AAOS Orthopedic MCQs (Set 3): Pediatric Femur Fractures, DDH & Scoliosis | Board Review

Key Takeaway
This high-yield question set for AAOS/ABOS/OITE exams focuses on crucial pediatric orthopedic topics. Questions cover diagnosis, classification, and management of pediatric femur fractures, developmental dysplasia of the hip (DDH), and various aspects of pediatric scoliosis, essential for board preparation.
AAOS Orthopedic MCQs (Set 3): Pediatric Femur Fractures, DDH & Scoliosis | Board Review
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 14-year-old girl has a painful hallux valgus deformity that has not responded to shoe modifications. Figure 21 shows a standing AP radiograph. What is the most appropriate surgical procedure?

Explanation
Question 2
Figure 22 shows the radiograph of a 7-year-old boy who underwent retrograde elastic nailing of a femoral shaft fracture. What is the most common problem following this procedure?

Explanation
Question 3
A newborn girl with an isolated unilateral dislocatable hip is placed in a Pavlik harness with the hips flexed 100 degrees and at resting abduction. Figure 23 shows an ultrasound obtained 2 weeks later. What is the next step in management?

Explanation
Question 4
During the early swing phase of the normal gait cycle, what lower extremity muscle is primarily contracting?
Explanation
Question 5
A 6-month-old child is seen in the emergency department with a spiral fracture of the tibia. The parents are vague about the etiology of the injury. There is no family history of a bone disease. In addition to casting of the fracture, initial management should include
Explanation
Question 6
What is the primary indication for performing an arthroscopic synovectomy on a patient with hemophilia that is the result of factor VIII deficiency?
Explanation
Question 7
The rate of complications after in situ pinning of a chronic slipped capital femoral epiphysis is highest with placement of the screw in what quadrant of the femoral head?
Explanation
Question 8
What is the incidence and significance of anterior cruciate ligament laxity following tibial eminence fractures in skeletally immature individuals?
Explanation
Question 9
A full-term newborn has webbing at the knees, rigid clubfeet, a Buddha-like posture of the lower extremities, and no voluntary or involuntary muscle action at and below the knees. Radiographs of the spine and pelvis reveal an absence of the lumbar spine and sacrum. What maternal condition is associated with this diagnosis?
Explanation
Question 10
Figure 24 shows the sitting AP and lateral spinal radiographs of a nonambulatory 12½-year-old boy with Duchenne muscular dystrophy who is being evaluated for scoliosis. The lumbar curve from T12 to L5 measures 36 degrees, and the thoracic curve from T3 to T12 measures 24 degrees on the AP radiograph. He has 5 degrees of pelvic obliquity. His forced vital capacity is 45% of predicted for height and weight. What is the most appropriate treatment for the spinal deformity?

Explanation
Question 11
A 3-year-old child has refused to walk for the past 2 days. Examination in the emergency department reveals a temperature of 102.2 degrees F (39 degrees C) and limited range of motion of the left hip. An AP pelvic radiograph is normal. Laboratory studies show a WBC count of 9,000/mm3, an erythrocyte sedimentation rate (ESR) of 65 mm/h, and a C-reactive protein level of 10.5 mg/L (normal < 0.4). What is the next most appropriate step in management?
Explanation
Question 12
A 2-year-old girl has had a swollen right knee for the past 7 weeks. There is no history of significant trauma, and she has not had a fever or been ill. Her parents report that she is stiff in the morning but otherwise does not report pain. A CBC count and erythrocyte sedimentation rate are normal. Treatment with naproxen at appropriate doses for the past 2 weeks has resulted in some improvement. Radiographs show only soft-tissue swelling. Examination reveals a healthy-appearing child with a warm and swollen right knee that is only slightly tender but lacks full extension by 20 degrees. What is the next most appropriate step in management?
Explanation
Question 13
A 12-year-old girl has back pain after falling 20 feet and landing in the sitting position. She has no fractures or other injuries, and her neurologic examination is normal. A lateral radiograph, transverse CT scan, and reformatted sagittal CT scan are shown in Figures 25a through 25c. Which of the following methods is associated with the best long-term outcome?

Explanation
Question 14
Figure 26 shows the radiograph of an otherwise healthy Caucasian 5-year-old boy who has a painless limp. What is the best treatment option?

