AAOS Spine Surgery MCQs (Set 1): Degenerative, Trauma & Deformity | Board Prep

Key Takeaway
This high-yield question set (Set 1) for the AAOS, ABOS, and OITE exams covers critical spine surgery topics. It includes detailed MCQs on degenerative spine conditions like disc herniation and stenosis, spinal trauma management, and principles of spinal deformity correction. Prepare for your board exams with solved practice questions.
AAOS Spine Surgery MCQs (Set 1): Degenerative, Trauma & Deformity | Board Prep
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
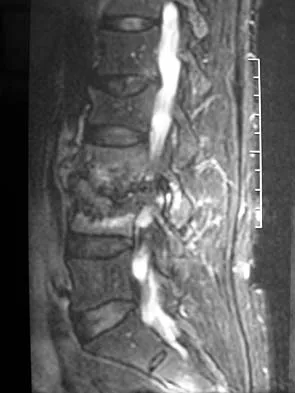
Figures 1a and 1b show the sagittal T2- and T1-weighted MRI scans of a 25-year-old intravenous drug abuser who has low back pain that is increasing in intensity. Laboratory studies show a WBC count of 10,000/mm3 and an erythrocyte sedimentation rate of 80 mm/h. Blood culture is negative. Initial management consist of
Explanation
Question 2
A 27-year-old man sustained a gunshot wound to the lumbar spine and undergoes an exploratory laparotomy. An injury to the cecum is identified and treated. Management should now include
Explanation
Question 3
A 68-year-old man reports a 1-year history of debilitating neck pain without neurologic symptoms. History reveals a C5-6 anterior diskectomy and bone grafting 10 years ago that provided good relief of arm and neck pain. Radiographs show evidence of fibrous union at C5-6, spondylotic disk narrowing at C4-5 and C6-7, and a fixed 2-mm subluxation at C3-4. Examination reveals cervical stiffness and discomfort at the extremes of movement. His neurologic examination is normal. Treatment should now consist of
Explanation
Question 4
Which of the following is considered the lowest level that a standard thoracolumbosacral orthosis (TLSO) can immobilize?
Explanation
Question 5
A 65-year-old man with ankylosing spondylitis has neck pain after falling back over his lawnmower, striking his thoracic spine, and forcing his neck into extension. Examination reveals subtle weakness of the intrinsics and finger flexors at approximately 4+/5. Initial management consists of immobilization in a rigid collar, and placing his head in the anatomic position. Radiographs reveal a subtle extension fracture of the lower cervical spine. Approximately 6 hours after the injury, he reports increasing paresthesias in his upper and lower extremities, and examination now shows his intrinsics are 2/5, finger flexors are 3/5, and his triceps are now weak at 4/5 on manual motor testing. In addition, his lower extremities now show weakness in both dorsal and plantar flexion of the ankle in the range of 4/5. Repeat radiographs appear unchanged. An MRI scan is shown in Figure 2. Management should now consist of
Explanation
Question 6
Figures 3a and 3b show the MRI scans of a patient with neck pain. What is the most likely diagnosis?
Explanation
Question 7
A Trendelenburg gait is most likely to be seen in association with
Explanation
Question 8
An otherwise healthy 70-year-old man has back and bilateral leg pain in an L5 distribution that is aggravated by standing more than 10 minutes or walking more than 100 feet. He has to sit to get relief. Neurologic and pulse examinations are normal. A radiograph and MRI scan are shown in Figures 4a and 4b. Treatment should consist of
Explanation
Question 9
Figures 5a and 5b show the radiograph and MRI scan of a patient who has severe mechanical neck pain but no neurologic problems. Biopsy and work-up show the lesion to be a solitary plasmacytoma. Treatment should consist of
Explanation
Question 10
A 71-year-old woman undergoes a posterior lumbar decompression and fusion from L4-S1. Thirty-six hours after the procedure, she reports severe right-sided chest pain and shortness of breath. Doppler ultrasound reveals a clot proximal to the knee within the femoral vein. A large pulmonary embolus is confirmed by CT angiography. The next most appropriate step in management should consist of
Explanation
Question 11
Figure 6 shows the lateral radiograph of a 22-year-old woman who has painful Scheuermanns's kyphosis in the middle and lower thoracic spine. When planning surgical correction using instrumentation, the distal aspect of the instrumentation should ideally extend to the
Explanation
Question 12
Figure 7 shows the radiograph of a 64-year-old man who has neck pain and weakness of the upper and lower extremities following a motor vehicle accident. Examination reveals 3/5 quadriceps and 4/5 hip flexors but no ankle dorsiflexion or plantar flexion. His intrinsics are 1/5, with finger flexors of 3/5. He is awake, alert, and cooperative. Management should consist of
Explanation
Question 13
What is the recommended insertion torque for halo pins in adults?
