
Comprehensive Introduction and Patho-Epidemiology
Pediatric elbow fractures represent one of the most critical and technically demanding domains within pediatric orthopedic trauma. These injuries require a profound understanding of evolving skeletal anatomy, nuanced radiographic interpretation, and meticulous surgical execution. Mismanagement can lead to devastating complications, including Volkmann ischemic contracture, permanent neurologic deficits, and severe angular deformities such as cubitus varus. As a highly respected academic orthopedic surgeon, it is imperative to approach these fractures with a rigorous, evidence-based algorithm. Elbow fractures account for approximately 8% to 9% of all upper extremity fractures in the pediatric population, making them a staple of emergency orthopedic consultations.
The distal humerus is the epicenter of pediatric elbow trauma, accounting for a staggering 85% of all elbow fractures. Within this anatomical subset, supracondylar humerus fractures dominate the clinical landscape, comprising 55% to 75% of distal humerus injuries. The peak incidence of these fractures occurs in children between 5 and 10 years of age. During this specific developmental window, the supracondylar region undergoes significant bony remodeling, resulting in a decreased anteroposterior (AP) diameter that acts as a structural stress riser. Furthermore, boys are disproportionately affected compared to girls, often presenting with higher-energy mechanisms.
A distinct seasonal distribution characterizes the epidemiology of pediatric elbow fractures. Incidence rates surge during the summer months, directly correlating with increased outdoor activities, playground use (particularly monkey bars), and trampoline-related trauma. Conversely, the winter months see a nadir in these specific fracture patterns, though snow-related sports can still contribute to the overall volume. Understanding these epidemiological trends is crucial for anticipating emergency department volume and ensuring adequate resource allocation during peak trauma seasons.
The pathophysiology of these injuries is intimately tied to the mechanism of injury and the inherent ligamentous laxity present in young children. Extension-type injuries account for 98% of supracondylar fractures and are classically the result of a fall onto an outstretched hand (FOOSH) with the elbow in full extension. In this position, the olecranon process forcefully engages the olecranon fossa, acting as a bony fulcrum that levers the distal humerus anteriorly, causing catastrophic failure of the anterior cortex while the posterior periosteal hinge typically remains intact.
Epidemiology of Pediatric Elbow Trauma
The demographic distribution of pediatric elbow fractures provides critical insight into injury mechanisms and preventative strategies. The male-to-female ratio for supracondylar fractures is approximately 3:2. This discrepancy is often attributed to differing play patterns and risk-taking behaviors, though the gap narrows in older pediatric cohorts. The non-dominant extremity is significantly more likely to sustain a fracture, as children reflexively use their non-dominant arm to break a fall while protecting their dominant side.
As children age out of the 5-to-8-year-old high-risk window, the structural integrity of the distal humerus matures, and the pattern of elbow trauma shifts. In older children and adolescents, supracondylar fractures become less common, superseded by elbow dislocations, medial epicondyle avulsions, and radial neck fractures. This epidemiological shift underscores the importance of correlating the patient's chronological and skeletal age with the expected injury pattern during the initial clinical assessment.
Socioeconomic and regional variations also play a subtle but measurable role in the epidemiology of pediatric elbow trauma. Urban environments with high-density playgrounds see localized spikes in supracondylar fractures, whereas rural settings may present with higher-energy mechanisms involving motorized vehicles or agricultural equipment. These higher-energy mechanisms are more frequently associated with open fractures, severe comminution, and concomitant neurovascular injuries, necessitating a heightened index of suspicion upon presentation.
Delayed presentations, while less common in modern healthcare systems, still occur and dramatically alter the epidemiological outcomes. A fracture that presents days after the initial injury is often complicated by profound soft tissue swelling, organizing hematoma, and early callus formation, rendering closed reduction exponentially more difficult. Recognizing the epidemiological factors that contribute to delayed presentation—such as lack of access to immediate care—is vital for the treating surgeon when formulating a preoperative plan.
Pathophysiology of Supracondylar Fractures
The mechanical failure of the distal humerus under axial and rotational loads is a fascinating study in pediatric biomechanics. In an extension-type supracondylar fracture, the anterior capsule of the elbow—which is thicker and stronger than the posterior capsule—becomes violently taut. This tension, combined with the bony impingement of the olecranon in the olecranon fossa, creates a massive bending moment across the thinned supracondylar metaphysis. The bone fails in tension anteriorly, propagating posteriorly.