Explanation
Question 15
A 12-year-old girl who has a history of frequent tripping and falling also has bilateral symmetric hand weakness, high arched feet, absent patellar and Achilles tendon reflexes, and excessive wear on the lateral border of her shoes. She reports that she has multiple paternal family members with similar deformities. She most likely has a defect of what protein?
Explanation
Question 16
A 12-year-old boy with an ankle fracture undergoes closed reduction under sedation in the emergency department. Figure 27 shows a lateral radiograph of the ankle after two attempts at closed reduction. Based on these findings, treatment should now consist of

Explanation
Question 17
A 9-year-old girl has pain over the fifth toe that is aggravated by shoe wear. Clinical photographs are shown in Figures 28a and 28b. Treatment of this deformity should consist of

Explanation
Question 18
What acetabular procedure for developmental dysplasia of the hip does not require a concentric reduction of the femoral head in the acetabulum?
Explanation
Question 19
Figure 29 shows the AP radiograph of a 14-year-old boy. The radiographic findings are most consistent with what pathologic process?
Explanation
Question 20
A 5-year-old boy has had pain in the right foot for the past month. Examination reveals tenderness and mild swelling in the region of the tarsal navicular. Radiographs are shown in Figure 30. Management should consist of

Explanation
Question 21
A 9-year-old child sustained a fracture-dislocation of C-5 and C-6 with a complete spinal cord injury. What is the likelihood that scoliosis will develop during the remaining years of his growth?
Explanation
Question 22
Figures 31a and 31b show the radiograph and MRI scan of an otherwise normal 3-month-old infant who has a spinal deformity. MRI reveals no intraspinal anomalies. What is the next step in management?
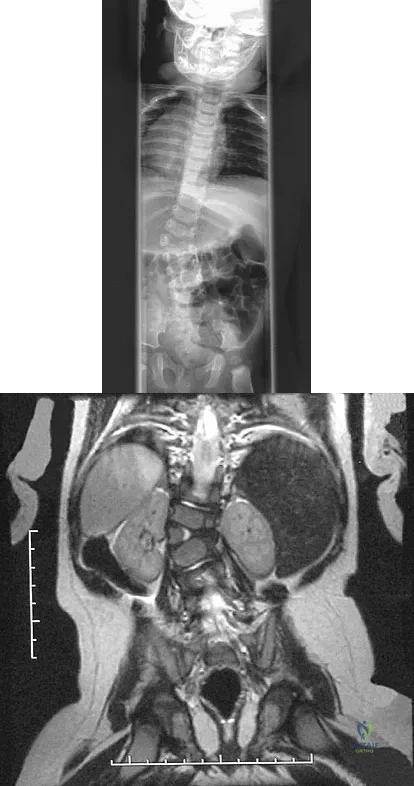
Explanation
Question 23
A 22-month-old girl has cerebral palsy. Which of the following findings is a good prognostic indicator of the child's ability to walk in the future?
Explanation
Question 24
The husband of a 22-year-old woman has hypophosphatemic rickets. The woman has no orthopaedic abnormalities, but she is concerned about her chances of having a child with the same disease. What should they be told regarding this disorder?
Explanation
Question 25
A 9-year-old boy sustained a traumatic brain injury and right lower extremity trauma in an accident involving a motor vehicle and a pedestrian. Initial evaluation in the emergency department reveals an obtunded patient who is breathing spontaneously and withdraws appropriately to painful stimuli. After initial resuscitation and stabilization, a CT scan reveals a right parietal intracranial hemorrhage. Radiographs of the swollen right thigh are shown in Figures 32a and 32b. Management of the fractured femur should ultimately consist of

Explanation
Question 26
An 11-year-old boy sustains a transverse diaphyseal femur fracture. The surgeon elects to proceed with rigid intramedullary nailing. To minimize the risk of iatrogenic avascular necrosis (AVN) of the femoral head, which entry point is most appropriate?
Explanation
Question 27
A 4-week-old infant with developmental dysplasia of the hip (DDH) has been treated in a Pavlik harness for 1 week. The mother brings the child in, noting that the infant is no longer actively kicking or extending the knee on the affected side. What is the most appropriate next step in management?
Explanation
Question 28
A 12-year-old pre-menarcheal girl presents with a right thoracic adolescent idiopathic scoliosis (AIS).
Her Risser stage is 0, and her curve measures 32 degrees on a standing PA radiograph. What is the most evidence-based management strategy?

