and 5b show the radiographs of an active 52-year-old man who has increasing knee pain and progressive varus deformity after undergoing total knee arthroplasty 7 years ago. Examination reveals a small effusion, but he has good motion and stability. What is the most likely diagnosis?
Explanation
Question 9
Which of the following best describes the course of the median nerve at the elbow?
Explanation
Question 10
A 62-year-old woman with soft-tissue calcifications and telangiectasia has severe pain in the left index, middle, ring, and little fingers. History reveals that she does not smoke. The clinical history and arteriogram shown in Figure 6 are consistent with which of the following conditions?
Explanation
Question 11
During excision of a Baker cyst, the base or stalk is usually found between the
Explanation
Question 12
A direct lateral (Hardinge) approach is used during total hip arthroplasty. The structure labeled A in Figure 7 is the
Explanation
Question 13
The dorsal digital cutaneous nerve of the great toe shown in Figure 8 is a branch of what nerve?
Explanation
Question 14
In hip arthroplasty, the location of the medial femoral circumflex artery is best described as
Explanation
Question 15
A 47-year-old man has acute right shoulder pain after falling off a ladder. The MRI scan shown in Figure 9 reveals
Explanation
Question 16
The oblique radiograph of the foot and the CT scan shown in Figures 10a and 10b show a patient whose symptoms have failed to respond to rest and non-steroidal anti-inflammatory drugs. What is the best course of action?
Explanation
Question 17
What is the typical MRI signal intensity of bone marrow affected by acute osteomyelitis?
Explanation
Question 18
Based on the appearance of the imaging studies shown in Figures 11a through 11c, what structure has most likely been injured?
Explanation
Question 19
In the anterior forearm approach to the distal radius (Henry approach), the radial artery is located between what two structures?
Explanation
Question 20
Following a radial nerve neurapraxia at or above the elbow, return of muscle function can be expected to start at the brachioradialis and return along which of the following progressions?
Explanation
Question 21
To preserve blood supply to the fractured bone seen in Figures 12a and 12b, care should be taken when exposing which of the following areas?
Explanation
Question 22
An axial T1-weighted MRI scan of the pelvis is shown in Figure 13. The arrow is pointing to what muscle?
Explanation
Question 23
Which of the following radiographic views best depicts a Hill-Sachs defect?
Explanation
Question 24
What structure provides the major blood supply to the humeral head?
Explanation
Question 25
Figure 14 shows an intra-articular gadolinium-enhanced MRI scan of a 52-year-old woman who has stopped playing tennis because of pain in her left shoulder while serving. What is the most likely diagnosis?
Explanation
Question 26
During a posterior approach to the hip (Moore or Southern), the short external rotators are tenotomized and reflected posteriorly. Which structure is most at risk if the piriformis is not carefully protected, specifically considering common anatomical variants?
Explanation
Question 27
When performing a direct lateral (deltoid-splitting) approach to the proximal humerus for open reduction and internal fixation, what is the maximum safe distance from the tip of the acromion to extend the split without risking denervation of the anterior deltoid?
Explanation
Question 28
During a lateral transpsoas approach (LLIF) to the lumbar spine at the L4-L5 level, the surgeon uses neuromonitoring to map the lumbar plexus. At this specific level, where is the lumbar plexus typically located relative to the psoas major muscle?
Explanation
Question 29
When establishing a posteromedial portal for knee arthroscopy to address a posterior horn medial meniscus tear, which anatomical structure is at greatest risk of iatrogenic injury during portal creation?
Explanation
Question 30
During a volar (Henry) approach to the proximal radius, the surgeon supinates the forearm to protect the posterior interosseous nerve (PIN). Supination moves the PIN in which direction relative to the anterior surgical exposure?
Explanation
Question 31
An extensile lateral approach to the calcaneus is planned for an intra-articular fracture. The surgeon must elevate a full-thickness flap to avoid wound necrosis. Which nerve is most at risk during the initial incision and flap elevation?
Explanation
Question 32
In the normal anatomical course of the cervical spine, the vertebral artery typically enters the transverse foramen at which vertebral level?
Explanation
Question 33
A 45-year-old cyclist presents with numbness in the little finger and weakness of the intrinsic hand muscles. Compression of the ulnar nerve is suspected in Guyon's canal. Which structure forms the floor of this canal?
Explanation
Question 34
When performing an anterior approach to the hip (Smith-Petersen), the superficial internervous plane is between the sartorius and tensor fasciae latae (TFL). Which nerve innervates the muscle forming the medial border of this interval?
