Masterclass in Pediatric Radial Head and Neck Fractures: Operative Orthopaedics
Key Takeaway
Pediatric radial neck fractures primarily affect children aged 4 to 14 years, typically occurring through the metaphysis or physis (Salter-Harris types I, II, or IV). Management depends on the degree of angulation. While angulation under 30 to 45 degrees is often managed non-operatively, severe displacement requires closed reduction, percutaneous leverage, intramedullary pinning (Metaizeau technique), or open reduction to restore radiocapitellar alignment and preserve forearm rotation.
Comprehensive Introduction and Patho-Epidemiology
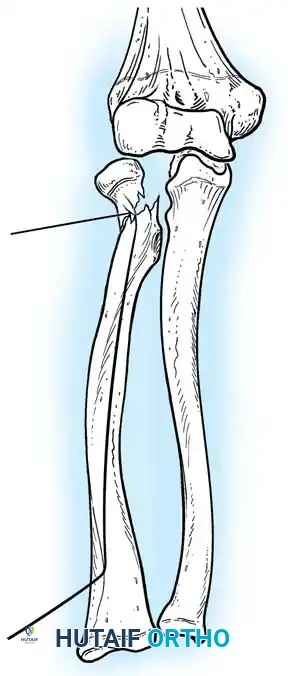
Pediatric radial neck fractures represent a distinct, highly nuanced biomechanical and anatomical challenge in the realm of orthopedic traumatology. Unlike the adult population, in whom fractures of the radial head predominate due to the structural rigidity of the fully ossified proximal radius, the pediatric demographic predominantly sustains fractures through the metaphyseal neck. These injuries most frequently occur in children between the ages of 4 and 14 years, with a peak incidence around 9 to 10 years of age. This specific demographic distribution is primarily dictated by the unique ossification timeline of the proximal radius. The secondary center of ossification for the radial head typically does not commence radiographic appearance until approximately 5 years of age. Consequently, the predominantly cartilaginous radial head is highly resilient, capable of absorbing and dissipating significant traumatic forces, thereby transferring the kinetic energy to the adjacent metaphyseal neck, which acts as the structural weak point during valgus loading.
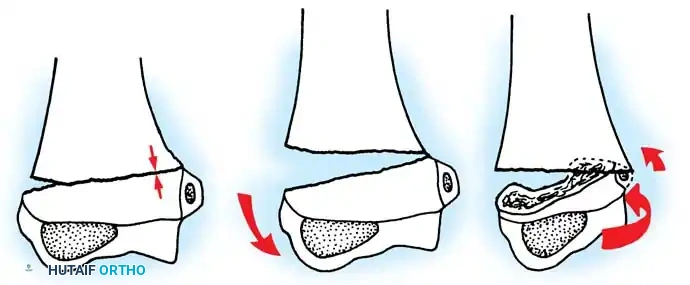
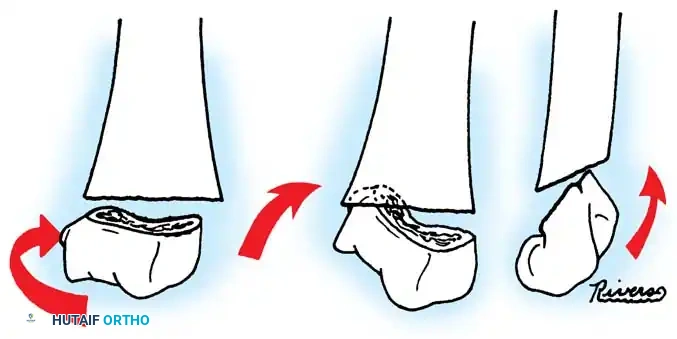
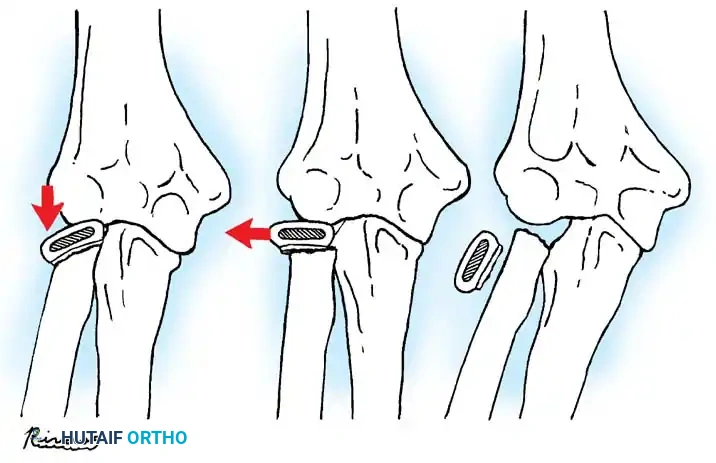
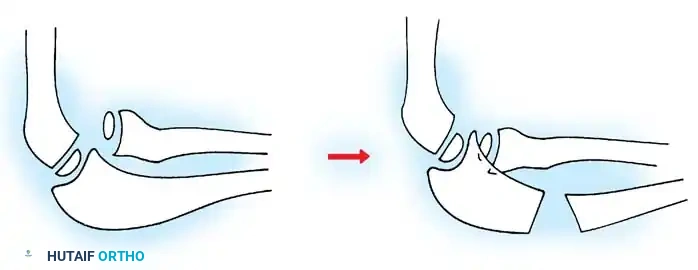
The predominant mechanism of injury involves a fall onto an outstretched hand (FOOSH) with the elbow in full extension and the forearm in supination. As the axial load is transmitted through the forearm, a profound valgus thrust is generated across the elbow joint. This forces the radial head to impact violently against the capitellum. Because the cartilaginous radial head is compressible, the shearing and compressive forces are concentrated at the subcapital physis or the metaphysis, resulting in a fracture. In more severe trauma, this mechanism can be accompanied by a transient or complete elbow dislocation, leading to complex fracture-dislocation patterns where the radial head may become incarcerated within the joint space, acting as an absolute mechanical block to reduction. Furthermore, the energy transfer may result in concomitant injuries, such as medial epicondyle avulsion fractures, olecranon fractures, or medial collateral ligament (MCL) ruptures, which drastically complicate the clinical picture and alter the therapeutic algorithm.

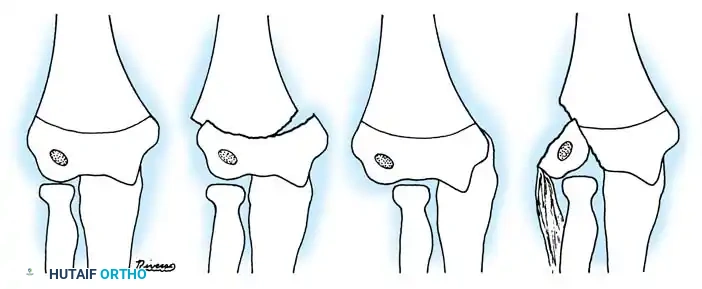
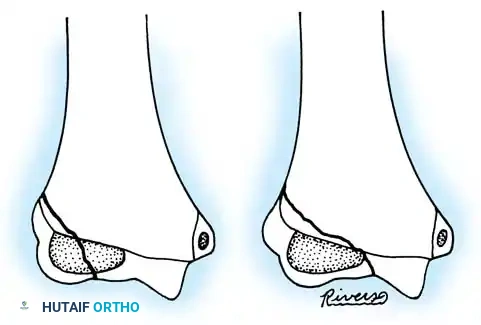
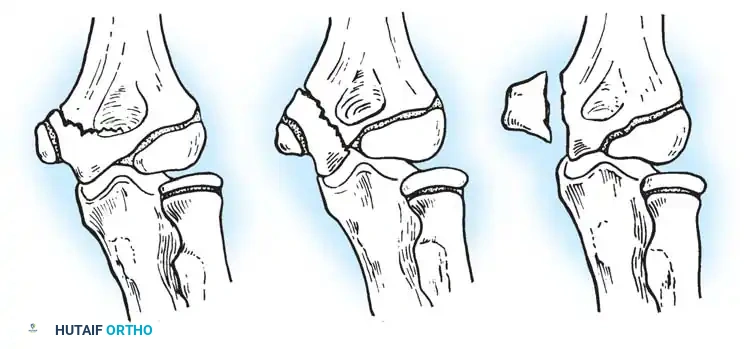
Historically, the classification of these injuries has been a subject of considerable debate, with numerous systems proposed by Vostal, Newman, O’Brien, and Jeffery. However, in contemporary academic and clinical practice, the Wilkins Classification system stands as the definitive gold standard for categorizing pediatric radial neck fractures and guiding surgical decision-making. The Wilkins system elegantly synthesizes the morphological descriptions of Jeffery and Newman, categorizing fractures based on their anatomical location, physeal involvement, and association with elbow dislocations. Type A injuries encompass Salter-Harris type I and II fractures of the proximal radial epiphysis, while Type B denotes Salter-Harris type IV injuries. Type C is reserved for fractures exclusively involving the proximal radial metaphysis. Types D and E are particularly critical for the operative surgeon, describing fractures that occur iatrogenically during the reduction of a dislocated elbow, or those occurring simultaneously with the dislocation, respectively.
