Effective Fixation of Pediatric T-Condylar Fractures for Best Outcomes
Key Takeaway
Your ultimate guide to Effective Fixation of Pediatric T-Condylar Fractures for Best Outcomes starts here. Fixation of pediatric T-condylar fractures typically involves closed reduction and pinning for younger children. Older children and adolescents often require an open approach with internal fixation. This can include intercondylar screw compression and K-wire fixation, or an olecranon osteotomy for comminuted fractures, ensuring anatomic reduction to restore elbow function.
Introduction and Epidemiology
T-condylar fractures of the distal humerus in the pediatric and adolescent populations represent a complex and relatively rare orthopedic challenge. Epidemiological data suggest that these injuries account for approximately 2% of all pediatric elbow fractures. Unlike the more ubiquitous supracondylar humerus fractures, which typically occur in younger children following low-energy falls, T-condylar fractures are generally the result of higher-energy mechanisms and present more frequently in older children and adolescents approaching skeletal maturity.
The pathomechanics of this injury involve the olecranon acting as a wedge during severe hyperextension or direct axial loading of the flexed elbow. This mechanical wedge effect drives the proximal ulna into the trochlear groove, creating a classic Y-shaped or T-shaped fracture pattern with the epicenter of energy dissipation located within the olecranon fossa.
While these fractures are less likely to exhibit the severe comminution frequently encountered in adult intra-articular distal humerus fractures, the presence of a coronal split or significant articular displacement demands meticulous surgical attention. In younger children with highly compliant bone and thick periosteal sleeves, an acceptable result can occasionally be obtained with closed reduction and percutaneous pinning. However, this is generally not as straightforward as in a standard supracondylar humerus fracture. Older children and young adolescents almost universally require an open approach to restore articular congruity and establish stable fixation that permits early range of motion.
Surgical Anatomy and Biomechanics
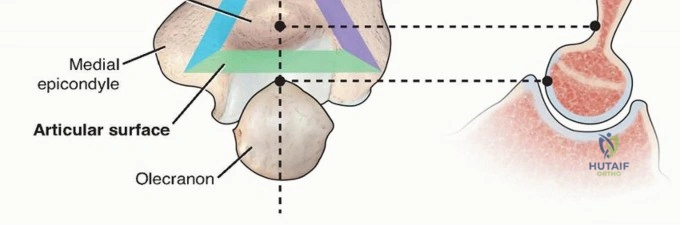
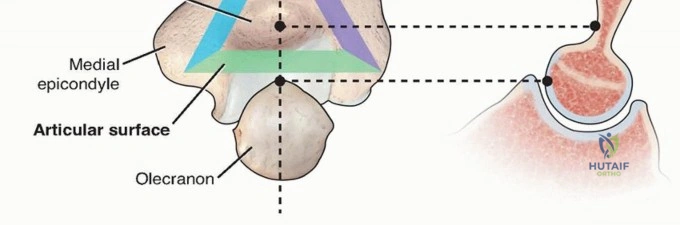
A profound understanding of distal humeral anatomy is requisite for the successful reconstruction of T-condylar fractures. The distal humerus is a complex, multi-axial articulation that functions mechanically as a hinge connecting the arm to the forearm. Conceptually, the distal humerus is composed of a medial column and a lateral column, which are connected distally by the articular block (the middle hinge).
This architectural configuration creates a "triangle of stability." The medial column diverges from the diaphyseal axis at approximately 45 degrees and terminates at the medial epicondyle. The lateral column diverges at approximately 20 degrees, ending at the lateral epicondyle and capitellum. The structural integrity of this triangle must be anatomically restored to withstand the significant torsional and bending moments applied across the elbow joint during physiologic loading.
The ulnohumeral articulation is the primary joint that must be reconstructed in a T-condylar fracture to restore the hinge mechanism of the elbow. The trochlea, which articulates with the greater sigmoid notch of the ulna, is highly congruent and unforgiving of step-offs or gap deformities. Occasionally, the radiocapitellar joint is also compromised by a concomitant coronal shear fracture of the capitellum.