Explanation
Question 35
During an anatomic reconstruction of the posterolateral corner of the knee, the surgeon must accurately identify the fibular insertion of the lateral collateral ligament (LCL). Where does the LCL insert relative to the popliteofibular ligament (PFL)?
Explanation
Question 36
When placing a pedicle screw at the L5 level, the starting point is identified at the intersection of the pars interarticularis, superior articular process, and transverse process. What is the typical medial angulation required to safely traverse the L5 pedicle?
Explanation
Question 37
A patient presents with medial winging of the scapula after an axillary node dissection, indicating injury to the long thoracic nerve. From which cervical nerve roots does this nerve originate?
Explanation
Question 38
Anterocentral portals for ankle arthroscopy are generally avoided due to the high risk of iatrogenic injury to which critical anatomical structure?
Explanation
Question 39
During an anterior approach to the elbow for a distal biceps tendon repair, the surgeon must carefully retract the lateral antebrachial cutaneous nerve. Between which two muscles does this nerve typically emerge in the distal arm?
Explanation
Question 40
During corrective spinal deformity surgery, the anterior spinal cord is vulnerable to ischemic injury. Which vascular territory is responsible for supplying the anterior spinal artery in the lower two-thirds of the spinal cord?
Explanation
Question 41
A patient undergoes a two-incision fasciotomy for a tibial shaft fracture complicated by compartment syndrome. Which muscle group must be carefully identified and released to ensure adequate decompression of the deep posterior compartment?
Explanation
Question 42
The recurrent motor branch of the median nerve innervates the thenar musculature. What is the most common anatomical relationship of this branch to the transverse carpal ligament?
Explanation
Question 43
During a medial approach to the distal tibia for minimally invasive plating of a pilon fracture, the surgeon must protect the saphenous nerve. Which vascular structure closely travels with the saphenous nerve in this region?
Explanation
Question 44
When placing half-pins for a humeral external fixator from a lateral approach, the radial nerve is at risk. At what location does the radial nerve predictably pierce the lateral intermuscular septum to enter the anterior compartment?
Explanation
Question 45
A 35-year-old patient undergoes a lymph node biopsy in the posterior triangle of the neck. Postoperatively, the patient is unable to abduct the arm past 90 degrees and demonstrates scapular winging. Injury to which of the following nerves is the most likely cause?
Explanation
Question 46
A 45-year-old sustains a displaced femoral neck fracture. Which of the following vessels provides the primary blood supply to the adult femoral head and is at greatest risk of disruption in this injury?
Explanation
Question 47
During the placement of pedicle screws at the L4 level, the surgeon breaches the inferior wall of the L4 pedicle. Which nerve root is most directly at risk of injury due to this specific breach?
Explanation
Question 48
During a volar forearm fasciotomy for compartment syndrome, the distal skin incision is deliberately directed ulnar to the palmaris longus tendon at the wrist crease. This maneuver primarily avoids injury to which of the following structures?
Explanation
Question 49
A surgeon is performing an extensile lateral approach to the calcaneus for an intra-articular fracture. Retraction of the full-thickness inferior flap places which of the following structures at highest risk?
Explanation
Question 50
During an anterior cervical discectomy and fusion (ACDF), the longus colli muscles are elevated to define the lateral margins. Overzealous lateral dissection and retraction past the longus colli places which structure at immediate risk?
Explanation
Question 51
During a trigger finger release, excessive division of the flexor sheath can lead to bowstringing of the flexor tendons. Which of the following pulleys is most critical to preserve to prevent this complication?
Explanation
Question 52
A patient presents with isolated varus instability at 30 degrees of knee flexion, but the knee is stable to varus stress at 0 degrees. Which of the following structures is the primary restraint to varus stress at 30 degrees of knee flexion?
Explanation
Question 53
During an arthroscopic rotator cuff repair, a portal is established posterior to the acromioclavicular joint. If the portal or dissection is extended more than 5 cm inferiorly from the lateral acromion edge, which nerve is at greatest risk of injury?
Explanation
Question 54
During an ilioinguinal approach to the acetabulum, severe hemorrhage is encountered while dissecting posterior to the superior pubic ramus. This is most likely due to an unligated vascular anastomosis between which two systems?
Explanation
Question 55
A patient undergoes a lateral transpsoas interbody fusion at L4-L5. Postoperatively, they display profound weakness in hip flexion and knee extension, along with anterior thigh numbness. Which nerve was most likely injured?
Explanation
Question 56
When performing an ulnar nerve transposition at the elbow, the surgeon must release all potential sites of compression. Which of the following represents the most proximal potential site of ulnar nerve compression?
