Spine Surgery Board Review MCQs (Set 2): Spinal Trauma & Degenerative Conditions | AAOS & ABOS
Key Takeaway
This high-yield question set for the AAOS and ABOS Spine Surgery Board Review (Set 2) focuses on critical topics like spinal trauma, including fractures and dislocations, as well as the diagnosis and management of degenerative spine conditions such as lumbar stenosis and disc disease. Prepare effectively for your exams.
Spine Surgery Board Review MCQs (Set 2): Spinal Trauma & Degenerative Conditions | AAOS & ABOS
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
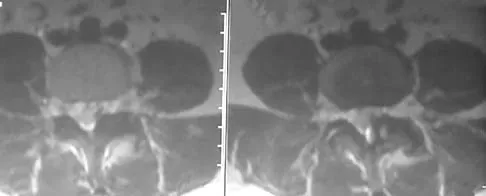
Figure 10 shows the MRI scan of a 56-year-old woman with metastatic breast cancer who now reports progressive paraparesis. Her general health remains good. Treatment should consist of
Explanation
Question 2
When 6 weeks of noninvasive nonsurgical management fails to provide relief for a lumbar disk herniation, a trial of epidural steroid injections is likely to yield which of the following results?
Explanation
Question 3
Which of the following anatomic changes is observed as part of the normal aging process of the adult spine?
Explanation
Question 4
A previously healthy 30-year-old woman has neck pain and bilateral hand and lower extremity tingling with weakness after falling down stairs. She is alert and oriented. Examination reveals incomplete quadriplegia at the C6 level that remains unchanged throughout her evaluation and initial treatment. Radiographs show a bilateral facet dislocation of C6 on C7 without fracture. Attempts at reduction with halo cervical traction up to her body weight are unsuccessful. What is the next most appropriate step?
Explanation
Question 5
Which of the following findings is the best radiographic indicator of segmental instability at L4-L5?
Explanation
Question 6
In a patient who has undergone fusion with instrumentation from T4 to the sacrum for adult scoliosis, at which site is a pseudarthrosis most likely to be discovered?
Explanation
Question 7
The afferent pain innervation of the L3-L4 facet joint arises from the medial branch nerve of
Explanation
Question 8
When posterior fusion with instrumentation to the sacrum is used to treat adult scoliosis, what instrumentation technique best increases the chance of a successful lumbosacral fusion?
Explanation
Question 9
Which of the following structures runs through the site indicated by the arrow in Figure 11?
Explanation
Question 10
A 42-year-old man has had left lower extremity pain in an L5 radicular pattern for the past 6 weeks. He denies significant axial low back pain. History reveals that he underwent an L4-5 diskectomy with successful relief of similar pain 5 years ago. Which of the following imaging studies would offer the greatest amount of information?
Explanation
Question 11
Figure 12 shows the radiograph of an 80-year-old woman who has had an 8-month history of back pain after a fall. What is the most likely diagnosis based on the radiographic findings at the fractured vertebrae?
Explanation
Question 12
Which of the following complications is uniquely associated with an anterior approach to the lumbosacral junction?
Explanation
Question 13
A 68-year-old woman with a history of rheumatoid arthritis has had neck pain and weakness in all four extremities that has become worse in the past 6 months. She has gone from a community to a household ambulator and uses a wheelchair outside of the home. Examination of the extremities reveals poor coordination, diffuse weakness, hyperactive reflexes, and bilateral sustained clonus. She has a broad-based and unsteady gait. The posterior atlanto-dens interval is 12 mm. Based on these findings and the radiograph and MRI scan shown in Figures 13a and 13b, the treatment of choice is surgical decompression and stabilization. However, the patient inquires about the prognosis with surgery compared to nonsurgical management. Assuming there are no complications from surgery, the patient should be informed that, with surgery, she will most likely
Explanation
Question 14
Five weeks after undergoing a successful L4-L5 diskectomy, with complete relief of his preoperative sciatica, a 36-year-old man has severe, relentless back and buttock pain. Examination and laboratory studies are unremarkable with the exception of an erythrocyte sedimentation rate (ESR) of 90 mm/h. What is the next most appropriate step in management?