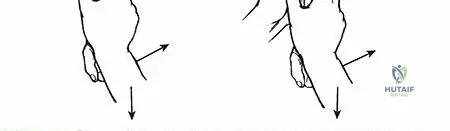
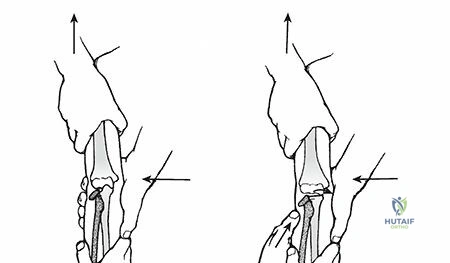
The concept of the periosteal hinge is paramount to the closed management of these fractures. In extension-type injuries, the posterior periosteum usually remains intact, tethering the proximal and distal fragments. This intact posterior hinge is the surgeon's greatest ally during closed reduction, allowing the distal fragment to be manipulated and "locked" into place via elbow flexion. The direction of displacement is heavily influenced by the position of the hand at the moment of impact. If the hand is pronated, the distal fragment typically displaces posteromedially; if supinated, it displaces posterolaterally.
Flexion-type supracondylar fractures, comprising a mere 2% of these injuries, possess a fundamentally different pathophysiology. These result from direct trauma to the posterior aspect of a flexed elbow or a fall directly onto the olecranon. The mechanical force drives the distal fragment anteriorly, rupturing the posterior periosteum while the anterior periosteal hinge may remain intact. This reversal of the periosteal hinge mechanics completely alters the reduction maneuver, requiring extension rather than flexion to achieve and maintain stability.
The rotational instability inherent in completely displaced (Type III) supracondylar fractures adds a complex dimension to the pathophysiology. The distal fragment not only extends and translates but also rotates horizontally. The medial column often collapses, leading to internal rotation of the distal fragment. If this rotational malalignment is not recognized and meticulously corrected during surgery, the intact anterior periosteum will heal asymmetrically, inevitably leading to the classic "gunstock deformity" or cubitus varus.
Detailed Surgical Anatomy and Biomechanics
The pediatric elbow is a highly complex, tri-articulate hinge joint comprising the ulnohumeral, radiocapitellar, and proximal radioulnar articulations. Mastery of this regional anatomy is non-negotiable for the orthopedic surgeon. The distal humerus possesses a unique geometry; the articulating surfaces of the capitellum and trochlea project distally and anteriorly at an angle of approximately 30 to 45 degrees relative to the humeral shaft. This anterior angulation is critical for allowing full elbow flexion without impingement of the coronoid process against the anterior humeral cortex.
The center of rotation of the articular surface of each condyle lies on the exact same horizontal axis. Consequently, any malalignment of the condylar relationships—whether through a supracondylar fracture, a lateral condyle fracture, or a transphyseal separation—alters their respective arcs of rotation. This biomechanical disruption severely limits both flexion and extension and can lead to early post-traumatic arthrosis. Furthermore, the elbow accounts for only 20% of the longitudinal growth of the upper extremity, meaning that remodeling potential for angular deformities is exceptionally poor, placing a premium on anatomic reduction.
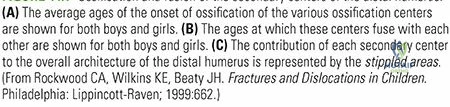
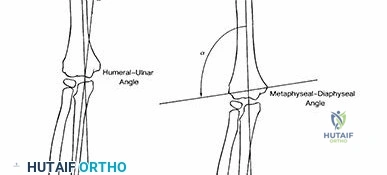
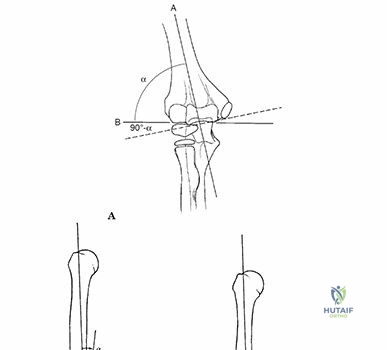
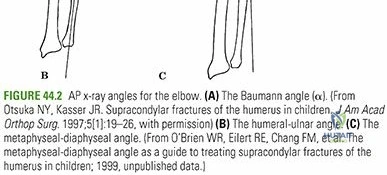
The carrying angle of the elbow is heavily influenced by the obliquity of the distal humeral physis. In a normal pediatric population, this angle averages 6 degrees of valgus in girls and 5 degrees in boys. In addition to the anterior angulation, there is a natural horizontal rotation of the humeral condyles in relation to the diaphysis, with the lateral condyle rotated approximately 5 degrees medially. In the setting of a displaced supracondylar fracture, this medial rotation is often significantly exacerbated, serving as the primary biomechanical driver for post-traumatic cubitus varus.