Neurovascular proximity dictates surgical strategy. The ulnar nerve courses posterior to the medial epicondyle within the cubital tunnel and is at high risk during both the initial trauma and subsequent medial surgical exposures. The radial nerve crosses the lateral column proximally, dictating the proximal extent of lateral plate fixation. Blood supply to the trochlea is predominantly endosteal, making it susceptible to avascular necrosis if excessive soft tissue stripping is performed during open reduction.
Indications and Contraindications
The management of pediatric T-condylar fractures hinges on the degree of displacement, articular involvement, and the skeletal maturity of the patient. Non-operative management is exceedingly rare and reserved strictly for truly non-displaced fractures where the articular congruity is perfectly maintained, and the columns are stable.

Surgical intervention is the gold standard for the vast majority of these injuries. The primary goal is anatomical restoration of the articular surface followed by rigid fixation of the articular block to the humeral metaphysis. Contraindications to immediate internal fixation include severe, life-threatening polytrauma requiring damage control orthopedics, active soft tissue infection at the surgical site, or severe burn injuries precluding safe surgical incisions.
| Indication Category | Operative Management | Non Operative Management |
|---|---|---|
| Displacement | > 2 mm articular step-off or gap | Truly non-displaced (< 1 mm) |
| Stability | Columnar instability / gross motion | Stable to varus/valgus stress |
| Soft Tissue | Open fractures, vascular compromise | Intact skin, no impending compartment syndrome |
| Patient Age | Adolescents nearing skeletal maturity | Very young children (rarely, if non-displaced) |
| Polytrauma | Floating elbow, concomitant injuries | Isolated injury in a compliant patient |

Pre Operative Planning and Patient Positioning
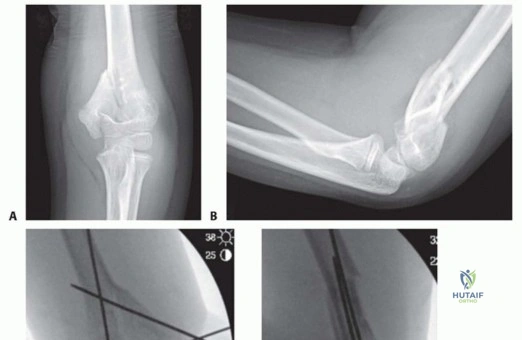
Thorough preoperative planning is critical for optimizing surgical outcomes and minimizing intraoperative delays. Standard anteroposterior and true lateral radiographs of the elbow are mandatory. However, due to the complex overlapping anatomy of the distal humerus, plain radiography often underestimates the degree of articular comminution.
A preoperative computed tomography (CT) scan with 3D reconstructions is highly recommended for all displaced T-condylar fractures. CT imaging delineates the exact fracture pattern, identifies coronal shear components, and allows the surgeon to template screw trajectories for the articular block. Furthermore, the remainder of the limb should be carefully examined. Coexisting wrist fractures or forearm injuries can drastically increase the risk of compartment syndrome and complicate soft tissue management. Fracture blisters resulting from severe soft tissue injury must be identified, as their presence may dictate the timing and placement of surgical incisions.

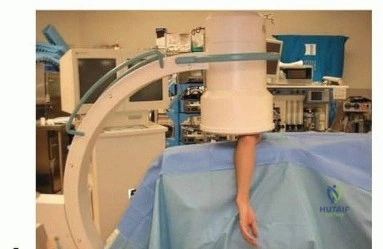
Patient positioning depends on the chosen surgical approach and surgeon preference. The lateral decubitus position with the arm draped over a radiolucent post is widely favored. This allows for excellent posterior access to the elbow, utilizes gravity to assist with elbow flexion, and provides unimpeded access for the C-arm fluoroscope. Alternatively, the prone position can be utilized, offering similar posterior access, though airway management and anesthesia access are more complex. A sterile tourniquet is typically applied high on the brachium to provide a bloodless surgical field during the critical phases of articular reduction.