Explanation
Question 29
A 3-year-old child sustains an isolated spiral fracture of the femoral shaft and is managed with a hip spica cast. During reduction, how much initial fracture shortening is most appropriate to accept to compensate for anticipated overgrowth?
Explanation
Question 30
A 7-month-old girl presents for her first pediatric orthopedic evaluation and is diagnosed with bilateral DDH. Ultrasound confirms bilateral dislocated hips that are irreducible on dynamic examination. What is the most appropriate initial treatment?
Explanation
Question 31
A 9-month-old boy is referred for a 25-degree left thoracic scoliosis.
Radiographs demonstrate a rib-vertebral angle difference (RVAD) of 25 degrees. What is the most likely natural history and appropriate treatment?
Explanation
Question 32
An 8-year-old boy is treated with titanium elastic nails for a midshaft transverse femur fracture.
What is the most commonly reported complication associated with this specific surgical intervention?

Explanation
Question 33
A 4-year-old girl with residual DDH requires an open reduction and pelvic osteotomy. The surgeon plans a Salter innominate osteotomy. This osteotomy relies on a hinge at which of the following structures to provide anterolateral coverage?
Explanation
Question 34
A 12-year-old boy with Duchenne muscular dystrophy presents with a 45-degree sweeping thoracolumbar neuromuscular scoliosis. His forced vital capacity (FVC) is 40% of predicted. What is the most appropriate management?
Explanation
Question 35
A 6-week-old female infant is evaluated for DDH. Coronal ultrasound of the right hip reveals an alpha angle of 55 degrees and a beta angle of 65 degrees. According to the Graf classification, what is the appropriate management?
Explanation
Question 36
A 6-year-old girl sustains a closed, completely displaced subtrochanteric femur fracture.
What is the most appropriate fixation strategy to minimize complications while facilitating early mobilization?
Explanation
Question 37
A 10-year-old boy with a history of DDH treated by closed reduction at age 1 presents for follow-up. Radiographs demonstrate a progressive coxa valga deformity and a short femoral neck, but the medial physis remains open. According to the Kalamchi-MacEwen classification, what type of vascular insult occurred?
Explanation
Question 38
A 10-year-old boy presents with a 30-degree left-sided thoracic scoliosis.
His neurological examination is normal. What is the most appropriate next step in his diagnostic workup?