Explanation
Question 15
An 18-year-old man sustained a knife injury to his midback, with the entry wound 2 cm to the left of the midline. He has been diagnosed with a hemicord transection. Neurologic examination will most likely reveal left-sided loss of
Explanation
Question 16
When using surgery extending to the pelvis to treat long spinal deformity in adults, the addition of anterior interbody structural support at the lumbosacral junction serves what biomechanical function?
Explanation
Question 17
A 40-year-old woman has had sciatic pain on the left side for the past 8 weeks. She reports that the pain radiates to her posterior thigh, lateral calf, and into the dorsum of her left foot. Neurologic examination shows weakness of the left extensor hallucis longus. Axial T2-weighted MRI scans through L4-L5 are shown in Figure 14. Management should consist of
Explanation
Question 18
During C1-C2 transarticular screw fixation, screw misplacement is most likely to result in injury to the
Explanation
Question 19
A 27-year-old professional soccer player sustained an injury to his cervical spine in a collision with another player. Initially he was diagnosed with a right C6 radiculopathy that resolved with rest, anti-inflammatory medications, and physical therapy. Following a fall in a game, he noted a recurrence of neck pain without radicular signs or symptoms. Additional nonsurgical management over the past few months has failed to provide relief. A cervical MRI scan shows a right-sided C5-6 herniation without any evidence of disk disease at other cervical levels. The patient desires to continue his career as a professional soccer player. What treatment offers the best long-term option for return to play?
Explanation
Question 20
A collegiate football player who sustained an injury to his neck has significant neck pain and weakness in his extremities. Following immobilization, which of the following steps should be taken prior to transport?
Explanation
Question 21
What is the most common complication following total disk arthroplasty in the lumbar spine?
Explanation
Question 22
A 42-year-old woman has cervical stenosis and radicular deficits at the C5-6 and C6-7 levels. History reveals that she has smoked one pack of cigarettes a day for 25 years. Because nonsurgical management has failed to provide relief, she is now seeking surgical treatment. After preoperative counseling, it becomes clear that she is not likely to stop smoking. Which of the following surgical procedures should be used?
Explanation
Question 23
An otherwise healthy 54-year-old man who underwent a successful multilevel lumbar decompression and fusion 4 years ago now reports increasingly severe bilateral thigh claudication with paresthesia and severe back pain for the past 12 months. Physical therapy, bracing, and epidural steroids have failed to provide relief. A radiograph and MRI scans are shown in Figures 15a through 15c. He is afebrile, and laboratory studies show an erythrocyte sedimentation rate of 5 mm/h and a normal WBC count. What is the best course of action?
Explanation
Question 24
Which of the following is considered a risk factor for the development of low back pain?
Explanation
Question 25
A corset-type brace may help reduce symptoms during an episode of acute low back pain as the result of
Explanation
Question 26
A 68-year-old man falls and strikes his chin, sustaining a hyperextension injury to his neck. He has severe weakness in his hands but can walk with assistance. Which of the following is the most likely diagnosis?
Explanation
Question 27
In evaluating a patient with a suspected L4-L5 far lateral (extraforaminal) disc herniation, which of the following physical examination findings is most likely expected?
Explanation
Question 28
A 72-year-old man presents with an acute Type II odontoid fracture following a fall. His fracture is posteriorly displaced by 6 mm.
Which of the following factors places him at the highest risk for nonunion with nonoperative management?

Explanation
Question 29
Which of the following represents the most common source of neurogenic claudication in patients older than 60 years?
Explanation
Question 30
A patient involved in a high-speed collision sustains a burst fracture of L1. On examination, he has loss of motor function, pain, and temperature sensation below the umbilicus, but retains proprioception and vibratory sense. This presentation is characteristic of which spinal cord syndrome?