Detailed Surgical Approach and Technique
The surgical management of pediatric T-condylar fractures requires a methodical, stepwise approach to restore the triangle of stability. The technique chosen must balance the need for adequate visualization against the morbidity of extensive soft tissue dissection.
Closed Reduction and Percutaneous Pinning
In select cases involving younger children with minimal comminution and highly stable fracture patterns, closed reduction and percutaneous pinning (CRPP) may be attempted. This involves longitudinal traction, correction of coronal and sagittal alignment, and percutaneous stabilization using smooth Kirschner wires (K-wires). However, achieving and maintaining anatomic articular reduction closed is notoriously difficult. If fluoroscopy reveals any residual articular step-off, the surgeon must immediately convert to an open approach.

Surgical Approaches
For older children and adolescents, an open approach is mandatory. The choice of approach is dictated by the level of comminution and the required visualization.
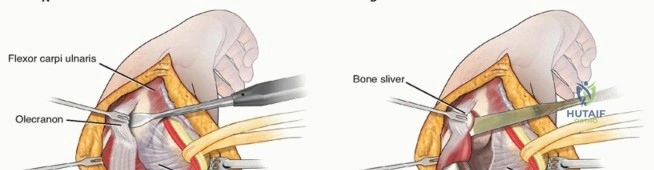
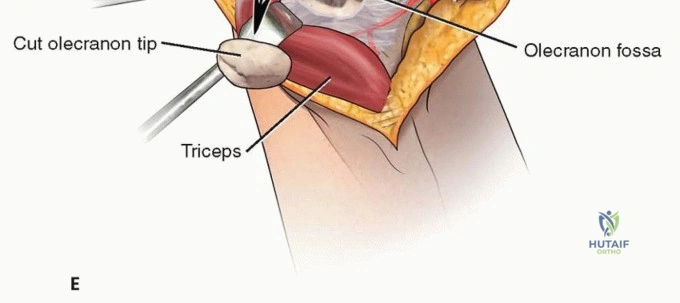
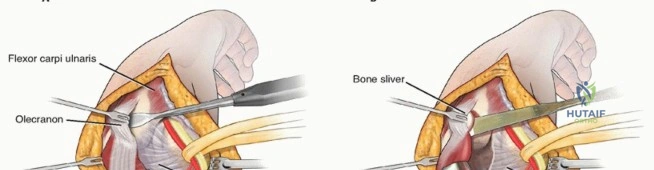
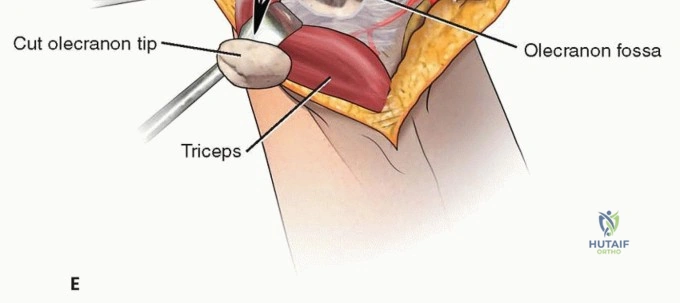
Olecranon Osteotomy: Historically, an intra-articular chevron olecranon osteotomy was the standard for visualizing the distal humeral articular surface. While it provides unparalleled exposure of the trochlea, it carries inherent risks in the pediatric population, including osteotomy nonunion, hardware prominence, and growth arrest if the proximal ulnar physis is violated. Therefore, in pediatric patients, it is reserved for cases with severe intra-articular comminution where visualization is otherwise impossible.