Explanation
Question 14
A 55-year-old woman with a history of untreated idiopathic scoliosis has had neurogenic claudication for the past several months. MRI reveals spinal stenosis at L2-L3, L3-L4, and L4-L5. Radiographs show a 45-degree lumbar curve from T10 to L4, with a degenerative spondylolisthesis at L4-L5. Laminectomy at the stenotic levels and stabilization of the deformity are planned. Which of the following is NOT considered an absolute indication for extending the fusion to the sacrum, rather than stopping at L5?
Explanation
Question 15
Which of the following findings is considered a contraindication for posterior decompression (with or without fusion) for myelopathy?
Explanation
Question 16
A patient reports progessive bilateral hand clumsiness and ataxia. Examination reveals a positive Hoffmann's sign and intrinsic atrophy. MRI reveals multilevel cervical spondylosis, and lateral flexion and extension radiographs show cervical kyphosis in the neutral position, with restoration of lordosis on extension. Which of the following procedures is most likely to result in poor long-term results?
Explanation
Question 17
A 45-year-old man seen in the emergency department reports a 1-week history of worsening low back pain and a progressive neurologic deficit in the S1 distribution. Examination reveals 2/5 strength in the gastrocnemius. Laboratory studies show a WBC count of 13,500/mm3 and an erythrocyte sedimentation rate of 74 mm/h. Radiographs of the lumbosacral spine show narrowing of the L5-S1 disk space, with irregularity of the end plates. A sagittal T2-weighted MRI scan is shown in Figure 8. Definitive management should consist of
Explanation
Question 18
In a retroperitoneal approach to the lumbar spine, what structure runs along the medial aspect of the psoas and along the lateral border of the spine?
Explanation
Question 19
What is the most likely primary cause of decreased success rates of bony fusion in smokers undergoing lumbar arthrodesis?
Explanation
Question 20
Flexion-distraction injuries of the thoracolumbar spine are most frequently associated with injury to what organ system?
Explanation
Question 21
What is the most common adverse postoperative complication of laminoplasty for multilevel cervical spondylotic myelopathy?
Explanation
Question 22
The thickest bone in the occiput is located
Explanation
Question 23
A patient who underwent an L5-S1 diskectomy 18 months ago has persistent pain in the left leg. Figures 9a and 9b show postoperative axial T1-weighted MRI scans at the L5-S1 level without and with gadolinium. What is the most likely diagnosis?
Explanation
Question 24
Which of the following factors is most closely associated with early postoperative migration of "stand-alone" lumbar interbody fusion cages?
Explanation
Question 25
If a laminectomy for spinal stenosis is performed, which of the following is an indication for concomitant arthrodesis at that level?
Explanation
Question 26
A 65-year-old man presents with progressive hand clumsiness and difficulty walking. Examination shows hyperreflexia in the lower extremities, a positive Hoffman's sign, and a wide-based gait. MRI reveals severe cervical stenosis from C3 to C6 with T2 signal change in the spinal cord, and a fixed cervical kyphosis of 15 degrees. What is the most appropriate surgical management?
Explanation
Question 27
A 45-year-old man falls from a height and sustains an L1 burst fracture. He is neurologically intact. CT and MRI show 15 degrees of kyphosis, 30% canal compromise, and an intact posterior ligamentous complex (PLC). According to the Thoracolumbar Injury Classification and Severity Score (TLICS), what is the most appropriate management?
Explanation
Question 28
A 72-year-old woman is planning to undergo reconstructive surgery for adult spinal deformity. To achieve optimal sagittal balance and minimize the risk of adjacent segment disease, her postoperative lumbar lordosis (LL) should be matched to which of the following pelvic parameters?