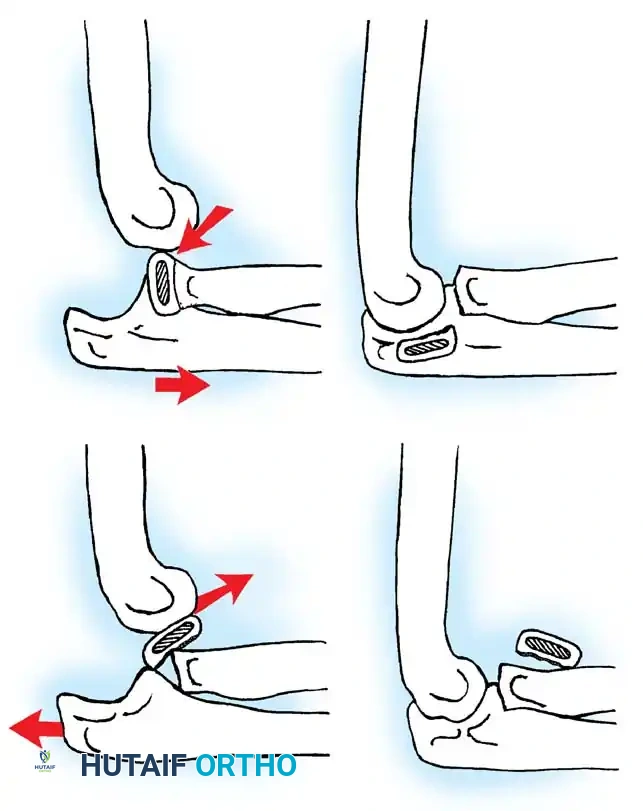
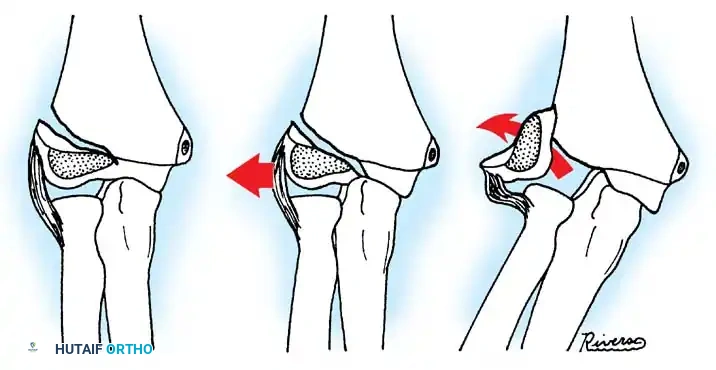
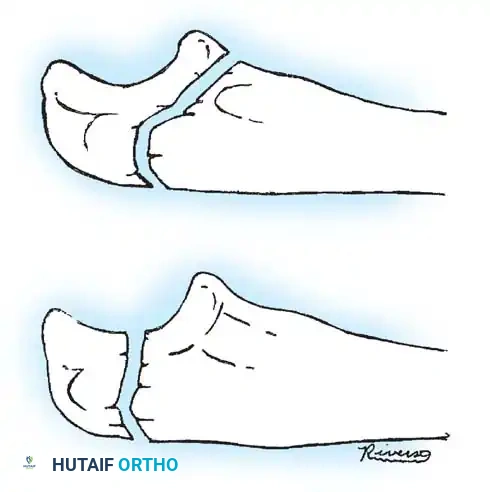
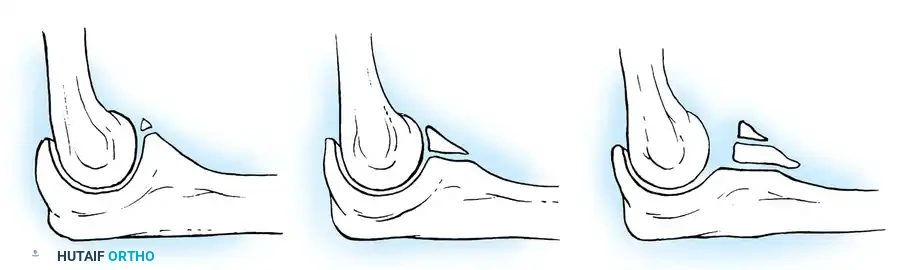
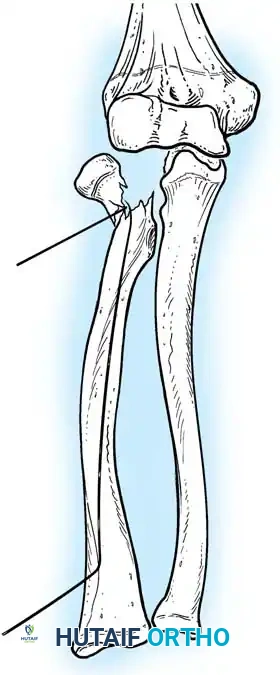
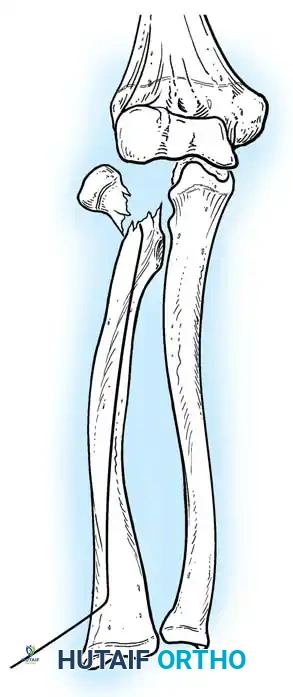
Understanding the patho-epidemiology and precise classification of these fractures is paramount for anticipating the trajectory of displacement and the propensity for spontaneous reduction versus mechanical locking. Fractures can present across a spectrum of displacement: from simple angulation, to translocation (translational shift), to complete displacement where the proximal fragment loses all soft tissue tethering. In the context of an elbow dislocation (Wilkins Type E), the completely displaced proximal fragment is at exceptionally high risk for avascular necrosis due to the catastrophic disruption of its delicate vascular supply. The surgeon must approach these high-energy variants with a high index of suspicion for compartment syndrome, neurovascular compromise, and the imminent need for urgent surgical intervention to restore joint congruity and preserve the viability of the radial head.