Explanation
Question 57
In a patient with a suspected ankle syndesmotic injury, which ligament serves as the primary restraint to anterior translation of the distal fibula relative to the tibia?
Explanation
Question 58
Following surgical fixation of a proximal radius fracture, a patient cannot extend the interphalangeal joint of the thumb or the metacarpophalangeal joints of the fingers, but sensation is intact. Which nerve is injured, and through which muscle does it pass?
Explanation
Question 59
During the insertion of a thoracic pedicle screw at T7, the surgeon inadvertently directs the screw too far laterally, breaching the lateral wall of the pedicle. What anatomic structure is at greatest risk of direct injury?
Explanation
Question 60
An isolated fracture of the fibular shaft is approached surgically. The surgeon utilizes the internervous plane between the lateral and superficial posterior compartments of the leg. Which two muscles define this specific surgical interval?
Explanation
Question 61
A 45-year-old man sustains a proximal humerus fracture and subsequently demonstrates weakness in shoulder abduction and diminished sensation over the lateral deltoid. The affected nerve exits the axilla through the quadrangular space. Which of the following defines the superior border of this anatomic space?
Explanation
Question 62
During an anterior cervical discectomy and fusion (ACDF), aggressive lateral dissection places the vertebral artery at risk. In standard human anatomy, the vertebral artery typically enters the transverse foramen at which cervical level?
Explanation
Question 63
A surgeon is performing an open reduction internal fixation of an acetabular fracture via the ilioinguinal approach. If a Smith-Petersen extension is utilized, the superficial internervous plane lies between muscles innervated by which two nerves?
Explanation
Question 64
An 18-year-old athlete sustains a multi-ligamentous knee injury, including the posterolateral corner (PLC). During reconstruction, the surgeon must identify the femoral footprint of the popliteus tendon. Where is this footprint located relative to the lateral collateral ligament (LCL) attachment?
Explanation
Question 65
A 60-year-old man undergoes L4-L5 posterior spinal fusion. What is the classic anatomical landmark for the starting point of an L4 pedicle screw?

Explanation
Question 66
During open reduction internal fixation of a medial malleolus fracture, the surgeon explores the structures posterior to the medial malleolus. Moving from anterior to posterior, which structure lies immediately posterior to the flexor digitorum longus (FDL) tendon?
Explanation
Question 67
While performing an ilioinguinal approach for a transverse acetabular fracture, life-threatening hemorrhage occurs near the superior pubic ramus. This bleeding is most likely originating from the corona mortis, which represents an anastomosis between which two vascular systems?
Explanation
Question 68
A 45-year-old mechanic presents with an inability to actively extend his fingers and thumb at the metacarpophalangeal joints. Wrist extension is preserved but exhibits a strong radial deviation. Sensation in the upper extremity is fully intact. Which of the following anatomical structures is the most likely site of neural compression?
Explanation
Question 69
During a posterior approach to the hip for a total hip arthroplasty, excessive bleeding is encountered near the inferior border of the quadratus femoris. Ligation of the vessels in this area puts the primary blood supply to the femoral head at risk. Which artery is responsible for this blood supply and passes between the quadratus femoris and the obturator externus?
Explanation
Question 70
A surgeon is performing an L4-L5 posterior instrumented fusion. During the placement of a pedicle screw into the right L4 pedicle, the screw breaches the inferior wall of the pedicle. Which of the following neurologic structures is at greatest risk of direct mechanical injury?
Explanation
Question 71
A 28-year-old male is evaluated in the emergency department following a direct blow to the lateral aspect of his shoulder. He has weakness in shoulder abduction and decreased sensation over the lateral deltoid. Through which anatomical space does the injured nerve exit the axilla?
Explanation
Question 72
During a posterolateral approach to the distal fibula for fracture fixation, a cutaneous nerve is identified and protected. What is the standard anatomical course of this nerve at the level of the ankle?
Explanation
Question 73
An orthopaedic spine surgeon is performing an anterior cervical discectomy and fusion (ACDF). The surgeon must be aware of the vertebral artery anatomy. In most individuals, at what cervical vertebral level does the vertebral artery initially enter the transverse foramen?
Explanation
Question 74
A 34-year-old avid cyclist reports progressive numbness in his ring and small fingers along with weakness in finger abduction. Suspecting compression at Guyon's canal, surgical release is planned. Which structure forms the floor of this anatomical canal?
Explanation
Question 75
Following a traumatic knee dislocation, a patient is noted to have a dense foot drop and inability to evert the foot. The injured nerve is most vulnerable as it courses around the fibular neck. Between which two structures does this nerve pass as it enters the anterior compartment of the leg?