Explanation
Question 29
A 55-year-old man presents with right leg pain and weakness. Examination reveals 3/5 strength in right knee extension and a diminished right patellar reflex. Sensation is decreased over the medial aspect of the lower leg. An MRI shows a far-lateral disc herniation at the L4-L5 level. Which nerve root is most likely compressed?
Explanation
Question 30
In the treatment of acute traumatic cervical bilateral facet dislocations in an awake, alert, and cooperative patient without distracting injuries, what is the most appropriate initial management step?
Explanation
Question 31
A 25-year-old man sustains a seatbelt-type injury in a high-speed motor vehicle collision. Radiographs demonstrate a flexion-distraction (Chance) fracture of L2. Which of the following associated injuries must be carefully evaluated for?
Explanation
Question 32
A 68-year-old man with a long-standing history of ankylosing spondylitis presents to the emergency department with severe neck pain after a minor fall from a standing height. Neurologic examination is normal. Initial standard AP and lateral cervical spine radiographs appear unremarkable. What is the next best step in management?
Explanation
Question 33
A 30-year-old man presents with severe central cord syndrome following a hyperextension injury. MRI reveals severe cervical stenosis and cord edema, but no evidence of fracture or instability. Regarding the timing of surgical decompression, what does current literature suggest?
Explanation
Question 34
A 14-year-old girl is diagnosed with Adolescent Idiopathic Scoliosis (AIS). Her standing radiographs show a right thoracic curve of 55 degrees and a left lumbar curve of 35 degrees. On side-bending radiographs, the lumbar curve corrects to 15 degrees. According to the Lenke classification system, what type of curve pattern does she have?
Explanation
Question 35
A 60-year-old woman presents with classic symptoms of neurogenic claudication. MRI shows severe lumbar spinal stenosis at L4-L5. Which of the following anatomic structures is the primary contributor to dorsal compression of the dural sac in this condition?
Explanation
Question 36
A 45-year-old diabetic patient presents with 2 weeks of worsening back pain, fever, and new-onset weakness in the lower extremities. Laboratory markers show elevated ESR and CRP. MRI reveals L3-L4 discitis/osteomyelitis with a ventral epidural abscess compressing the cauda equina. What is the most appropriate next step?
Explanation
Question 37
A 65-year-old man undergoes a multi-level posterior cervical laminectomy and fusion (C3-C7) for cervical spondylotic myelopathy. On postoperative day 2, he develops isolated weakness in right shoulder abduction and external rotation (strength 2/5). His preoperative strength was normal, and long-tract signs are absent. What is the most likely diagnosis?
Explanation
Question 38
A 75-year-old woman suffers a Type II odontoid fracture after a ground-level fall. The fracture is displaced 3 mm posteriorly. She has severe medical comorbidities, including advanced COPD and heart failure. What is the most appropriate management?
Explanation
Question 39
A 65-year-old man presents with neurogenic claudication. What is the most common anatomical cause of central canal stenosis in this patient?
Explanation
Question 40
A 72-year-old woman presents with dropping objects, a broad-based gait, and hyperreflexia. A positive Hoffmann sign is noted. MRI shows severe C5-C6 stenosis with cord signal changes. What is the best next step in management?
Explanation
Question 41
A 45-year-old man fell from 10 feet. CT reveals an L1 burst fracture with 40% canal compromise. He is neurologically intact. MRI demonstrates an intact posterior ligamentous complex (PLC). According to the Thoracolumbar Injury Classification and Severity (TLICS) score, what is the recommended treatment?
Explanation
Question 42
Which of the following is considered a significant risk factor for nonunion of a Type II odontoid fracture treated nonoperatively with a halo vest?
Explanation
Question 43
A 13-year-old girl presents with adolescent idiopathic scoliosis. She has a right thoracic curve of 55 degrees. She is Risser 0 and premenarchal. What is the most appropriate management?
Explanation
Question 44
A 45-year-old man complains of severe anterior thigh pain and weakness in knee extension. MRI shows a far lateral (extraforaminal) disc herniation at the L3-L4 level. Which nerve root is most likely compressed?
Explanation
Question 45
A 68-year-old man with a history of cervical spondylosis sustains a hyperextension injury to his neck during a fall. He presents with severe motor weakness in his upper extremities but can move his lower extremities against gravity. What is the most likely diagnosis?