Detailed Surgical Anatomy and Biomechanics
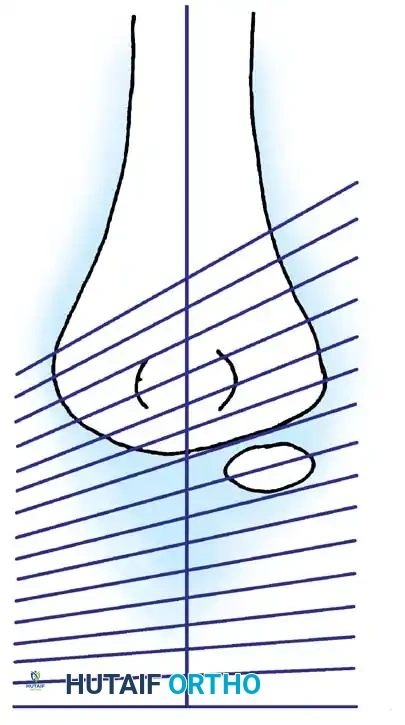
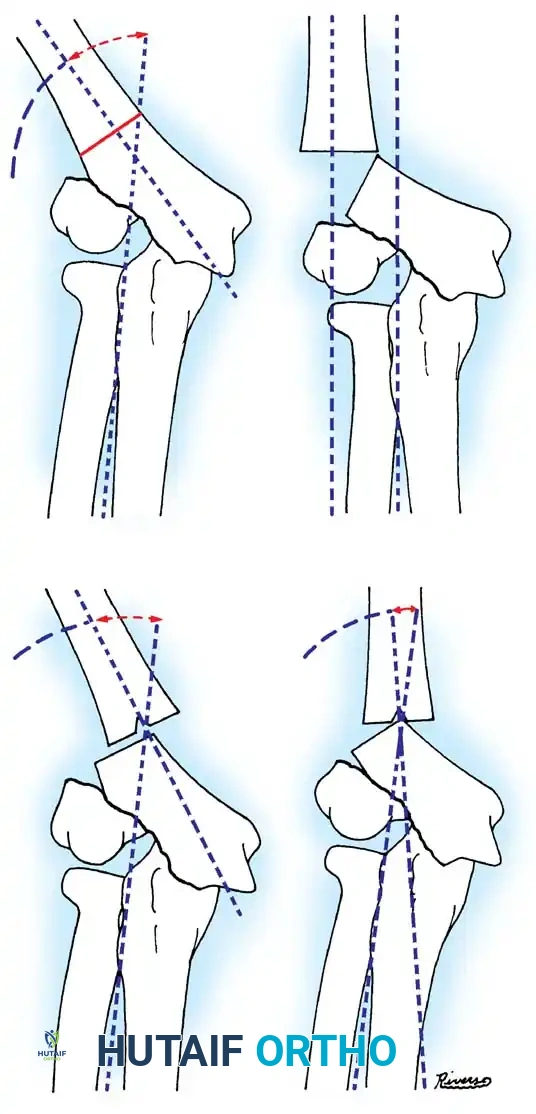
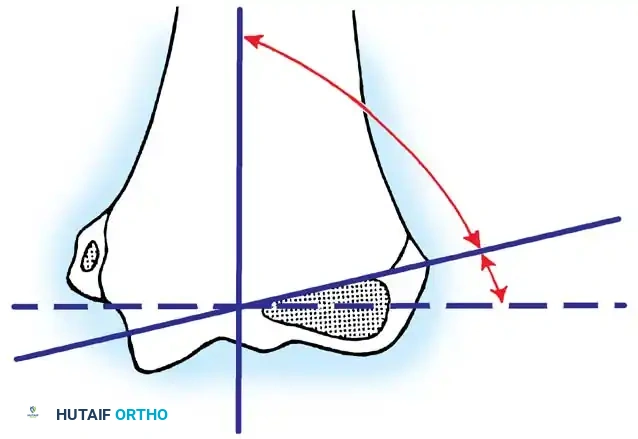
The osteology of the pediatric proximal radius is characterized by a complex, evolving morphology that dictates both injury patterns and surgical approaches. The radial head articulates with the capitellum of the distal humerus, functioning as a critical secondary stabilizer to valgus stress, transmitting approximately 60% of the axial load across the elbow joint. It also articulates medially with the radial notch of the ulna, facilitating the complex biomechanics of forearm pronation and supination. A critical clinical pearl for the evaluating surgeon is the recognition of the normal anatomical angulation of the pediatric radial neck. The proximal articular surface is not perfectly orthogonal to the radial shaft; it normally tilts up to 15 degrees laterally and slightly posteriorly. Inexperienced clinicians frequently and erroneously diagnose this physiological tilt as a subtle buckle fracture or minimal displacement. Therefore, mandatory comparison with high-quality contralateral radiographs is essential whenever the diagnosis remains equivocal.
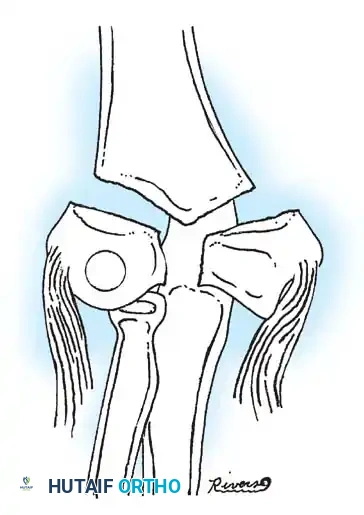
The ligamentous and capsular anatomy surrounding the proximal radius is intricate and unforgiving of surgical error. The radial head is encircled by the annular ligament, a robust fibrous band that anchors to the anterior and posterior margins of the radial notch of the ulna, maintaining the radial head in tight approximation during rotation. Blending with the annular ligament is the lateral ulnar collateral ligament (LUCL) complex, the primary restraint against posterolateral rotatory instability (PLRI). During open surgical approaches, particularly the Kocher interval, the surgeon must exercise extreme caution to incise the joint capsule anterior to the LUCL. Iatrogenic transection of the LUCL without meticulous repair will inevitably result in chronic, debilitating PLRI, necessitating complex secondary ligamentous reconstruction.
The vascular supply to the pediatric radial head is notoriously tenuous, rendering it highly susceptible to ischemic complications following trauma or surgical intervention. The primary blood supply is derived from intraosseous vessels ascending from the radial shaft through the metaphyseal neck. When a fracture occurs, particularly a completely displaced Salter-Harris type I or II, this intraosseous supply is abruptly severed. The secondary extraosseous supply arises from a delicate anastomotic ring formed by the radial recurrent artery and the interosseous recurrent artery, which penetrate the non-articular portion of the radial head via the synovial reflections. Extensive surgical dissection, aggressive periosteal stripping, or the use of multiple transarticular K-wires can obliterate these remaining extraosseous vessels, precipitating irreversible avascular necrosis (AVN) of the radial head, subsequent collapse, and severe functional impairment.
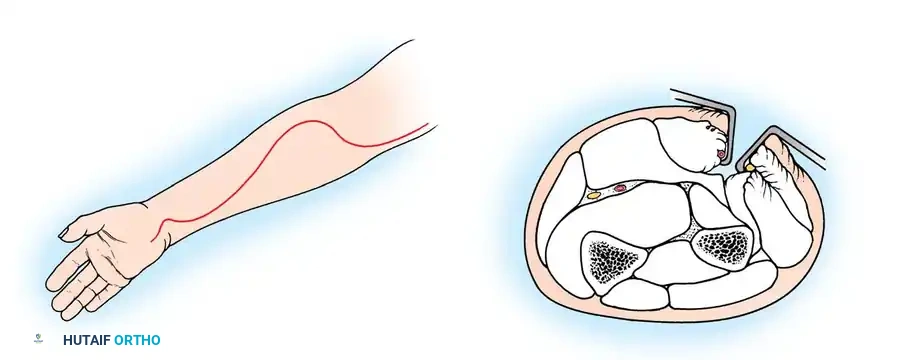
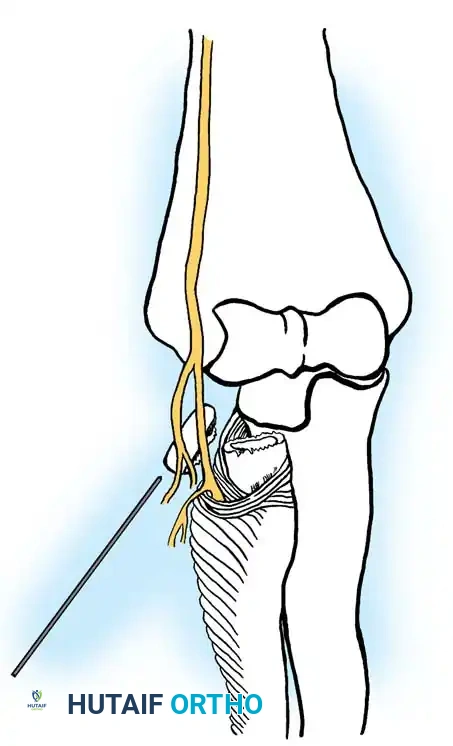
Neurologically, the proximal radius exists in perilous proximity to the deep branch of the radial nerve, also known as the posterior interosseous nerve (PIN). After bifurcating from the superficial radial nerve, the PIN courses distally and laterally, wrapping around the radial neck to dive beneath the superficial head of the supinator muscle at the arcade of Frohse. This anatomical relationship represents a profound pitfall during percutaneous pinning techniques. If a Kirschner wire or reduction tool is introduced directly from the lateral aspect, the PIN is at extreme risk of impalement, wrapping, or thermal necrosis. Therefore, all percutaneous interventions must be approached from the posterolateral or direct posterior trajectory, with the forearm in pronation to dynamically shift the PIN anteriorly and medially, safely out of the surgical trajectory.