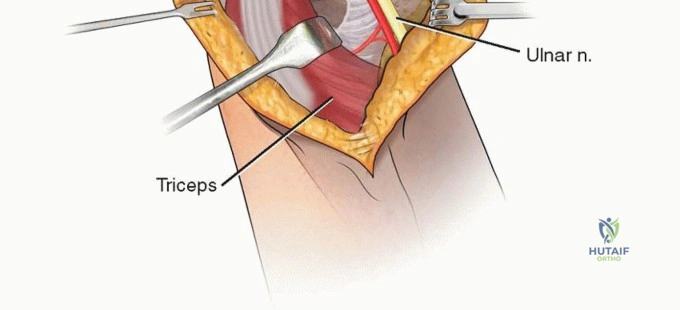
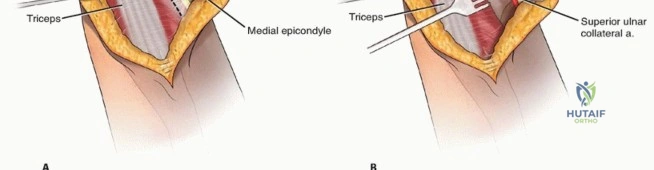
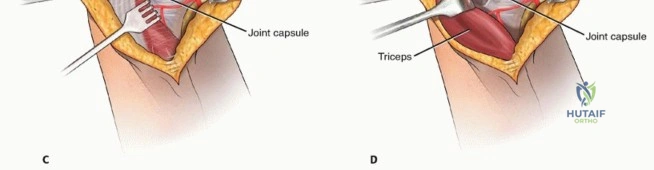
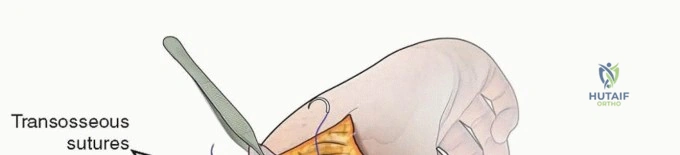
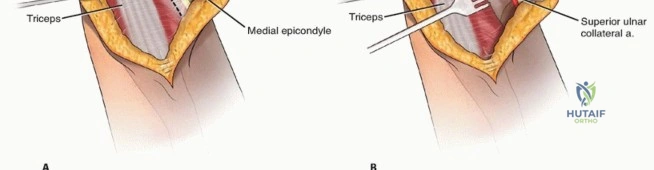
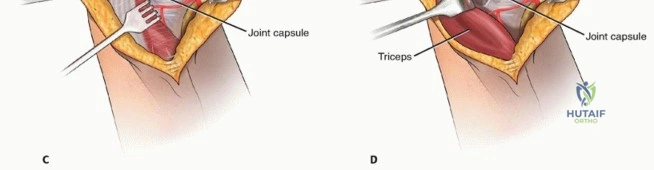
Morrey Slide Approach: Because pediatric fractures are generally less comminuted than adult fractures, they frequently do not require a full osteotomy. The Morrey slide (triceps-reflecting) approach is highly advantageous in this demographic. Originally described to avoid olecranon osteotomies in cases where total elbow arthroplasty would be a salvage operation, it has immense utility in adolescent trauma. The triceps and ulnar periosteum are elevated off the ulna medially, maintaining continuity with the forearm fascia. This provides excellent visualization of the joint to facilitate anatomic reduction while preserving the extensor mechanism and avoiding the complications of an osteotomy.

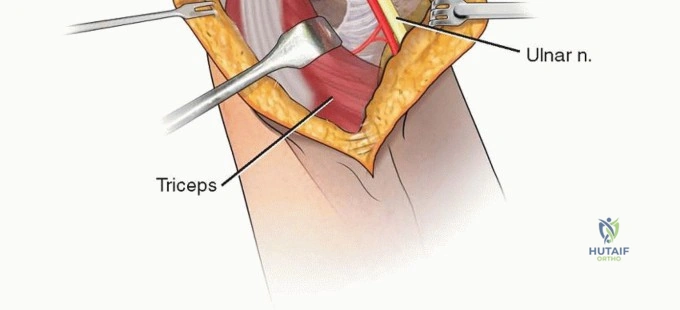
Ulnar Nerve Management
Regardless of the posterior approach utilized, the ulnar nerve must be identified, neurolysed, and protected early in the procedure. The nerve is located in the cubital tunnel posterior to the medial epicondyle. Whether to perform an in situ decompression or an anterior transposition remains a topic of surgical debate. Transposition is generally indicated if the medial hardware placement will irritate the nerve in its native bed, or if significant medial column comminution requires extensive dissection.