Explanation
Question 46
A 15-year-old gymnast presents with persistent lower back pain unresponsive to 6 months of conservative management. Radiographs show a grade II isthmic spondylolisthesis at L5-S1. What is the most appropriate surgical treatment?
Explanation
Question 47
A 55-year-old man with long-standing Ankylosing Spondylitis suffers a minor mechanical fall. He complains of new-onset, severe lower cervical pain. Initial plain radiographs of the cervical spine are obscured by the shoulders and appear inconclusive. What is the mandatory next step?
Explanation
Question 48
In planning reconstructive surgery for adult spinal deformity, achieving appropriate sagittal balance requires restoring lumbar lordosis (LL) to match the patient's pelvic incidence (PI). What is the widely accepted target formula to minimize the risk of adjacent segment disease and mechanical failure?
Explanation
Question 49
A 62-year-old man presents with progressive gait instability and hand clumsiness over the past 14 months. Examination reveals hyperreflexia, a positive Hoffmann sign, and a positive Romberg test. MRI shows severe stenosis at C5-C6 with T2 hyperintensity and T1 hypointensity within the spinal cord. What is the most significant predictor of poor postoperative neurological recovery in this patient?
Explanation
Question 50
A 75-year-old woman sustains a Type II odontoid fracture after a low-energy fall. Surgical stabilization is being considered due to a high risk of nonunion. Which of the following fracture characteristics is an absolute CONTRAINDICATION to anterior odontoid screw fixation?
Explanation
Question 51
A 14-year-old girl with adolescent idiopathic scoliosis (AIS) has a right thoracic curve of 55 degrees and a left lumbar curve of 35 degrees. On lateral bending radiographs, the thoracic curve corrects to 30 degrees, while the lumbar curve corrects to 15 degrees. According to the Lenke classification, what is her curve type?
Explanation
Question 52
A 30-year-old neurologically intact male sustains an L1 burst fracture. CT shows 30% canal compromise and 15 degrees of local kyphosis. MRI confirms an intact posterior ligamentous complex (PLC). According to the Thoracolumbar Injury Classification and Severity (TLICS) score, what is his total score and the recommended management?
Explanation
Question 53
Based on the Spine Patient Outcomes Research Trial (SPORT) data regarding the treatment of degenerative spondylolisthesis, which of the following statements is true?
Explanation
Question 54
A 65-year-old man with long-standing ankylosing spondylitis sustains a low-energy fall. He complains of severe neck pain but remains neurologically intact. Standard anterior-posterior and lateral radiographs of the cervical spine appear normal. What is the most appropriate next step in management?
Explanation
Question 55
Which of the following represents the classic Sorensen radiographic criteria required for the diagnosis of typical Scheuermann's kyphosis?
Explanation
Question 56
A 45-year-old man presents with severe left anterior thigh pain, decreased sensation over the medial leg, and weakness in knee extension. MRI reveals a far lateral (extraforaminal) disc herniation at the L4-L5 level on the left. Which nerve root is most likely compressed?
Explanation
Question 57
A 70-year-old man with preexisting cervical spondylosis presents with upper extremity weakness greater than lower extremity weakness after a hyperextension injury. Which spinal tract's medial fiber topography explains the disproportionate upper extremity involvement in this central cord syndrome?
Explanation
Question 58
In the preoperative surgical planning for an adult spinal deformity, restoring sagittal balance is critical to improving clinical outcomes. The optimal postoperative lumbar lordosis (LL) should be matched to which of the following spinopelvic parameters?
Explanation
Question 59
A 12-year-old boy with Down syndrome is being evaluated for participation in the Special Olympics. Flexion-extension cervical radiographs show an atlantodens interval (ADI) of 6 mm. He is completely asymptomatic and his neurologic examination is normal. What is the most appropriate recommendation?
Explanation
Question 60
A 65-year-old man presents with progressive clumsiness in his hands, difficulty buttoning his shirts, and an unsteady gait. Examination reveals hyperreflexia in the lower extremities, a positive Hoffmann sign bilaterally, and an inverted brachioradialis reflex. What is the most likely diagnosis?