Exhaustive Indications and Contraindications
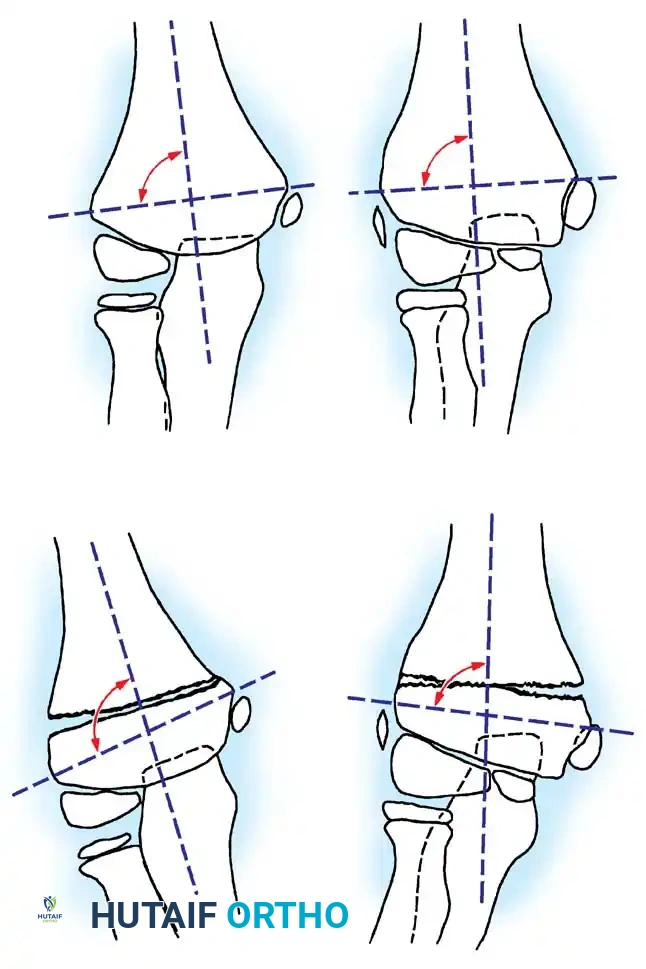
The overarching philosophy in the management of pediatric radial neck fractures is the restoration of precise radiocapitellar alignment to preserve the full, unhindered arc of forearm pronation and supination. The pediatric radial neck possesses a remarkable, yet finite, capacity for spontaneous remodeling. Consequently, determining the threshold for surgical intervention requires a nuanced understanding of acceptable angulation parameters, which are intrinsically tied to the patient's remaining skeletal growth potential. As a general surgical axiom, 30 to 45 degrees of residual angulation in the sagittal or coronal plane is deemed acceptable for closed treatment in younger children (under 10 years of age), yielding satisfactory long-term functional outcomes as the physis remodels the deformity. Attempting open reduction for angulation less than 45 degrees in a young child introduces entirely unnecessary risks of joint stiffness, avascular necrosis, and devastating radioulnar synostosis, often resulting in an outcome far inferior to the natural history of the unoperated fracture.
However, the indications for operative intervention become absolute when specific clinical and radiographic criteria are met. Surgical reduction (closed, percutaneous, or open) is strictly indicated when the initial fracture angulation exceeds 45 degrees, when there is translation (translocation) of the radial shaft exceeding 50% of the bone diameter, or when mechanical restriction of pronation and supination is clinically evident under anesthesia. Furthermore, according to landmark outcome studies by Tibone and Stoltz, the tolerance for residual angulation plummets in older children approaching skeletal maturity (older than 12 years). In this demographic, remodeling potential is negligible, and any residual angulation exceeding 15 to 20 degrees will likely result in a permanent, symptomatic block to forearm rotation, mandating aggressive surgical correction. Associated upper extremity injuries, such as medial epicondyle fractures, olecranon fractures, or acute elbow dislocations, also lower the threshold for surgical fixation to restore global elbow stability.
Contraindications to surgical intervention must be carefully weighed to avoid iatrogenic morbidity. Absolute contraindications include active surgical site infection, overwhelming systemic sepsis, or severe medical comorbidities precluding the safe administration of general anesthesia. Relative contraindications revolve primarily around the timing of the injury and the degree of displacement. Open reduction is relatively contraindicated in fractures presenting late (beyond 7 to 10 days post-injury). Delayed open surgical intervention drastically exponentially increases the risk of myositis ossificans, profound joint stiffness, and proximal radioulnar synostosis due to the robust, unyielding inflammatory and early callous response already underway. In such delayed presentations with unacceptable angulation, surgeons may opt for watchful waiting followed by a delayed corrective osteotomy, rather than attempting a morbid, forceful open reduction through inflamed, contracted tissues.
| Parameter | Indications for Operative Intervention (Percutaneous or Open) | Contraindications to Operative Intervention |
|---|---|---|
| Angulation | > 45 degrees in any plane (absolute indication if > 60 degrees) | < 30-45 degrees in a child < 10 years old |
| Translation | > 50% shaft translation | < 50% translation with acceptable angulation |
| Range of Motion | Mechanical block to pronation/supination under anesthesia | Full, smooth ROM under anesthesia |
| Patient Age | Older children (>12 years) with >15-20 degrees angulation | Young children (<8 years) with borderline angulation (remodeling expected) |
| Associated Injuries | Concomitant elbow dislocation, floating elbow, compartment syndrome | Isolated injury with acceptable alignment |
| Timing of Injury | Acute presentation (< 5-7 days) | Delayed presentation (> 10-14 days) - relative contraindication for ORIF |
Pre-Operative Planning, Templating, and Patient Positioning
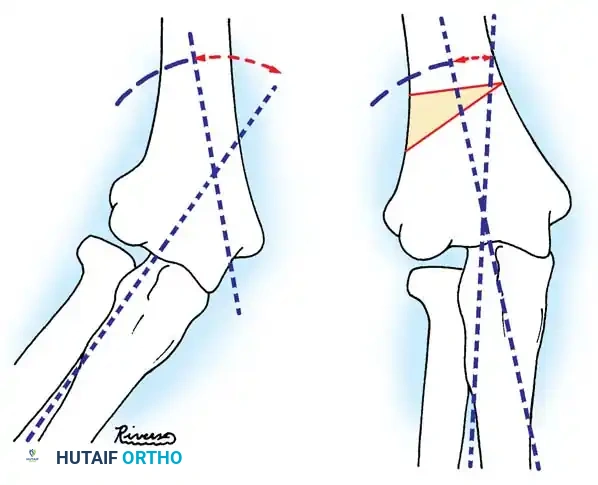
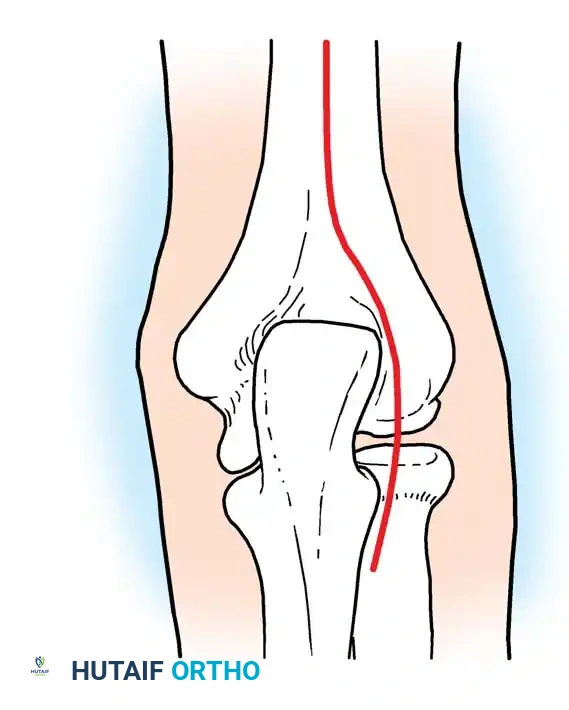
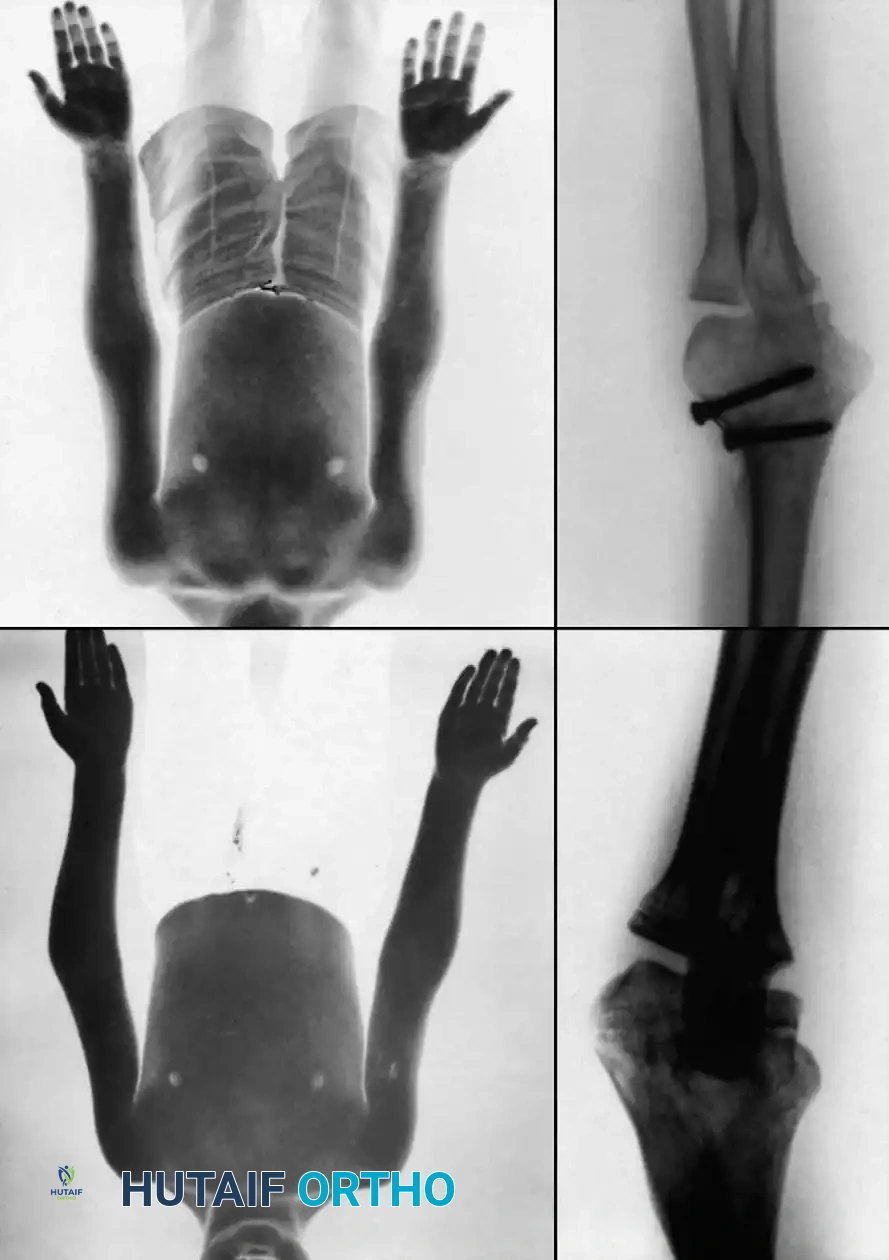
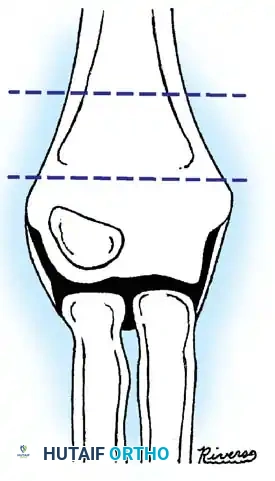