Fracture Reduction and Fixation Sequence
The fundamental principle of T-condylar fracture fixation is to convert the complex intra-articular fracture into a simpler extra-articular fracture.
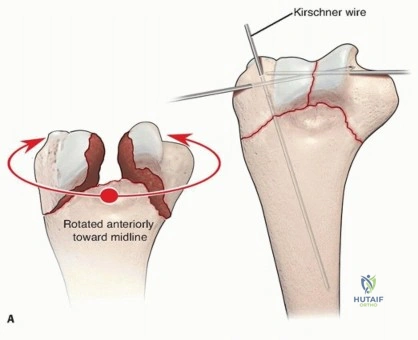
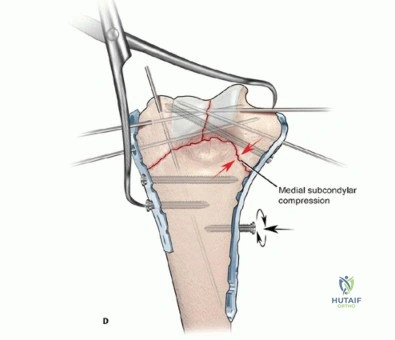
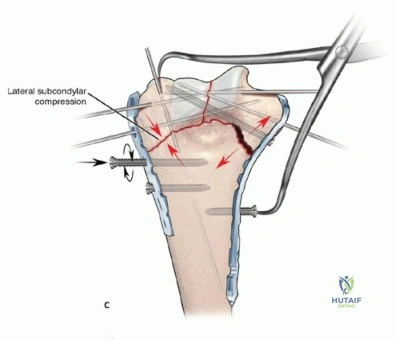
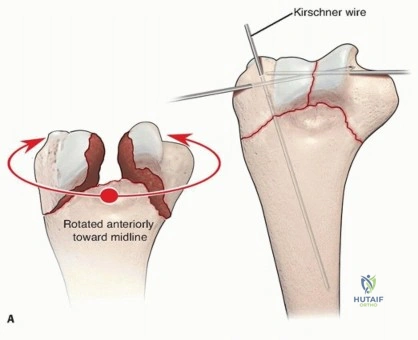
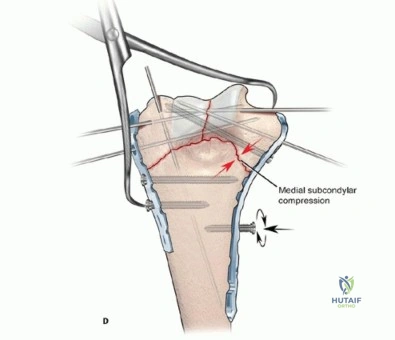
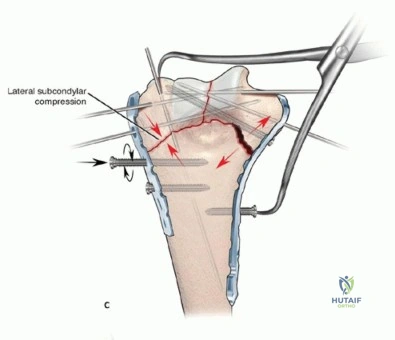
- Articular Reconstruction: The first step is the anatomical reduction of the trochlea and capitellum. The articular fragments are meticulously cleaned of hematoma and interposed periosteum. They are reduced using pointed reduction forceps and provisionally stabilized with smooth K-wires. Definitive fixation of the articular block is achieved using intercondylar compression screws (typically 2.5 mm, 3.0 mm, or 3.5 mm headless compression screws or partially threaded cancellous screws). The screw trajectory must be carefully planned to avoid violating the olecranon or coronoid fossae, which would mechanically block elbow motion.
- Metaphyseal Attachment: Once the articular block is reconstructed, it is reduced to the humeral shaft. In younger children with robust periosteum, crossed K-wires or a combination of K-wires and a single column plate may provide sufficient stability.