Explanation
Question 61
A 72-year-old woman complains of bilateral buttock and posterior thigh pain that worsens after walking for 10 minutes. The pain is rapidly relieved when she sits down or leans forward over a shopping cart. The primary anatomic contributor to her condition is typically hypertrophy of which of the following structures?
Explanation
Question 62
When evaluating a patient with adult spinal deformity, achieving appropriate sagittal balance is a primary surgical goal. Which of the following spinopelvic parameter relationships correlates most closely with favorable health-related quality of life (HRQOL) scores?
Explanation
Question 63
A 12-year-old premenarchal girl presents with a right thoracic curve measuring 32 degrees on standing posteroanterior radiographs. Her Risser stage is 0. What is the most appropriate management?
Explanation
Question 64
A 35-year-old man sustains an L1 burst fracture in a motor vehicle collision. He is neurologically intact. Radiographs and CT show 20 degrees of local kyphosis, 40% loss of anterior vertebral body height, and 30% retropulsion of the posterior cortex into the canal. The posterior ligamentous complex is intact on MRI. What is the most appropriate treatment?
Explanation
Question 65
A 45-year-old man develops severe right lower extremity radiculopathy. MRI reveals a far lateral (extraforaminal) disc herniation at the L4-L5 level on the right side. Which nerve root is most likely compressed?
Explanation
Question 66
An 82-year-old man falls from a standing height and sustains a Type II odontoid fracture with 2 mm of posterior displacement. He is neurologically intact. Given his age and significant medical comorbidities, what is the most appropriate initial management considering the high nonunion rate?
Explanation
Question 67
A 24-year-old woman involved in a high-speed motor vehicle collision wearing only a lap belt presents with severe back pain. Radiographs reveal a transverse fracture through the spinous process, pedicles, and vertebral body of L2. What is the primary mechanism of this injury?
Explanation
Question 68
A 68-year-old man with known cervical spondylosis falls forward and strikes his chin, resulting in a hyperextension injury of the neck. Examination reveals motor weakness that is significantly worse in his upper extremities than in his lower extremities, along with patchy sensory loss. What is the most likely diagnosis?
Explanation
Question 69
A 55-year-old man with a long-standing history of ankylosing spondylitis presents to the emergency department complaining of new-onset neck pain after a minor fall. Plain radiographs show typical osteophyte formation and bamboo spine, but no clear fracture. He has no neurologic deficits. What is the mandatory next step in management?
Explanation
Question 70
A 30-year-old man sustains a traumatic spondylolisthesis of the axis (Hangman's fracture) following a motor vehicle collision. Radiographs show a bilateral fracture of the C2 with 4 mm of anterior displacement of C2 on C3 and severe angulation. This injury involves disruption of which primary anatomic structure?
Explanation
Question 71
A 26-year-old man presents after a diving accident. He is awake, alert, and cooperative. He complains of severe neck pain and has right-sided upper extremity weakness (C6 distribution). Radiographs reveal a right unilateral facet dislocation at C5-C6. What is the most appropriate initial management?
Explanation
Question 72
A 16-year-old boy presents with progressive mid-back pain and a noticeable rounding of his back. Standing lateral radiographs reveal a thoracic kyphosis of 60 degrees. Which of the following radiographic criteria is required to confirm a diagnosis of classic Scheuermann's disease?
Explanation
Question 73
A 15-year-old female gymnast complains of 6 months of low back pain that is exacerbated by extension activities. Radiographs demonstrate a pars interarticularis defect at L5 bilaterally and a 15% anterior translation of L5 on S1. Her neurologic examination is normal. What is the most appropriate initial management?
Explanation
Question 74
A 42-year-old man presents with 24 hours of severe lower back pain, bilateral lower extremity weakness, and new-onset urinary incontinence. Perianal sensation is significantly decreased. MRI confirms a massive extruded L4-L5 disc herniation compressing the thecal sac. What is the most critical prognostic factor for his return of bowel and bladder function following surgical decompression?
Explanation
Question 75
A 65-year-old woman presents with severe neurogenic claudication and low back pain. Upright lateral flexion-extension radiographs demonstrate a Grade 1 spondylolisthesis at L4-L5 with 4 mm of dynamic translation. After failing 6 months of comprehensive nonoperative management, what is the most appropriate surgical treatment?