Osteology and Articular Relationships
The osteology of the distal humerus is characterized by two distinct columns—the medial and lateral columns—that diverge from the diaphysis to support the articular segment. Between these columns lies the coronoid fossa anteriorly and the olecranon fossa posteriorly. The bone separating these two fossae is paper-thin, sometimes even completely absent (forming a supratrochlear foramen). This structural void creates a significant mechanical weak point, precisely where supracondylar fractures propagate.
The articular cartilage in the pediatric elbow is exceptionally thick, rendering much of the joint radiolucent on standard radiographs. This necessitates a reliance on secondary ossification centers and subtle radiographic lines to infer the alignment of the cartilaginous anlage. The "teardrop" is a critical radiographic shadow seen on a true lateral radiograph. It is formed by the posterior margin of the coronoid fossa anteriorly, the anterior margin of the olecranon fossa posteriorly, and the superior margin of the capitellar ossification center inferiorly. Disruption of the teardrop indicates a fracture through the supracondylar region.
The ligamentous stabilizers of the pediatric elbow include the medial collateral ligament (MCL) complex and the lateral collateral ligament (LCL) complex. In children, these ligaments are biomechanically stronger than the adjacent physes and metaphyseal bone. Therefore, forces that would typically cause an elbow dislocation or ligamentous rupture in an adult will instead result in a supracondylar fracture or an avulsion fracture of the epicondyles in a child.
The proximal radioulnar joint and the radiocapitellar joint must act in perfect synchrony to allow for pronation and supination. The radial head must point directly at the capitellum in all radiographic views. Any disruption of this relationship, such as in a Monteggia fracture-dislocation or a missed radial neck fracture, will result in profound functional deficits, highlighting the need to evaluate the entire forearm and wrist during the assessment of pediatric elbow trauma.
Vascular Anatomy and Perfusion Networks
The vascular supply to the pediatric elbow is a robust, broad anastomotic network comprising both intraosseous and extraosseous blood supplies. This redundancy is generally protective against ischemia; however, specific anatomic quirks render certain regions highly vulnerable. The brachial artery, the primary axial vessel, courses anteriorly over the brachialis muscle and is tightly tethered by the bicipital aponeurosis (lacertus fibrosus). In a severely displaced extension-type supracondylar fracture, the proximal humeral shaft is driven anteriorly, impaling or tenting the brachial artery, leading to immediate vascular compromise.
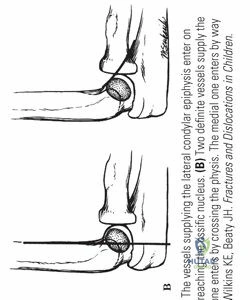
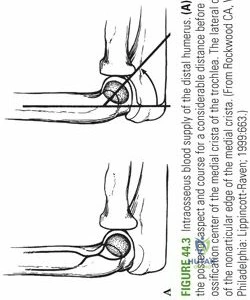
The intraosseous vascularity of the distal humerus is of paramount surgical importance. The capitellum is primarily supplied by a posterior branch of the brachial artery that enters the bone along the lateral crista. This distinct blood supply makes the capitellum relatively resistant to avascular necrosis (AVN) following supracondylar fractures, provided the lateral column is not aggressively stripped of its soft tissue envelope during open reduction.