Meticulous pre-operative planning is the cornerstone of successful outcomes in pediatric orthopedic trauma, particularly in the unforgiving anatomical region of the proximal radius. The radiographic evaluation must begin with high-quality, orthogonal true anteroposterior (AP) and lateral radiographs of the affected elbow. The surgeon must critically evaluate the radiocapitellar line in all views; a line drawn bisecting the proximal radial shaft must pass precisely through the center of the capitellar ossific nucleus. Any deviation indicates residual subluxation, dislocation, or unacceptable angular deformity. Furthermore, the degree of angulation, the direction of tilt (anterior, posterior, lateral, or medial), and the percentage of translation must be precisely quantified. Given the subtle nature of physiological radial neck tilt, obtaining comparison radiographs of the uninjured contralateral elbow is strongly recommended to establish the patient's baseline anatomical parameters and to prevent the over-treatment of physiological variants.
In scenarios involving high-energy trauma, complex fracture-dislocations, or delayed presentations, advanced cross-sectional imaging may be warranted. Computed Tomography (CT) with 3D reconstructions can provide invaluable spatial information regarding the exact orientation of a completely displaced or intra-articularly incarcerated radial head fragment, allowing the surgeon to mentally rehearse the reduction maneuver. Magnetic Resonance Imaging (MRI) is rarely indicated in the acute setting but may be utilized in subacute or chronic cases to assess the viability (perfusion) of the radial head, the integrity of the annular ligament, or the presence of interposed soft tissue blocking reduction. Pre-operative templating is essential when planning for intramedullary fixation (e.g., the Metaizeau technique). The surgeon must measure the narrowest diameter of the radial medullary canal (the isthmus) on the AP radiograph to select the appropriate diameter of the Titanium Elastic Nail (TEN) or Kirschner wire. The selected implant should ideally occupy approximately 60% to 70% of the canal diameter to ensure adequate biomechanical purchase and rotational control during the reduction maneuver.
The choice of anesthesia and the setup of the operating theater are critical logistical considerations. General anesthesia with complete neuromuscular blockade is highly recommended to eliminate muscle spasm, particularly from the robust biceps brachii and supinator muscles, which act as formidable deforming forces. Conscious sedation may be attempted in the emergency department for simple closed reductions, but it often fails to provide the profound relaxation necessary for complex manipulations. The fluoroscopy unit (C-arm) must be positioned optimally, typically entering from the contralateral side of the table or parallel to the operative arm, allowing for unhindered, dynamic orthogonal imaging without compromising the sterile field or the surgeon's working space. The monitor should be placed directly in the surgeon's line of sight.
Patient positioning must facilitate unrestricted access to the entire upper extremity. The patient is placed supine on the operating table with the affected arm extended onto a radiolucent hand table. A sterile pneumatic tourniquet is applied high on the brachium but is generally not inflated for closed or percutaneous techniques, reserving inflation strictly for open procedures to minimize ischemic time. The entire upper extremity, from the fingertips to the axilla, is meticulously prepped and draped to allow for full, unhindered manipulation of the elbow and forearm. In cases of chronic dislocation where an ulnar osteotomy (Hirayama technique) is anticipated, the ipsilateral iliac crest must also be prepped and draped in the event that autologous structural bone grafting is required to manage the osteotomy gap or nonunion.

Step-by-Step Surgical Approach and Fixation Technique
Closed Reduction Maneuvers
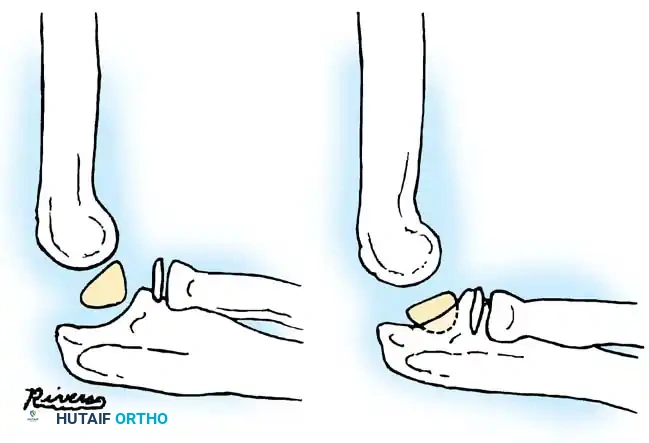
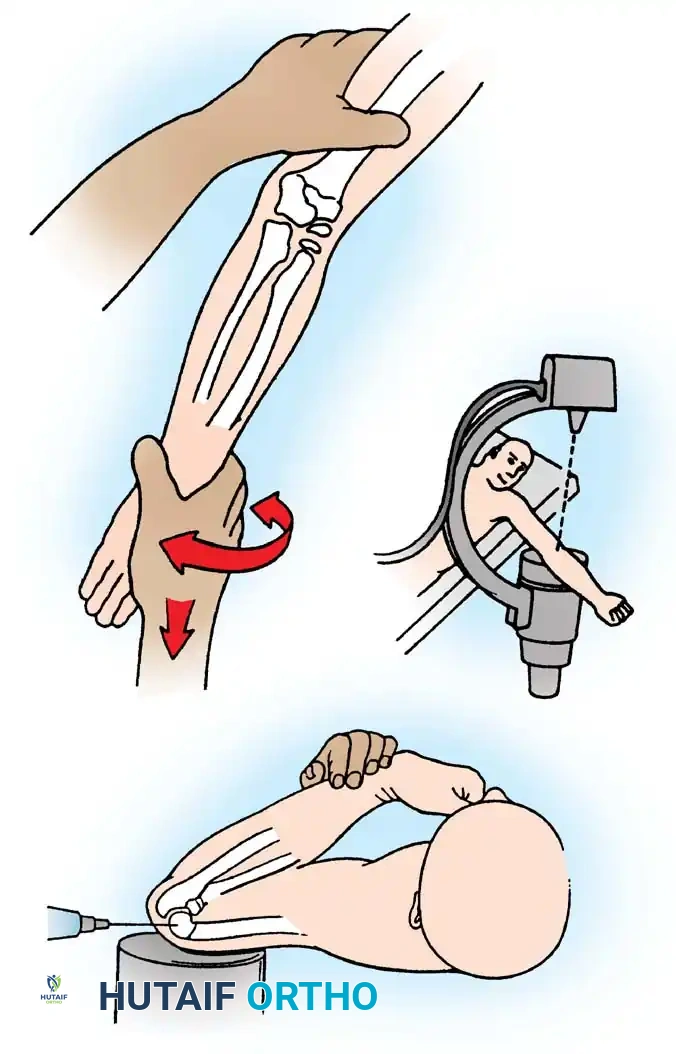
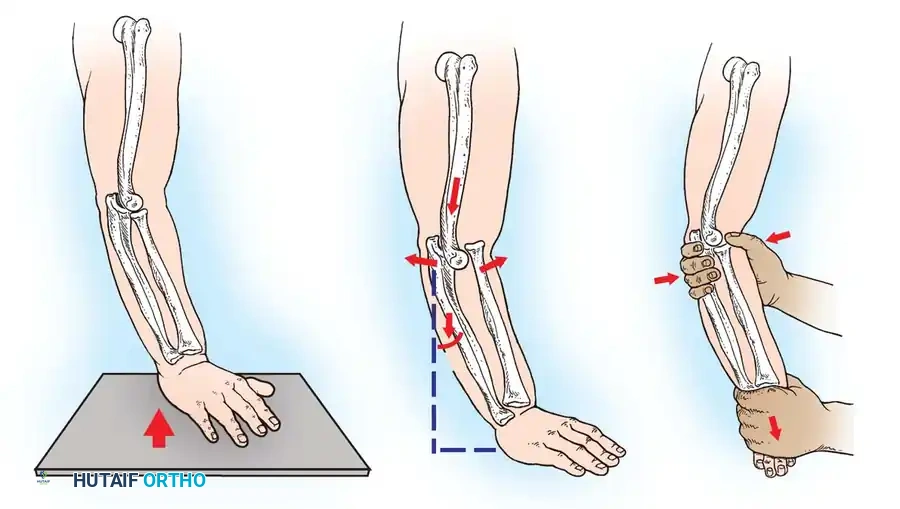
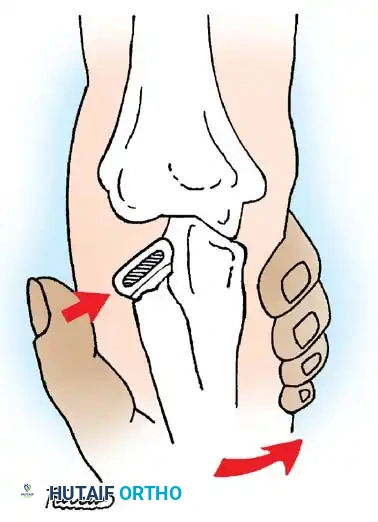
When the angular deformity of the radial neck exceeds the acceptable threshold of 45 degrees, closed reduction represents the mandatory first line of intervention. The Patterson technique, often modified by Neher and Torch, is the most universally applied and mechanically sound maneuver. The patient is positioned supine with the arm extended. An assistant provides rigid counter-traction by firmly grasping the distal humerus. The surgeon grasps the patient's wrist and forearm, maintaining the elbow in full, locked extension. The critical first step is the application of a profound varus stress to the elbow joint. This maneuver utilizes the intact medial collateral ligament as a hinge to distract the lateral compartment, effectively opening the radiocapitellar joint space and disengaging the impacted fracture fragments.
