Pediatric Lateral Condyle Fracture: The Critical Role of Internal Oblique Radiographs
Key Takeaway
The internal oblique radiograph is crucial for diagnosing pediatric lateral condyle fractures because standard AP/lateral views often obscure subtle displacement or articular involvement due to developing ossification centers. This specialized view clearly delineates the fracture line, extent of displacement, rotation, and articular surface involvement, enabling accurate Salter-Harris classification and guiding optimal management decisions.
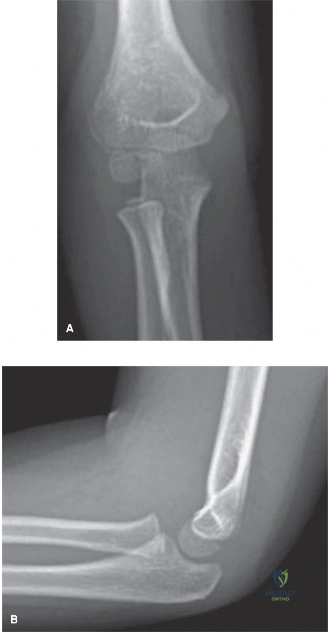
You are presented with a 7-year-old child following a fall from a height. You suspect a lateral condyle fracture. Looking at these initial radiographs, what is your systematic approach to assessing the injury, and what additional views—if any—would you order to guide your management?
Candidate: I would assess the radiographs for signs of a lateral condyle fracture, specifically looking at the capitellum and lateral metaphysis. I’d look for an anterior fat pad sign on the lateral view. Because standard views can be deceptive due to the cartilaginous nature of the fragment, I would order an internal oblique view to better define the fracture line and degree of displacement.
The candidate fails to mention the "hinge" concept or the importance of the internal oblique view specifically for evaluating the articular surface. They often focus on the humerus broadly rather than specifically assessing the capitellar physis and the trochlear groove displacement.
Systematically evaluate: 1. Presence of effusion (anterior fat pad). 2. Cortical step-off at the lateral metaphysis. 3. Integrity of the articular surface. The internal oblique view is mandatory to profile the lateral condyle, removing the radial head superimposition. Mention that standard views underestimate displacement because the majority of the fragment is radiolucent cartilage; thus, an internal oblique view is essential to determine if the fracture is >2mm or has hinge disruption.
The internal oblique view confirms a Jakob Stage 3 fracture. Discuss your surgical decision-making and the specific anatomical structures you must protect to avoid long-term complications.

Candidate: Jakob Stage 3 signifies complete displacement and rotation, which is an indication for ORIF. I would use a lateral approach, avoiding posterior dissection to preserve the blood supply to the capitellum, which enters posteriorly.
Candidates often suggest aggressive dissection to "see the whole fracture." Failing to warn against stripping the posterior soft tissues is a major red flag, as this directly leads to AVN/fishtail deformity.
Identify: 1. Jakob Stage 3 requires ORIF to restore articular congruity. 2. Approach: Kocher interval (between anconeus and ECU). 3. Critical technical point: Protect the posterior soft tissue hinge to avoid devascularizing the capitellum. 4. Fixation: Divergent K-wires or screws (if avoiding physis) to ensure stability. 5. Emphasize that active-only ROM post-op is critical to prevent myositis ossificans.
You have treated the fracture with ORIF and K-wires. At the 6-month follow-up, the parents are worried about a prominent lump on the lateral aspect of the elbow, but the child is asymptomatic. How do you manage this?
Candidate: This is likely lateral spurring or overgrowth. I would reassure the parents that this is a common sequela, occurring in up to 70% of cases, and is generally benign if the child has full range of motion.
Suggesting immediate surgical excision of the spur. This is a common but unnecessary procedure; most spurs remodel or remain asymptomatic, and surgery risks further stiffness.
Diagnose as "Lateral Spurring" (overgrowth). Explain it is due to periosteal stripping/hyperemia. Management is observation and reassurance. Only consider excision if symptomatic (nerve irritation) or cosmetically unacceptable after a prolonged period of failed conservative management.
