Pediatric Ankle Pain: Diagnosis Involves the Subtalar Joint
Key Takeaway
Here are the crucial details you must know about Pediatric Ankle Pain: Diagnosis Involves the Subtalar Joint. Talocalcaneal coalition is a fibrous, cartilaginous, or bony connection between the talus and calcaneus, causing vague, deep medial ankle discomfort. Prevalent in adolescents (12-16 years) due to segmentation failure, it commonly involves of the subtalar joint, leading to limited motion. This condition can present with a lump under the medial malleolus and potentially a valgus hindfoot.
A 14-year-old male presents with persistent medial hindfoot pain and a rigid flatfoot. He has failed 6 months of non-operative management, including orthotics and physical therapy. You suspect a talocalcaneal (TC) coalition. What radiographic signs would you look for on plain film, and what is the next definitive imaging step?
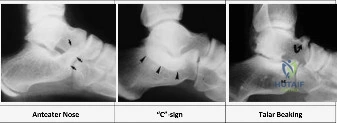
Candidate: I would order weight-bearing foot and ankle X-rays. I’d look for the "C-sign" on the lateral view and perhaps some talar beaking. For definitive imaging, I would order a CT scan of the hindfoot.
Failing to mention the specifics of the CT scan. A failing candidate often omits the necessity of coronal slices perpendicular to the posterior facet, which are essential for calculating the percentage of joint involvement—the key decision point for surgery vs. fusion.
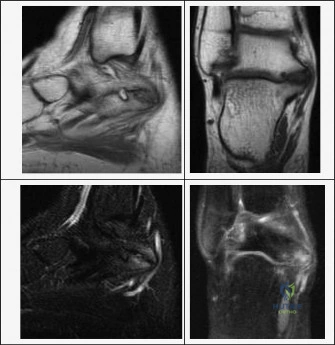
I would perform weight-bearing radiographs: the "C-sign" (continuity of the talar dome and sustentaculum tali) is highly specific for TC coalition. I would also assess for talar beaking (a traction osteophyte). The gold standard for definitive planning is a CT scan. I specifically require coronal slices perpendicular to the posterior facet to measure the surface area of the coalition. If the coalition involves >50% of the posterior facet, resection is contraindicated, and I would instead discuss subtalar arthrodesis.
You are performing a resection of a calcaneonavicular coalition. Please describe your surgical approach and the specific steps taken to prevent recurrence.

Candidate: I would use a lateral Ollier incision. I would reflect the EDB muscle and resect the bony bar between the calcaneus and navicular. Finally, I would interpose fat or muscle to stop it from growing back.
Ignoring the "medial extent" of the resection. A common error is incomplete medial resection, leaving part of the coalition near the talar head, which guarantees recurrence. Candidates often forget to mention protecting the intermediate dorsal cutaneous and sural nerves.
I utilize an Ollier incision, identifying and protecting the intermediate dorsal cutaneous and sural nerves. I elevate the Extensor Digitorum Brevis (EDB) from its calcaneal origin, tagging it for later use. I then perform a generous rectangular resection of the coalition; it is critical to extend the resection medially all the way to the talar head, as incomplete medial resection is the primary cause of failure. Finally, I interpose the EDB muscle belly into the defect and secure it to the medial soft tissues to prevent bone regrowth.
During the medial approach for a talocalcaneal coalition resection, you are dissecting toward the sustentaculum tali. What anatomical structures must you protect, and what is your specific strategy for ensuring restoration of motion?
Candidate: I would retract the posterior tibial tendon and protect the neurovascular bundle. I would then resect the middle facet bar until I see the posterior facet cartilage.
Failing to mention the "release" test. A high-scoring candidate must describe the manual inversion/eversion of the heel to confirm the "sudden release" of motion, which is the intraoperative feedback that resection is complete.
The dissection follows an internervous plane between the posterior tibial tendon (retracted superiorly) and the flexor digitorum longus (retracted inferiorly). The posterior tibial neurovascular bundle lies posterior/inferior to the FDL and requires meticulous protection. The coalition is excised starting from the anterior facet toward the posterior facet. The endpoint is confirmed by manual inversion and eversion of the heel; a palpable "release" of the hindfoot indicates complete excision. I then apply bone wax to the cancellous surfaces and pack the defect with a free fat graft to prevent recurrence.