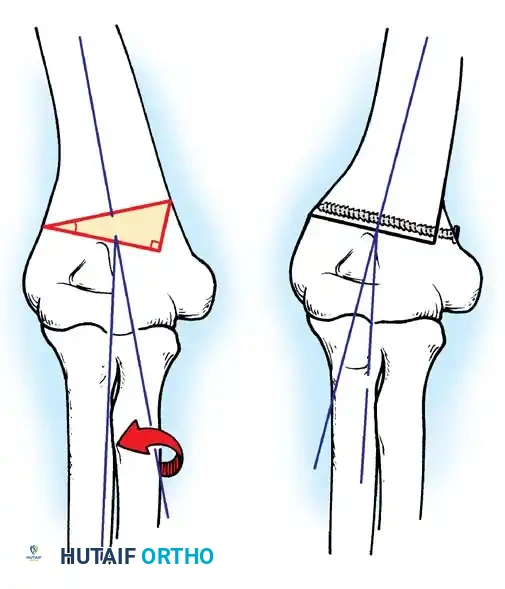
Once the lateral joint space is distracted, the surgeon utilizes the thumb of their free hand to apply direct, forceful, lateral-to-medial digital pressure over the tilted radial head. The goal is to lever the proximal fragment back into anatomical alignment with the radial shaft. While maintaining this digital pressure, the surgeon dynamically manipulates the forearm rotation. If the radial head is tilted laterally, the forearm is pronated; if tilted anteriorly, the forearm is supinated. This rotational maneuver utilizes the intact periosteal hinge to guide the radial head into position. Following the manipulative reduction, the varus stress is released, and the elbow is immediately brought into 90 degrees of flexion with the forearm locked in full pronation. This position utilizes the tension of the biceps tendon and the bony congruity of the joint to stabilize the reduction. Fluoroscopy is then utilized to confirm the restoration of the radiocapitellar line in both AP and lateral planes.
Percutaneous and Intramedullary Techniques
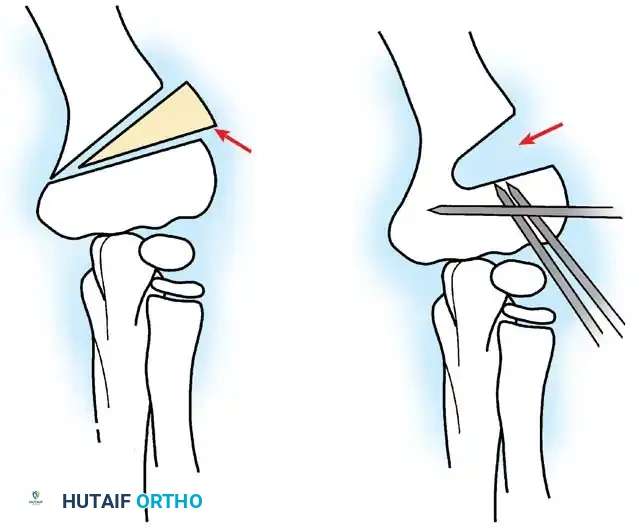
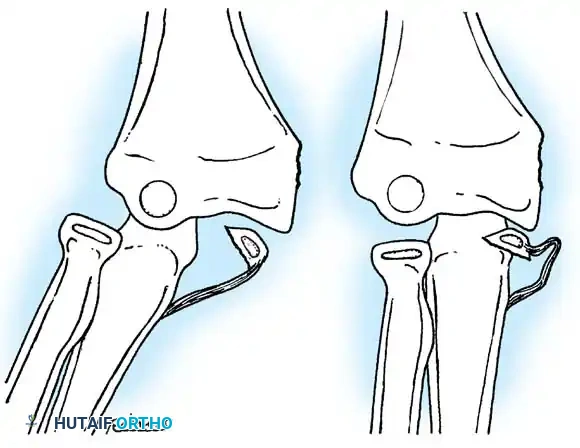
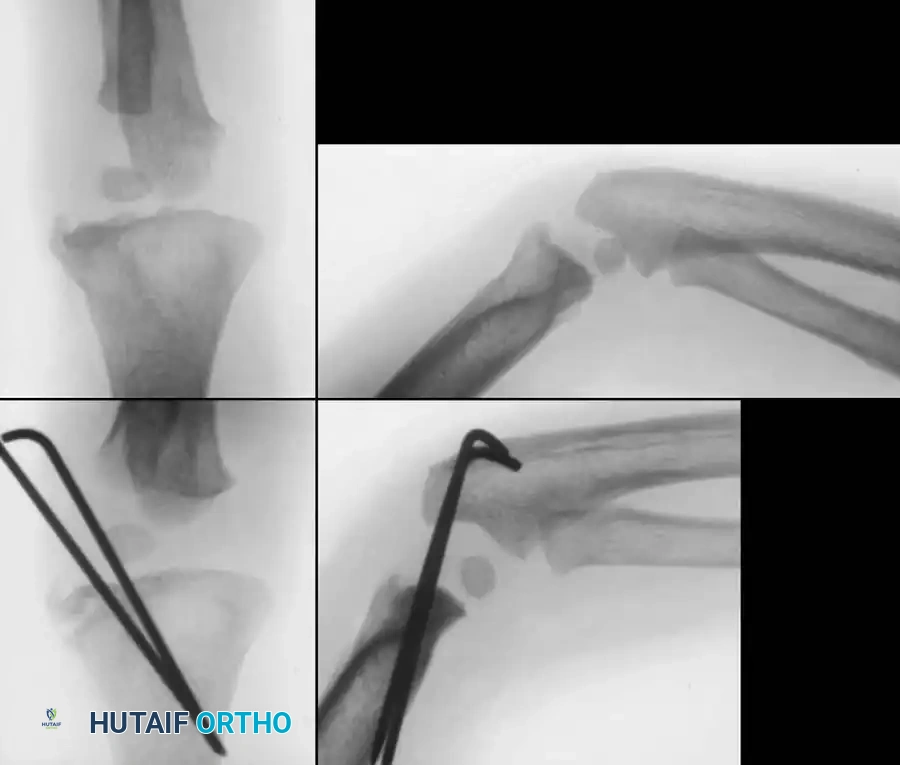
If closed manipulation fails to achieve acceptable alignment, the surgeon must escalate to percutaneous or intramedullary techniques before committing to the morbidity of an open approach. The Bernstein technique of percutaneous leverage is highly effective for moderately displaced fractures. Under fluoroscopic guidance, a robust Kirschner wire (typically 1.6mm or 2.0mm) is introduced percutaneously to act as a "joystick." Crucially, to avoid catastrophic injury to the posterior interosseous nerve (PIN), the wire must be introduced from the posterolateral or direct posterior aspect of the proximal forearm, with the forearm held in pronation. The wire is advanced until its tip engages the fracture site or the cortex of the displaced radial head. Using the intact cortex of the radial shaft as a fulcrum, the surgeon levers the radial head back into position. This technique requires significant tactile feedback and precise fluoroscopic visualization.