Explanation
Question 76
A 22-year-old collegiate volleyball player presents with isolated weakness in shoulder external rotation. Shoulder abduction and internal rotation are full strength. There is isolated atrophy of the infraspinatus fossa. Where is the most likely site of nerve compression?
Explanation
Question 77
During a lateral closing-wedge high tibial osteotomy, a retractor is carefully placed posterior to the proximal tibia to protect the neurovascular structures. Which of the following vessels is at greatest risk of injury if this retractor is incorrectly positioned directly posterior to the interosseous membrane?
Explanation
Question 78
A patient with an unstable pelvic ring fracture requires percutaneous iliosacral screw fixation at the S1 level. If the screw trajectory is placed too far anteriorly and inferiorly to the sacral ala, which nerve root is at highest risk of iatrogenic injury?
Explanation
Question 79
A 30-year-old man sustains a penetrating stab wound to the axilla. Physical examination demonstrates profound weakness in elbow flexion and decreased sensation along the lateral aspect of the forearm. From which portion of the brachial plexus does the injured nerve originate?
Explanation
Question 80
An orthopaedic surgeon uses the Smith-Petersen (anterior) approach for a pelvic osteotomy. This approach exploits an internervous plane between the sartorius and the tensor fasciae latae. Which of the following nerves innervates the sartorius?
Explanation
Question 81
A lateral transpsoas approach (LLIF) is utilized for interbody fusion at L4-L5. Postoperatively, the patient experiences quadriceps weakness and anterior thigh numbness. Which structure within the psoas major muscle was most likely injured?
Explanation
Question 82
A hand surgeon is repairing a flexor tendon laceration in Zone II of the index finger. Which of the following best describes the anatomical relationship of the flexor tendons within this specific zone?
Explanation
Question 83
During an anterior subcutaneous transposition of the ulnar nerve, the nerve is released from the cubital tunnel. What anatomical structure forms the roof of the cubital tunnel?
Explanation
Question 84
A surgeon utilizes the Smith-Petersen (direct anterior) approach for a total hip arthroplasty. To prevent denervation of the surrounding musculature, the dissection utilizes a true internervous plane. Which two nerves supply the muscles defining this superficial interval?
Explanation
Question 85
A surgeon is placing pedicle screws in the lumbar spine for a burst fracture. On an anteroposterior (AP) fluoroscopic view, the medial border of the pedicle corresponds to which structural boundary of the spinal canal?
Explanation
Question 86
An elite overhead throwing athlete presents with isolated weakness in external rotation of the shoulder. Examination reveals atrophy of the infraspinatus but normal supraspinatus bulk. Which anatomical structure is most likely compressing the affected nerve?
Explanation
Question 87
A patient sustains a traumatic knee dislocation and undergoes immediate reduction. Vascular evaluation is required due to the high risk of popliteal artery injury. Between which two distinct anatomical structures is the popliteal artery firmly tethered, making it susceptible to shear stress?
Explanation
Question 88
A patient sustains a spiral fracture of the distal third of the humerus (Holstein-Lewis fracture). They present with wrist drop and loss of finger extension. The nerve involved is at greatest risk of tethering as it passes through which anatomical structure?
Explanation
Question 89
A patient requires the creation of a posterolateral portal during ankle arthroscopy. Which nerve is at greatest risk of injury during the establishment of this portal?
Explanation
Question 90
A patient presents with the inability to form an "OK" sign, demonstrating an extended distal interphalangeal joint of the index finger and interphalangeal joint of the thumb during pinch. Sensation in the hand is completely normal. What is the most likely diagnosis?
Explanation
Question 91
Following a traumatic anterior shoulder dislocation, a patient complains of numbness over the lateral aspect of the shoulder. The injured nerve exits the axilla through the quadrangular space. Which of the following muscles forms the inferior border of this space?
Explanation
Question 92
A runner requires a lateral compartment fasciotomy for chronic exertional compartment syndrome. The surgeon must protect the superficial peroneal nerve. At what anatomical location does this nerve typically pierce the deep fascia to become subcutaneous?
Explanation
Question 93
Six weeks after undergoing volar plating for a distal radius fracture, a patient notes a sudden inability to actively extend the interphalangeal joint of the thumb. The tendon most likely ruptured wraps around which bony prominence?
Explanation
Question 94
Piriformis syndrome occurs due to compression of the sciatic nerve by the piriformis muscle. In the most common anatomical configuration, what is the relationship of the sciatic nerve to the piriformis muscle as it exits the greater sciatic foramen?
Explanation
None