Explanation
Question 31
According to the Thoracolumbar Injury Classification and Severity (TLICS) score, which of the following injury characteristics assigns the highest independent point value toward the decision for surgical intervention?
Explanation
Question 32
A 45-year-old man has a large sequestered (free fragment) disc herniation at L5-S1 causing severe S1 radiculopathy without motor deficit. What is the expected natural history of this specific type of disc herniation?
Explanation
Question 33
A 25-year-old man is brought to the ED after a lap-belt restrained motor vehicle collision. X-rays reveal a flexion-distraction injury (Chance fracture) at L2. Which of the following associated injuries must be actively ruled out?
Explanation
Question 34
An 80-year-old man with long-standing Ankylosing Spondylitis falls backwards, hitting his head. He reports severe neck pain but has a normal neurological examination. Initial cross-table lateral cervical X-rays are read as normal. What is the most appropriate next step in management?
Explanation
Question 35
A 55-year-old woman presents with progressive clumsiness in her hands and difficulty walking. Examination reveals a positive Hoffmann sign bilaterally, hyperreflexia in the lower extremities, and an inverted radial reflex. What is the most likely diagnosis?
Explanation
Question 36
A patient with a T4 spinal cord injury presents to the ER with a blood pressure of 80/50 mmHg and a heart rate of 50 bpm. His extremities are warm and well-perfused. What is the primary pathophysiologic mechanism for his hemodynamic state?
Explanation
Question 37
In a patient with traumatic spinal cord injury, the end of the "spinal shock" phase is clinically indicated by the return of which of the following?
Explanation
Question 38
A 45-year-old woman presents with severe, burning right anterior thigh pain and weakness in knee extension. Her symptoms began acutely after lifting a heavy box. Physical examination reveals a diminished right patellar reflex and a positive femoral stretch test. MRI of the lumbar spine demonstrates a far lateral (extraforaminal) disc herniation at the L3-L4 level. Which nerve root is most likely being compressed?
Explanation
Question 39
A 65-year-old man with a history of cervical spondylosis falls forward, striking his forehead. He presents to the emergency department with profound bilateral upper extremity weakness and relatively preserved lower extremity function. Sensation is decreased in a cape-like distribution over his shoulders. Following initial ATLS protocol, which of the following is the most critical medical management parameter for his spinal cord injury?
Explanation
Question 40
A 25-year-old man is brought to the trauma bay after a diving accident. He is awake, alert, and cooperative. Neurologic examination is entirely normal. Plain radiographs and CT scans demonstrate a unilateral C5-C6 facet dislocation with approximately 25% anterior translation of C5 on C6. What is the most appropriate next step in management?
Explanation
Question 41
An 82-year-old man with multiple medical comorbidities including severe COPD and ischemic heart disease falls from a standing height. CT of the cervical spine reveals a Type II odontoid fracture with 2 mm of posterior displacement. He is neurologically intact. What is the most appropriate definitive management?
Explanation
Question 42
An 18-year-old male is involved in a high-speed motor vehicle collision while wearing a lap belt. He complains of severe back pain. Radiographs demonstrate a horizontal fracture line passing through the spinous process, pedicles, and vertebral body of L2. Neurologic exam is normal. Which of the following is the most essential next step in his evaluation?
Explanation
Question 43
A 68-year-old woman presents with worsening back and bilateral leg pain that increases with walking and is relieved by leaning over a shopping cart. She has failed 6 months of non-operative management including physical therapy and epidural steroid injections. Imaging reveals an L4-L5 Grade 1 degenerative spondylolisthesis with severe central canal stenosis. Dynamic radiographs show 4 mm of translation. What is the most effective surgical treatment?