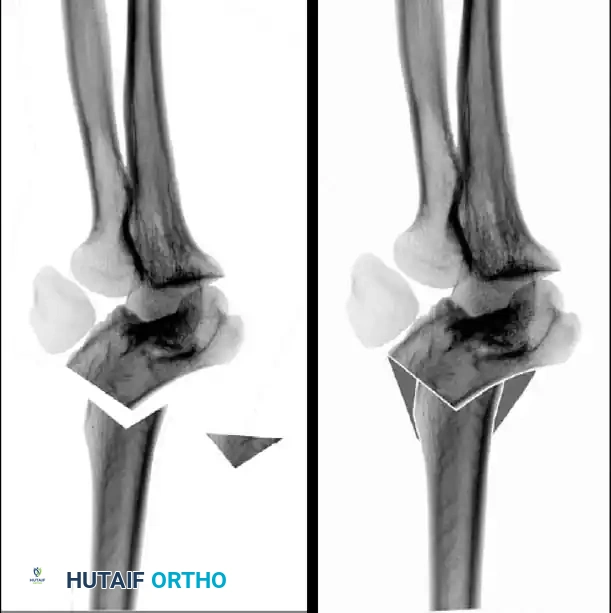
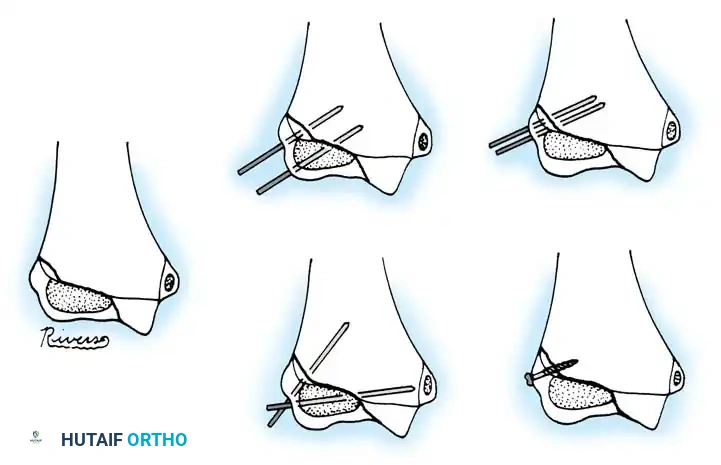
The Metaizeau technique, utilizing Elastic Stable Intramedullary Nailing (ESIN), has revolutionized the management of severely displaced or unstable pediatric radial neck fractures, boasting success rates exceeding 94%. A small 1-2 cm longitudinal incision is made over the distal lateral radial metaphysis, approximately 2-3 cm proximal to the distal physis, taking immense care to identify and retract the superficial branch of the radial nerve. The lateral cortex is breached with an awl or drill, creating an entry portal directed proximally. A titanium elastic nail (TEN) or a pre-bent steel Kirschner wire is prepared by sharply bending the distal 1.5 cm to an angle of 30 to 45 degrees. The nail is introduced retrograde into the medullary canal and advanced proximally under fluoroscopy.
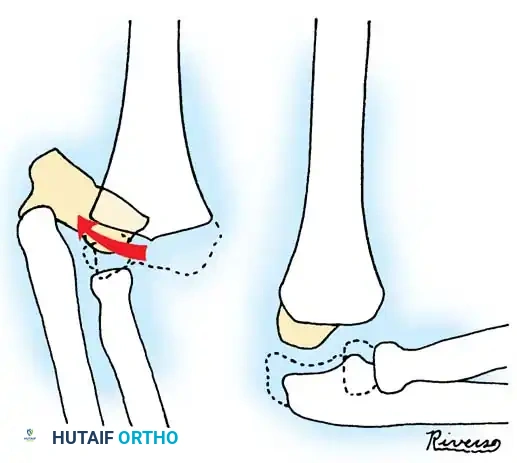
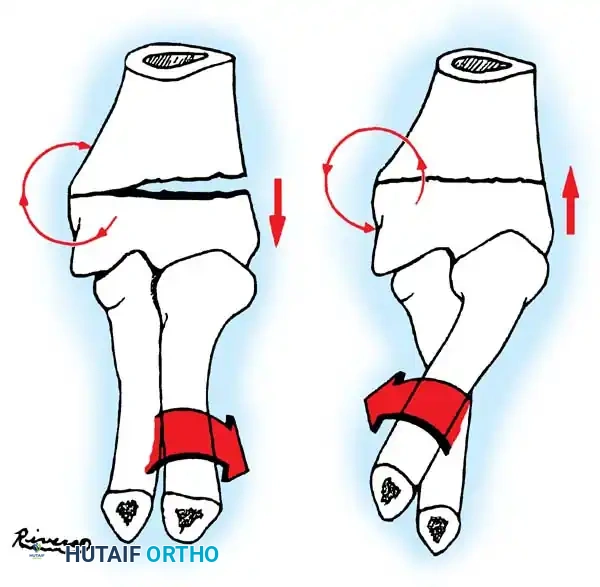
As the tip of the nail reaches the fracture site, it is carefully manipulated to cross the fracture hematoma and enter the medullary cavity of the displaced proximal epiphysis. Once the tip is securely embedded within the radial head, the critical reduction maneuver is performed. The surgeon rotates the nail 180 degrees around its longitudinal axis. The pre-bent tip acts as an internal cam or "joystick," physically elevating the tilted radial head and shifting it medially or laterally into perfect anatomical alignment beneath the capitellum. Once reduced, the nail is advanced slightly further to secure the subchondral bone, cut flush with the distal cortex to prevent soft tissue irritation, and the wound is closed.

Open Reduction and Internal Fixation
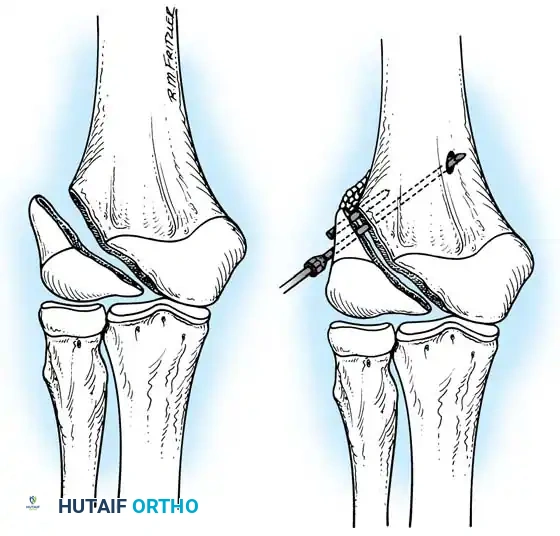
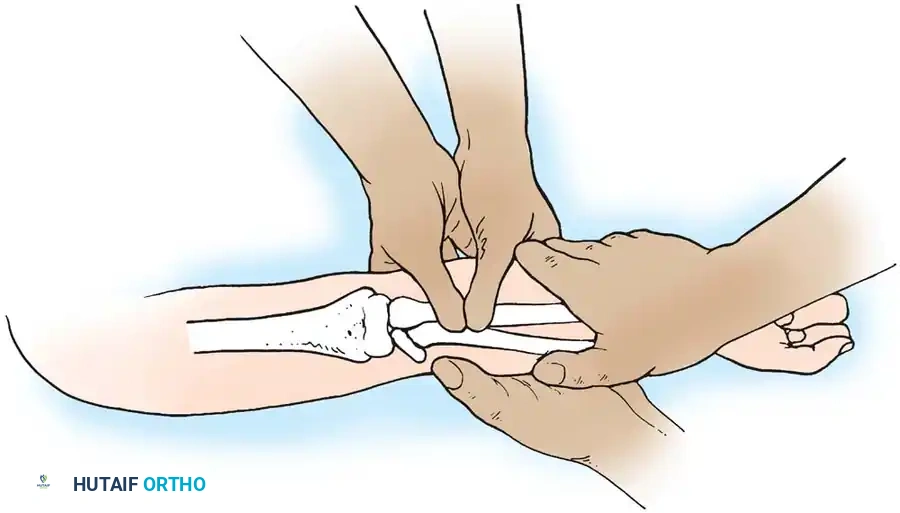
Open reduction is strictly reserved for cases where closed and percutaneous methods have definitively failed, or in cases of delayed presentation with incarcerated fragments. The surgical approach of choice is the lateral Kocher interval. The incision is made obliquely from the lateral epicondyle extending distally toward the ulnar crest. The deep fascia is incised, and the internervous plane between the anconeus (innervated by the radial nerve) and the extensor carpi ulnaris (innervated by the PIN) is meticulously developed. The surgeon must stay strictly on the ulnar side of the interval to protect the PIN. The joint capsule is exposed and incised longitudinally, strictly anterior to the lateral ulnar collateral ligament (LUCL). Preserving the LUCL is paramount to preventing iatrogenic posterolateral rotatory instability.