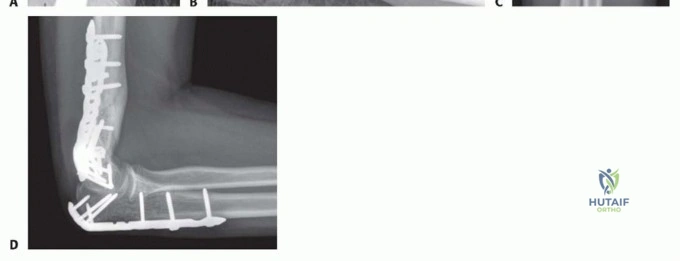
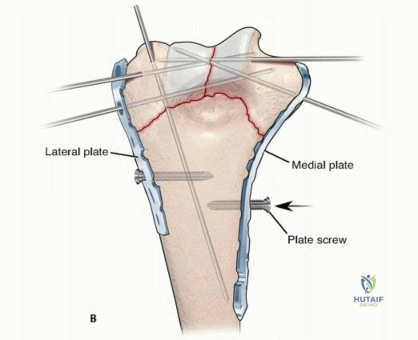
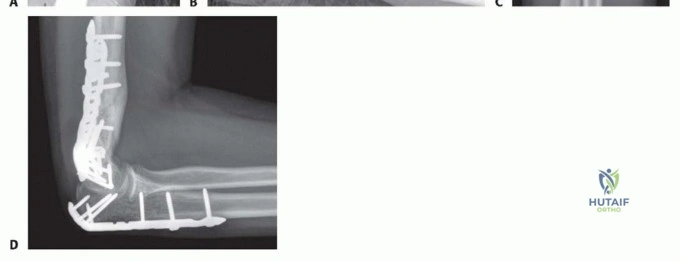
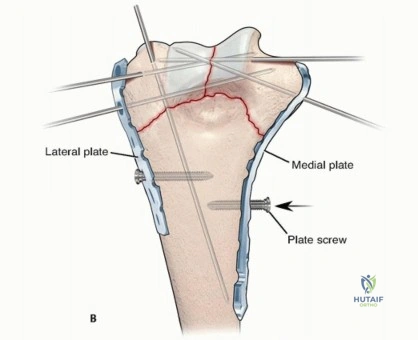
- Columnar Plating: In older adolescents, rigid internal fixation with dual plating is required. Plates are typically applied in either an orthogonal configuration (one medial, one posterolateral) or a parallel configuration (medial and lateral). Biomechanical studies suggest parallel plating may offer superior resistance to torsional forces, but orthogonal plating is often more anatomically accommodating to the distal humerus. Pediatric-specific locking plates or contoured reconstruction plates are utilized. The plates must be dynamically compressed to the shaft, and locking screws should be utilized in the articular block to prevent secondary loss of reduction.

Complications and Management
The surgical management of pediatric T-condylar fractures is fraught with potential complications. The high-energy nature of the injury combined with the complex anatomy of the elbow makes perfect outcomes challenging to achieve consistently.
Elbow stiffness is the most ubiquitous complication. The elbow joint capsule is highly reactive to trauma and surgical dissection, rapidly forming dense scar tissue. Loss of terminal extension is common, though usually functionally well-tolerated. Severe stiffness (arc of motion less than 100 degrees) significantly impairs activities of daily living.
Malunion, particularly cubitus varus resulting from inadequate medial column reduction or collapse, alters the mechanical axis of the upper extremity. While often considered a cosmetic deformity, severe cubitus varus can lead to tardy ulnar nerve palsy or posterolateral rotatory instability later in life.