Explanation
Question 44
A 24-year-old male arrives in the emergency department after a motorcycle crash. He has a palpable step-off at the upper thoracic spine and is completely flaccid and areflexic below the T4 level. His heart rate is 50 beats/minute and his blood pressure is 80/50 mmHg. His extremities are warm and well-perfused. Which of the following best explains his hemodynamic parameters?
Explanation
Question 45
A 14-year-old female gymnast complains of insidious onset lower back pain that worsens with back extension. Neurologic examination is entirely normal. Radiographs reveal a pars interarticularis defect at L5 bilaterally with 15% translation of L5 on S1. What is the most appropriate initial management?
Explanation
Question 46
A 40-year-old man presents to the emergency department with severe lower back pain, bilateral lower extremity weakness, and new-onset urinary incontinence. Physical examination reveals perianal numbness and decreased bilateral Achilles reflexes. What is the most appropriate next step in management?
Explanation
Question 47
When evaluating an MRI of the cervical spine in a patient with severe cervical spondylotic myelopathy, which of the following intrinsic cord signal changes is associated with the poorest prognosis for neurologic recovery following surgical decompression?
Explanation
Question 48
A 55-year-old man with a known history of ankylosing spondylitis presents to the emergency department complaining of severe neck pain after a minor fall from a chair. He is neurologically intact. Standard anteroposterior and lateral cervical radiographs demonstrate osteopenia and syndesmophyte formation but no obvious fracture. What is the mandatory next step in his evaluation?
Explanation
Question 49
A traumatic spondylolisthesis of the axis, commonly known as a Hangman's fracture, involves bilateral fractures through which specific anatomic structure?
Explanation
Question 50
The Thoracolumbar Injury Classification and Severity (TLICS) score is used to guide the surgical management of thoracolumbar trauma. Which of the following is NOT one of the three main categories evaluated in the TLICS system?
Explanation
Question 51
A 65-year-old man is evaluated for mild mid-back stiffness. Radiographs reveal flowing ossification along the anterolateral aspect of the thoracic vertebrae with preservation of disc height and no evidence of sacroiliac joint erosions. To meet the Resnick diagnostic criteria for Diffuse Idiopathic Skeletal Hyperostosis (DISH), this flowing ossification must bridge at least how many contiguous vertebral bodies?
Explanation
Question 52
A 52-year-old woman presents with neck pain radiating down her left arm. Physical examination demonstrates weakness in elbow extension and wrist flexion, along with an absent triceps reflex. She reports numbness primarily in her long (middle) finger. Which cervical nerve root is most likely compressed?
Explanation
Question 53
A 60-year-old man with end-stage renal disease on hemodialysis presents with severe, unrelenting mid-back pain and fever. Laboratory tests show an ESR of 100 mm/h and a CRP of 50 mg/L. MRI of the spine with gadolinium reveals a dorsal epidural abscess causing moderate cord compression. What is the most common causative organism for this condition?
Explanation
Question 54
A 56-year-old woman with a history of metastatic breast cancer presents with progressive paraparesis and hyperreflexia in her lower extremities over the last 3 days. Her systemic disease is otherwise well-controlled, and her expected survival is greater than 1 year. MRI reveals a pathological fracture at T8 with high-grade epidural spinal cord compression caused by tumor mass. Based on the Patchell trial criteria, what is the most appropriate initial treatment?
Explanation
Question 55
A 30-year-old male is intubated following a high-speed motor vehicle collision. A trauma CT scan of the head and neck demonstrates a significantly increased basion-dens interval (>12 mm) and a Powers ratio greater than 1, diagnostic of atlanto-occipital dissociation (AOD). What is the definitive treatment for this highly unstable injury?
Explanation
Question 56
A 70-year-old man presents with bilateral upper extremity weakness (hands greater than shoulders) and mild lower extremity clumsiness after a hyperextension injury during a fall.
What is the most appropriate initial hemodynamic management for this patient?