Explanation
Question 76
A 58-year-old man of East Asian descent presents with progressive clumsiness in his hands, hyperreflexia, and gait instability. Radiographs and MRI show continuous ossification of the posterior longitudinal ligament (OPLL) from C3 to C6, causing severe multilevel cord compression. His cervical alignment is lordotic. What is the most appropriate surgical intervention?
Explanation
Question 77
A 35-year-old man falls from a height of 10 feet and sustains an L1 burst fracture. He is neurologically intact with normal perianal tone. MRI demonstrates an intact posterior ligamentous complex (PLC). His Thoracolumbar Injury Classification and Severity (TLICS) score is calculated. What is the most appropriate management?
Explanation
Question 78
An 82-year-old man with advanced dementia and severe chronic obstructive pulmonary disease presents after a ground-level fall. CT scan reveals a Type II odontoid fracture with 3 mm of posterior displacement. He is neurologically intact. What is the recommended initial management?
Explanation
Question 79
A 62-year-old woman is planning to undergo reconstructive surgery for adult spinal deformity. Preoperative measurements show her pelvic incidence (PI) is 60 degrees. To achieve optimal sagittal balance postoperatively, what should her target lumbar lordosis (LL) ideally be?
Explanation
Question 80
A 60-year-old man with a known history of severe cervical spondylosis presents after sustaining a hyperextension injury in a motor vehicle collision. He has severe motor weakness in his hands and arms (1/5) but can still move his lower extremities against gravity (4/5). He retains intact perineal sensation. What is the most likely diagnosis?
Explanation
Question 81
A 24-year-old woman involved in a high-speed motor vehicle collision wearing only a lap belt sustains a flexion-distraction injury (Chance fracture) at L2. She is neurologically intact. What associated injury must be rigorously ruled out before definitive spinal management?
Explanation
Question 82
A 55-year-old man with a 20-year history of ankylosing spondylitis presents with acute, severe localized lower back pain after a minor slip and fall. Initial radiographs are equivocal, but a CT scan demonstrates a transdiscal fracture at T11-T12. He is neurologically intact. What is the most appropriate definitive management?
Explanation
Question 83
A 65-year-old man presents with progressive difficulty buttoning his shirts, frequent tripping, and bilateral hand numbness. Physical examination reveals a positive Hoffmann sign bilaterally, hyperreflexia in the lower extremities, and an unsteady, wide-based gait. MRI of the cervical spine shows severe canal stenosis at C4-C5 and C5-C6 with T2 signal changes in the spinal cord. What is the most appropriate next step in management?
Explanation
Question 84
When evaluating a 60-year-old female for adult degenerative scoliosis and severe low back pain, standing full-length spine radiographs are obtained. Which of the following radiographic parameters is most closely correlated with improved health-related quality of life (HRQOL) scores following corrective surgery?
Explanation
Question 85
An 82-year-old man falls from a standing height and sustains a Type II odontoid fracture with 3 mm of posterior displacement. He is neurologically intact but has severe neck pain. He has a history of severe COPD, ischemic heart disease, and osteoporosis. What is the most appropriate initial management?
Explanation
Question 86
A 28-year-old construction worker falls from a scaffolding, sustaining an L1 burst fracture. He is neurologically intact. Upright radiographs show 20 degrees of local kyphosis, and CT shows 40% canal compromise. The posterior ligamentous complex is intact on MRI. According to the Thoracolumbar Injury Classification and Severity (TLICS) score, what is the most appropriate treatment?
Explanation
Question 87
A 45-year-old female presents with persistent lower back pain and bilateral L5 radiculopathy that has failed 6 months of conservative management. Flexion-extension radiographs reveal a Grade II L4-L5 degenerative spondylolisthesis with 5 mm of dynamic instability. MRI shows severe bilateral foraminal stenosis at L4-L5. Which of the following is the most appropriate surgical intervention?
Explanation
Question 88
A 34-year-old male presents to the emergency department with acute onset of severe lower back pain, bilateral sciatica, and perianal numbness after lifting a heavy box. He reports a recent episode of urinary incontinence, and his post-void residual volume is 350 mL. An emergent MRI of the lumbar spine demonstrates a massive central L4-L5 disc herniation. What is the most critical time frame for surgical decompression to optimize the recovery of bladder and bowel function?
Explanation
None