Explanation
Question 39
A 10-month-old infant who is not yet cruising or walking presents to the emergency department with a swollen, painful thigh. Radiographs reveal a closed spiral fracture of the mid-diaphyseal femur. What is the most critical next step in management?
Explanation
Question 40
A 5-year-old girl with residual DDH undergoes preoperative planning for a pelvic osteotomy. The chosen technique is an incomplete pericapsular osteotomy that hinges on the triradiate cartilage, dynamically reducing the volume of the acetabulum. Which osteotomy is described?
Explanation
Question 41
When classifying adolescent idiopathic scoliosis using the Lenke system, the lumbar spine modifier is determined by the relationship of the center sacral vertical line (CSVL) to the lumbar vertebrae. What defines a Lumbar Modifier B?
Explanation
Question 42
A 4-week-old infant sustains a closed midshaft femur fracture after a roll-over injury in a stroller. What is the most appropriate initial management?
Explanation
Question 43
A 10-year-old boy weighing 55 kg (121 lbs) sustains a length-unstable, comminuted midshaft femur fracture. Which of the following surgical options is most appropriate?
Explanation
Question 44
A 7-year-old girl sustains a Delbet type II (transcervical) femoral neck fracture. Despite urgent closed reduction and internal fixation, she is at the highest risk for which of the following complications?
Explanation
Question 45
A 3-year-old child sustains a closed midshaft femur fracture and is treated with a one-and-a-half spica cast. What is the maximum acceptable amount of fracture overriding to anticipate the overgrowth phenomenon?
Explanation
Question 46
A 4-month-old girl is being treated in a Pavlik harness for developmental dysplasia of the hip (DDH). Her parents report that she is no longer actively extending her right knee. What is the most likely cause of this complication?
Explanation
Question 47
A 6-week-old infant undergoes hip ultrasonography for suspected developmental dysplasia. The alpha angle is measured at 62 degrees and the beta angle is 50 degrees. According to the Graf classification, what is the appropriate management?
Explanation
Question 48
A 12-year-old premenarchal girl (Risser 0) has a right thoracic adolescent idiopathic scoliosis (AIS) curve of 35 degrees. Which of the following is the most appropriate management?
Explanation
Question 49
A 2-year-old boy presents with congenital scoliosis secondary to a fully segmented hemivertebra at T8. In addition to full spine radiographs, what routine screening must be obtained?
Explanation
Question 50
An 11-year-old boy requires rigid intramedullary nailing for a transverse femur fracture. To minimize the risk of iatrogenic avascular necrosis (AVN), what is the optimal entry point?
Explanation
Question 51
A 9-month-old infant undergoes closed reduction and spica casting for late-diagnosed DDH. Postoperatively, the hip is noted to be immobilized in 65 degrees of abduction. What complication is the child at highest risk for?
Explanation
Question 52
A 10-year-old boy presents with a left-sided thoracic scoliosis of 25 degrees. His neurologic examination is unremarkable. What is the most appropriate next step in evaluation?
Explanation
Question 53
An 18-month-old girl presents with untreated developmental dysplasia of the hip (DDH). She has a positive Galeazzi sign and limited hip abduction. What is the most appropriate initial intervention?
Explanation
Question 54
In an infant with idiopathic scoliosis, which radiographic parameter most strongly predicts the likelihood of curve progression?
Explanation
Question 55
A 2-year-old child is placed in a 90/90 spica cast for a midshaft femur fracture. This specific positioning (90 degrees hip flexion, 90 degrees knee flexion) is primarily chosen to control which of the following?
Explanation
Question 56
A 6-year-old boy sustains a midshaft femur fracture and is treated with flexible intramedullary nails. Which of the following is the most common complication associated with this treatment modality?
Explanation
Question 57
A 6-week-old female is treated with a Pavlik harness for developmental dysplasia of the hip (DDH). After 1 week, the mother notes the child is no longer kicking her right leg, and the knee rests in extension. What is the most likely cause?
Explanation
Question 58
Which of the following factors indicates the highest risk for curve progression in a patient with Adolescent Idiopathic Scoliosis (AIS)?
Explanation
Question 59
A 9-month-old boy presents with a spiral fracture of the femoral shaft. He is not yet walking independently. What is the most appropriate next step in management?
Explanation
Question 60
When evaluating a 4-week-old infant's hip using Graf's ultrasound method, an alpha angle of 45 degrees is noted. What does this angle primarily measure?
Explanation
Question 61
A 9-month-old boy is diagnosed with infantile idiopathic scoliosis. His rib-vertebral angle difference (RVAD) of Mehta is measured at 25 degrees. What is the most likely clinical course?
Explanation
Question 62
A 13-year-old boy weighing 65 kg sustains a length-unstable transverse femoral shaft fracture. If a rigid locked intramedullary nail is selected, which entry point minimizes the risk of iatrogenic avascular necrosis?
Explanation
Question 63
A 4-year-old girl with untreated DDH is scheduled for open reduction and an innominate osteotomy. The planned procedure involves a complete transiliac osteotomy that redirects the entire acetabulum by hinging on the pubic symphysis. Which osteotomy is being described?
Explanation
Question 64
A 3-year-old girl is found to have congenital scoliosis due to a fully segmented hemivertebra. Which of the following screening tests must be obtained to evaluate for commonly associated anomalies?
Explanation
Question 65