Explanation
Question 57
A 35-year-old man falls from a roof, sustaining an L1 burst fracture. His neurological examination is completely intact. MRI demonstrates an intact posterior ligamentous complex (PLC). The fracture exhibits 15 degrees of local kyphosis. Based on the Thoracolumbar Injury Classification and Severity (TLICS) score, what is the recommended management?
Explanation
Question 58
Which of the following preoperative factors is the most reliable negative prognostic indicator for postoperative neurological recovery in a patient undergoing surgical decompression for degenerative cervical spondylotic myelopathy?
Explanation
Question 59
An 82-year-old man sustains a Type II odontoid fracture after a ground-level fall. He is neurologically intact. Which of the following stabilization methods is associated with the highest risk of severe morbidity and mortality in this specific patient population?
Explanation
Question 60
A 65-year-old woman presents with severe neurogenic claudication and low back pain. Radiographs demonstrate a Grade I L4-L5 degenerative spondylolisthesis that increases to Grade II on dynamic flexion films. What is the most appropriate surgical intervention if a 6-month trial of conservative management fails?
Explanation
Question 61
A 22-year-old restrained passenger in a high-speed motor vehicle collision sustains a flexion-distraction (Chance) fracture of L2. Due to the mechanism of this injury, which of the following associated injuries must be aggressively ruled out?
Explanation
Question 62
A patient sustains a traumatic spondylolisthesis of the axis (Hangman's fracture). Imaging demonstrates severe angulation with minimal translation, consistent with a Levine-Edwards Type IIA fracture. Which of the following management steps is strictly contraindicated?
Explanation
Question 63
A 30-year-old man presents neurologically intact but with severe neck pain following a football tackle. CT demonstrates a unilateral C5-C6 facet dislocation. He is awake, cooperative, and able to follow commands perfectly. What is the next most appropriate step in management?
Explanation
Question 64
A 60-year-old man with a 30-year history of ankylosing spondylitis presents with new-onset mechanical neck pain after a minor fall from a chair. Initial plain radiographs of the cervical spine are read as normal. His neurological exam is intact. What is the most appropriate next step?
Explanation
Question 65
A 45-year-old man presents with right arm pain and weakness following a weightlifting injury. Examination reveals a diminished brachioradialis reflex, weakness in wrist extension, and numbness over the dorsal web space of the thumb and index finger. Which cervical nerve root is most likely compressed?
Explanation
Question 66
A 50-year-old man presents with severe left-sided anterior thigh pain. Examination reveals profound weakness in left knee extension and a diminished left patellar reflex. Sensation is decreased over the medial aspect of the leg. MRI demonstrates a far lateral (extraforaminal) disc herniation. At which level is this herniation most likely located?
Explanation
Question 67
According to the Denis classification of sacral fractures, fractures involving Zone III are most highly associated with which of the following clinical complications?
Explanation
Question 68
An 82-year-old woman falls from a standing height and presents with severe neck pain. Radiographs reveal a Type II odontoid fracture with 3 mm of posterior displacement. She has a history of severe COPD and ischemic heart disease. What is the most appropriate non-operative management for this patient?
Explanation
Question 69
A 65-year-old man sustains a hyperextension injury to his cervical spine during a motor vehicle collision. On examination, he has motor weakness in all four extremities, but his upper extremities (especially the hands) are significantly weaker than his lower extremities. What is the typical pattern of functional recovery in this syndrome?
Explanation
Question 70
A 70-year-old man presents with bilateral leg pain and fatigue that worsens after walking two blocks. Which of the following clinical findings most reliably differentiates neurogenic claudication from vascular claudication?
Explanation
Question 71
A 55-year-old man presents with difficulty buttoning his shirts and a wide-based, unsteady gait. Physical examination reveals a positive Hoffmann's sign. Which of the following additional physical examination findings is most specific for this patient's underlying condition?
Explanation
Question 72
A 25-year-old woman involved in a high-speed motor vehicle collision presents with a transverse ecchymosis across her abdomen (seatbelt sign). Radiographs reveal an osseous flexion-distraction injury (Chance fracture) of L2. What associated injury must be most urgently and specifically ruled out?