| Complication | Estimated Incidence | Prevention and Salvage Strategies |
|---|---|---|
| Elbow Stiffness | 15% - 30% | Rigid fixation allowing early ROM; static progressive splinting; late capsular release. |
| Ulnar Neuropathy | 5% - 10% | Careful identification and protection; anterior transposition if hardware impinges; post-op neurolysis. |
| Malunion (Varus/Valgus) | 5% - 15% | Anatomic reduction; rigid dual plating; corrective osteotomy for severe symptomatic deformity. |
| Heterotopic Ossification | 3% - 8% | Gentle soft tissue handling; avoid aggressive passive stretching; NSAID prophylaxis in high-risk cases. |
| Avascular Necrosis | < 5% | Minimize stripping of the posterior trochlea; preserve extraosseous vascular sling. |
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is entirely dependent on the rigidity of the intraoperative fixation. The overarching goal is to initiate motion as early as possible to mitigate capsular contracture while protecting the healing osteosynthesis construct.
If rigid dual plating is achieved in an adolescent, the elbow is typically immobilized in a posterior splint at 60 to 90 degrees of flexion for only 7 to 10 days to allow for initial soft tissue and incisional healing. Following this brief period of immobilization, active and active-assisted range of motion exercises are initiated under the guidance of a physical therapist. Passive stretching is strictly avoided in the early phases, as it provokes an inflammatory response, exacerbates capsular scarring, and increases the risk of heterotopic ossification.
In younger children where fixation relies heavily on K-wires, a longer period of immobilization is required. The elbow is casted or splinted for 3 to 4 weeks until radiographic evidence of early callus formation is visible. At that point, the K-wires are removed in the clinic or operating room, and motion is initiated.
Hardware removal of plates and screws is generally not indicated unless the implants become prominent and symptomatic, or if they are situated in a location that tethers physeal growth in a younger child. If hardware removal is necessary, it is typically delayed until at least 6 to 12 months postoperatively to ensure complete bony consolidation.
Summary of Key Literature and Guidelines
Current academic literature emphasizes that the treatment of pediatric T-condylar fractures must be highly individualized based on the patient's physiological age and the specific fracture morphology. While closed reduction and pinning remain a viable option in the pre-adolescent population with simple fracture patterns, there is a clear paradigm shift toward open reduction and rigid internal fixation in adolescents.
Studies comparing surgical approaches consistently demonstrate that triceps-sparing or triceps-reflecting approaches (such as the Morrey slide) yield equivalent articular visualization to olecranon osteotomies in pediatric patients, but with a significantly lower complication profile. The avoidance of iatrogenic physeal injury to the proximal ulna and the elimination of osteotomy-related hardware complications make these soft-tissue approaches highly preferable.

Furthermore, biomechanical analyses of fixation constructs in the distal humerus support the use of parallel or orthogonal plating over isolated screw or wire fixation in adolescents approaching adult body habitus. The literature underscores that the primary determinant of a successful outcome is the achievement of absolute articular congruity and sufficient construct stability to permit early, active rehabilitation, thereby minimizing the functionally devastating complication of elbow stiffness.
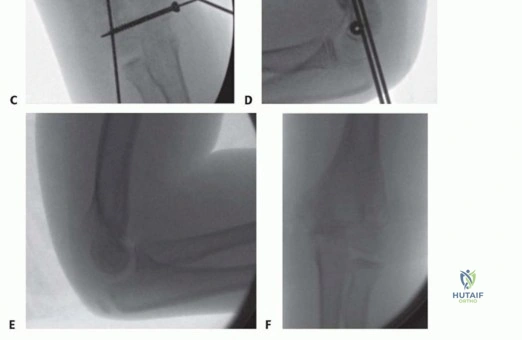
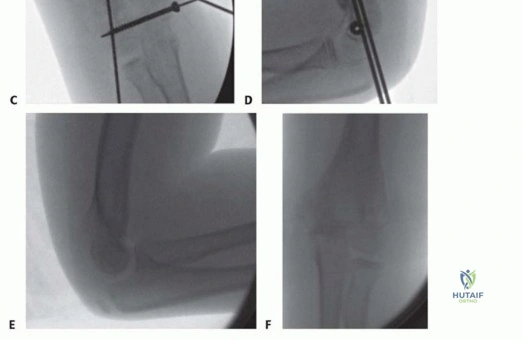
Clinical & Radiographic Imaging