A 3-year-old boy is treated in a 90-90 hip spica cast for a femoral shaft fracture. He presents 2 weeks later with excessive crying, bilious vomiting, and food refusal. What is the most likely diagnosis?
Explanation
Question 66
During closed reduction of a dislocated hip in a 9-month-old child, the Ramsey safe zone is assessed. What defines the boundaries of this zone?
Explanation
Question 67
In the Lenke classification for Adolescent Idiopathic Scoliosis, how is a structural minor curve defined on supine side-bending radiographs?
Explanation
Question 68
A 7-year-old child weighing 45 kg sustains a highly comminuted, length-unstable femur fracture. What is the most appropriate fixation method to maintain length and alignment?
Explanation
Question 69
A 12-year-old girl with a history of DDH treated with closed reduction at infancy presents with a limp. Radiographs show a shortened, widened femoral neck and an enlarged, flat femoral head. This deformity is most likely a sequela of which complication?
Explanation
Question 70
A 14-year-old non-ambulatory male with Duchenne muscular dystrophy has a 60-degree thoracolumbar scoliosis and severe pelvic obliquity. What is the most appropriate surgical strategy?
Explanation
Question 71
A 6-month-old female presents with an asymmetric thigh crease. An AP pelvis radiograph is obtained. Which of the following acetabular index measurements is considered normal for this age?
Explanation
Question 72
A 4-year-old boy undergoes application of a hip spica cast for a transverse midshaft femur fracture. The surgeon intentionally positions the fracture with 1.5 cm of overlap. What is the primary rationale for this?
Explanation
Question 73
In a young child with early-onset scoliosis and multiple fused ribs, vertical expandable prosthetic titanium rib (VEPTR) surgery is indicated primarily to treat or prevent which condition?
Explanation
Question 74
When performing an anterior (Smith-Petersen) approach for open reduction of a DDH, which structure is typically released at the pelvic brim rather than its insertion to protect the primary blood supply to the femoral head?
Explanation
Question 75
A 12-year-old premenarchal girl (Risser 0) is diagnosed with Adolescent Idiopathic Scoliosis. Her right thoracic curve measures 32 degrees. What is the most appropriate recommended management?
Explanation
Question 76
A 12-year-old boy weighing 55 kg (121 lbs) sustains a midshaft femur fracture. The plan is to proceed with antegrade rigid intramedullary nailing. Which entry point is recommended to minimize the risk of iatrogenic avascular necrosis (AVN) of the femoral head?
Explanation
Question 77
A 4-month-old female with developmental dysplasia of the hip (DDH) is being treated with a Pavlik harness. During a follow-up exam, she exhibits absent active knee extension on the treated side. What is the most likely cause of this finding?
Explanation
Question 78
A 13-year-old premenarchal girl presents with a right thoracic adolescent idiopathic scoliosis. Standing AP radiographs demonstrate a Cobb angle of 32 degrees. Her Risser stage is 1. What is the most appropriate management?
Explanation
Question 79
A 4-year-old boy is treated with a hip spica cast for a transverse midshaft femur fracture. Which of the following describes the expected maximum amount of femoral overgrowth and the typical timeframe it peaks following the injury?
Explanation
Question 80
An 18-month-old girl presents with a painless limp and delayed walking. Examination reveals asymmetric thigh folds and a positive Galeazzi sign. Radiographs confirm a unilateral dislocated hip. What is the most appropriate initial treatment?
Explanation
Question 81
A 2-year-old boy is evaluated for congenital scoliosis secondary to a fully segmented hemivertebra at T8. What screening studies are mandatory prior to definitive orthopedic management?
Explanation
Question 82
A 9-year-old girl weighing 48 kg (105 lbs) sustains a length-unstable, highly comminuted spiral fracture of the femoral shaft. Which of the following is the most appropriate surgical fixation method?
Explanation
Question 83
On an AP pelvis radiograph of a 6-month-old evaluated for DDH, the proximal femoral metaphysis is located in the upper outer quadrant formed by Hilgenreiner's and Perkin's lines. What does this radiographic finding indicate?
Explanation
Question 84
A 14-year-old boy with Duchenne muscular dystrophy presents with a progressive 55-degree thoracolumbar scoliosis. His forced vital capacity (FVC) is 40% of predicted. What is the recommended management?
Explanation
Question 85
A 7-month-old infant is brought to the emergency department with a spiral midshaft femur fracture. The parents state the child rolled off a low couch. What is the most appropriate next step in management?
Explanation
Question 86
An ultrasound of a 6-week-old infant's hip reveals a rounded bony promontory, an alpha angle of 48 degrees, and a beta angle of 60 degrees. According to the Graf classification, what is the best description of this hip?
Explanation
Question 87
In the Lenke classification for Adolescent Idiopathic Scoliosis, what radiographic criterion defines a "structural" minor curve that must be included in the operative fusion construct?
Explanation
Question 88
You are performing retrograde titanium elastic nailing for a pediatric femur fracture. To achieve optimal three-point fixation and biomechanical stability, how should the nails be contoured and positioned within the canal?
Explanation
Question 89
What is the most critical technical risk factor for the development of iatrogenic avascular necrosis (AVN) of the femoral head during closed reduction and spica casting for DDH?
Explanation
Question 90
A 6-month-old boy has a left-sided infantile idiopathic scoliosis with a Cobb angle of 35 degrees. The Rib-Vertebral Angle Difference (RVAD) of Mehta is measured at 25 degrees. What is the most likely natural history of this curve without treatment?
Explanation
None