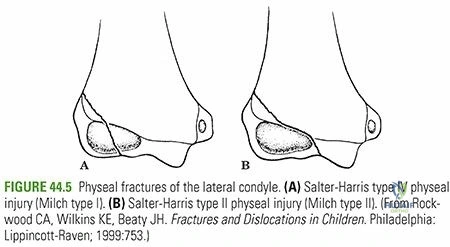
Conversely, the trochlea has a much more precarious blood supply. It is perfused by a medial branch that enters along the nonarticular medial crista and a lateral branch that crosses the physis. Crucially, there is no anastomotic connection between these two vessels within the trochlea itself. This end-arterial watershed physiology makes the trochlea highly susceptible to AVN, particularly following fractures of the lateral condyle or aggressive surgical dissection of the medial column.
Understanding this vascular anatomy is critical when planning surgical approaches. Medial approaches must respect the medial epicondylar vessels, while lateral approaches must preserve the posterior vascular tether to the capitellum. Iatrogenic disruption of these delicate networks can result in partial or complete physeal arrest, fishtail deformity of the distal humerus, and progressive angular deformity that is exceptionally difficult to salvage.
Ossification Centers and Developmental Milestones
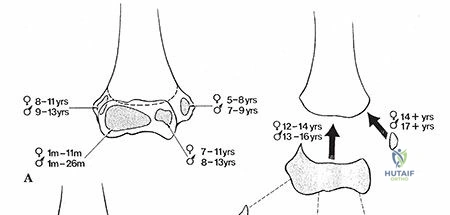
The pediatric elbow is a dynamic radiographic landscape, with secondary ossification centers appearing and fusing in a highly predictable, sequential manner. Mastery of these milestones is essential to differentiate true fractures from normal developmental variants. With the exception of the capitellum, these ossification centers appear approximately two years earlier in girls than in boys. The widely accepted mnemonic for the appearance of these centers is CRMTOL.
- Capitellum: Appears at 1 year.
- Radial Head: Appears at 3 years.
- Medial Epicondyle: Appears at 5 years.
- Trochlea: Appears at 7 years.
- Olecranon: Appears at 9 years.
- Lateral Epicondyle: Appears at 11 years.

The sequence of appearance is more reliable than the exact chronologic age. This sequential rule is an invaluable diagnostic tool. For instance, if a radiograph of a 6-year-old child shows an ossified trochlea but an "absent" medial epicondyle, the surgeon must immediately suspect that the medial epicondyle has been avulsed and is incarcerated within the ulnohumeral joint. Failure to recognize this pattern will result in a missed diagnosis, rapid joint destruction, and severe ulnar neuropathy.
Pseudofractures of the ossification centers are a common pitfall for the uninitiated. The trochlea, in particular, frequently ossifies from multiple distinct foci, giving it a fragmented, irregular appearance that perfectly mimics a comminuted fracture. Similarly, the lateral epicondyle can appear as a thin, wispy flake of bone before fully consolidating. When in doubt, obtaining comparison radiographs of the uninjured contralateral elbow is the gold standard for distinguishing a developmental variant from acute trauma.
Furthermore, the fusion of these centers dictates the timing of skeletal maturity at the elbow. The lateral epicondyle, capitellum, and trochlea fuse together to form a single conjoint epiphysis before ultimately fusing to the humeral metaphysis around age 14 to 16. The medial epicondyle is the last center to fuse to the shaft, often remaining open until age 15 to 18. This prolonged vulnerability explains why medial epicondyle avulsions remain common well into adolescence.
Exhaustive Indications and Contraindications
The management of pediatric supracondylar humerus fractures is dictated by the modified Gartland classification system, which categorizes fractures based on the degree of displacement and the integrity of the periosteal hinges. Decision-making must be swift, precise, and tailored to the individual fracture personality. While non-operative management has a distinct role, the threshold for surgical intervention in modern pediatric orthopedics is appropriately low to prevent the devastating sequelae of malunion and neurovascular compromise.
Gartland Type I fractures are truly nondisplaced and are universally treated with non-operative immobilization. Gartland Type II fractures are displaced but maintain an intact posterior cortex (in extension types). The treatment of Type II fractures is nuanced; Type IIa fractures (minimal angulation, no rotational deformity, anterior humeral line intersects the anterior capitellum) may be managed non-operatively with close radiographic follow-up. However, Type IIb fractures (rotational deformity, anterior humeral line misses the capit
Clinical & Radiographic Imaging Archive





Detailed Chapters & Topics
Dive deeper into specialized chapters regarding pediatric-elbow-fractures-and-dislocations