Explanation
Question 73
A 65-year-old woman with L4-L5 degenerative spondylolisthesis and severe spinal stenosis has failed six months of conservative management. She complains of severe neurogenic claudication and mechanical back pain. What is the most appropriate surgical treatment?
Explanation
Question 74
A 30-year-old man falls from a ladder and sustains a traumatic fracture of the L1 vertebra. According to the Denis three-column classification system, which of the following features defines a burst fracture and differentiates it from a simple compression fracture?
Explanation
Question 75
A 22-year-old man presents with severe neck pain after a rugby tackle. Radiographs reveal a unilateral facet dislocation at C5-C6. What is the classic mechanism of injury responsible for this specific pathology?
Explanation
Question 76
A 60-year-old man with a known history of advanced ankylosing spondylitis presents to the emergency department complaining of new, severe neck pain after tripping and falling onto a carpeted floor. Initial plain radiographs of the cervical spine are interpreted as negative. What is the most appropriate next step in management?
Explanation
Question 77
A 45-year-old man presents with acute onset right leg pain that radiates down the lateral aspect of his calf to the dorsum of his foot. MRI reveals a large paracentral disc herniation at the L4-L5 level. Which nerve root is most likely compressed, and what is the expected motor deficit?
Explanation
Question 78
An 8-year-old boy is brought to the ED after a motor vehicle collision. He had transient numbness and weakness in both legs that has since resolved. Plain radiographs and a non-contrast CT of the spine are completely normal. What is the diagnostic modality of choice to fully evaluate this clinical picture?
Explanation
Question 79
A 62-year-old woman underwent an L4-S1 posterior spinal instrumented fusion 5 years ago. She now presents with new-onset radicular leg pain and progressive low back pain. Radiographs show significant degenerative changes and stenosis at the L3-L4 level. Which biomechanical factor is the primary contributor to this new pathology?
Explanation
Question 80
A 45-year-old man with a history of chronic low back pain suddenly develops severe bilateral sciatica, saddle anesthesia, and urinary retention. Physical examination reveals decreased rectal tone. What is the most critical and definitive step in his management?
Explanation
Question 81
A 28-year-old unrestrained driver is involved in a head-on collision. Radiographs demonstrate bilateral fractures through the pars interarticularis of the C2 vertebra with mild anterior subluxation of C2 on C3. What is the classic mechanism of injury for this specific fracture pattern?
Explanation
Question 82
A 35-year-old pedestrian is struck by a vehicle and sustains a severe traumatic brain injury. Lateral cervical spine radiographs demonstrate a basion-dental interval (BDI) of 14 mm. Which of the following initial stabilization techniques is strictly contraindicated in this patient?
Explanation
Question 83
A 68-year-old man presents with a 2-year history of bilateral buttock and leg pain that worsens with walking and standing. He reports that leaning forward on a shopping cart relieves his symptoms. Which of the following physical examination findings is most likely to be present in this patient?
Explanation
Question 84
A 72-year-old man presents with severe neck pain following a ground-level fall. CT imaging reveals a Type II odontoid fracture with 6 mm of posterior displacement. He is neurologically intact. Which of the following factors is most strongly predictive of nonunion if this patient is treated conservatively with a halo vest?
Explanation
Question 85
A 45-year-old construction worker falls 15 feet, sustaining a T12 burst fracture. He remains neurologically intact. Which of the following radiographic findings is the most reliable indicator of a concurrent posterior ligamentous complex (PLC) injury?
Explanation
Question 86
A 65-year-old man with known advanced cervical spondylosis is involved in a motor vehicle collision. He presents with severe motor weakness in his upper extremities but is able to move his lower extremities against resistance. He also has decreased sensation over the cape-like distribution of his shoulders. What is the most likely diagnosis?
Explanation
None