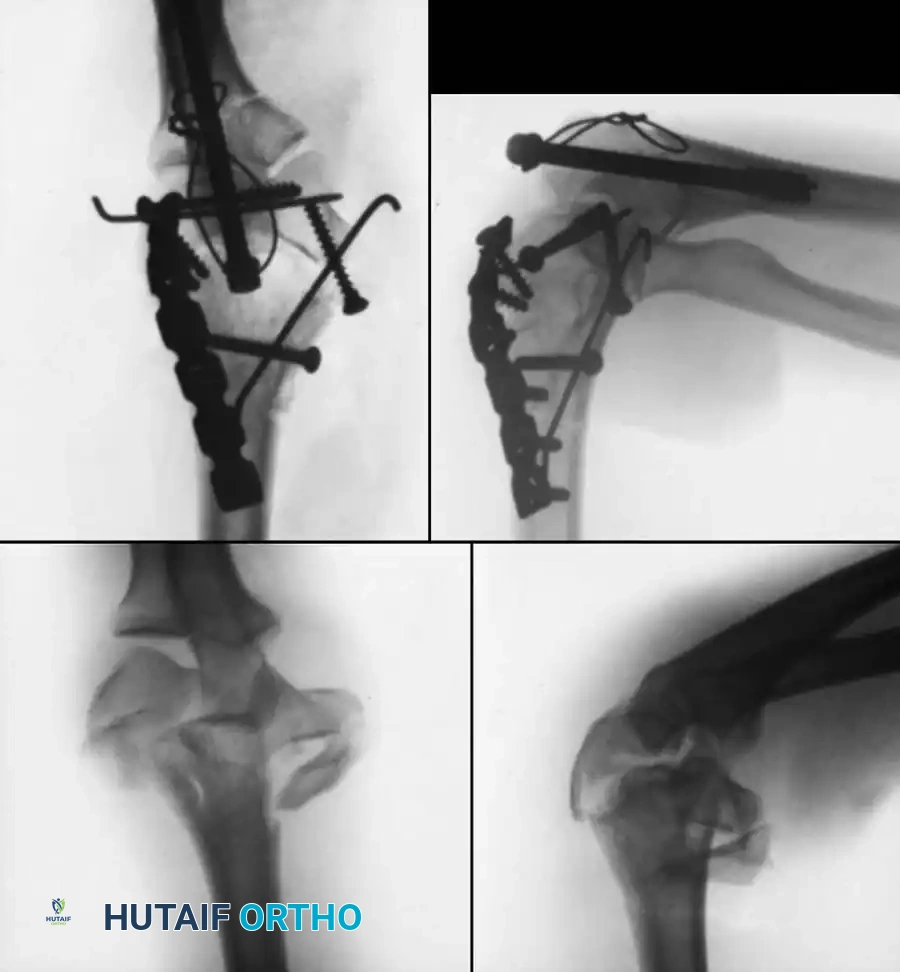
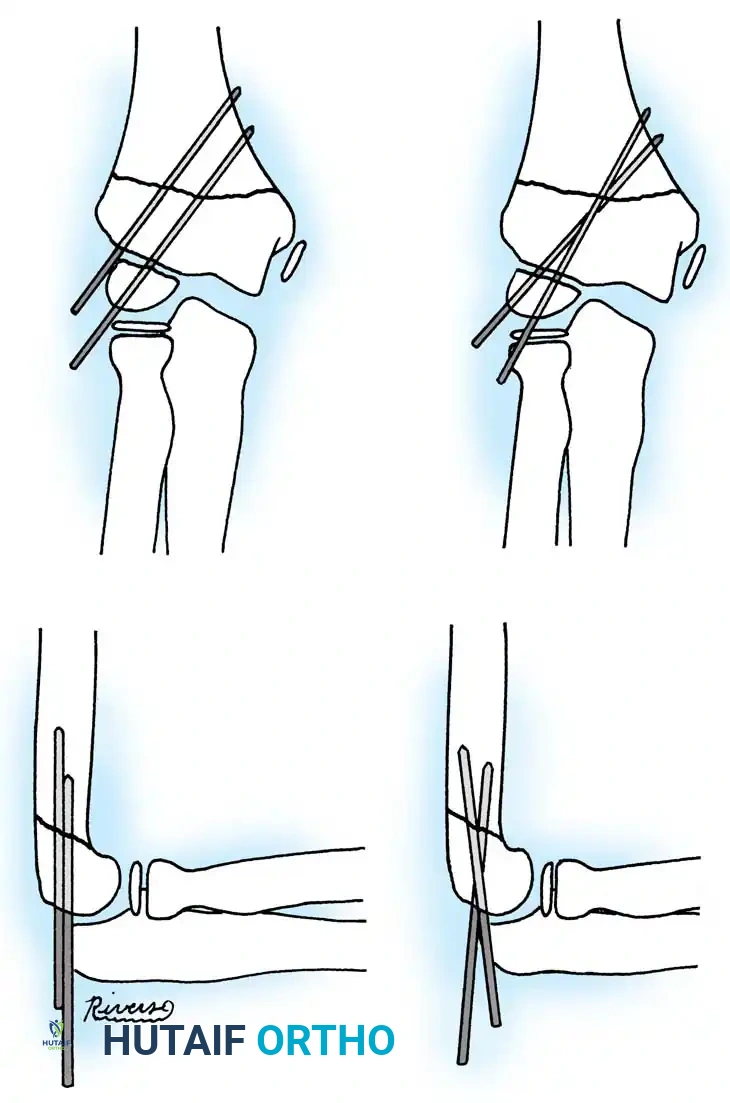
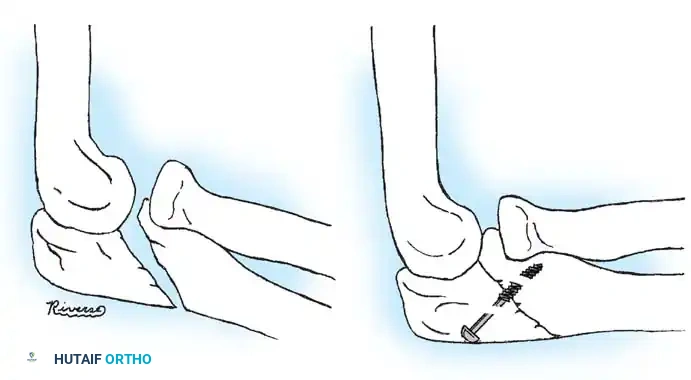
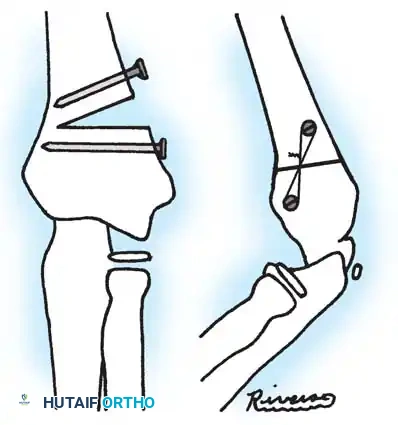
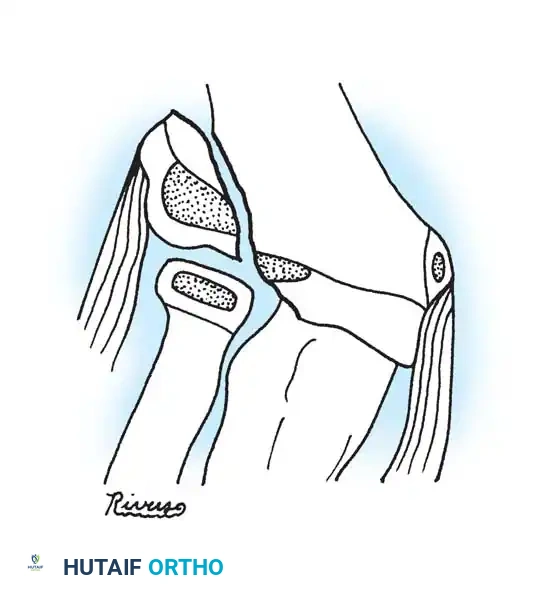
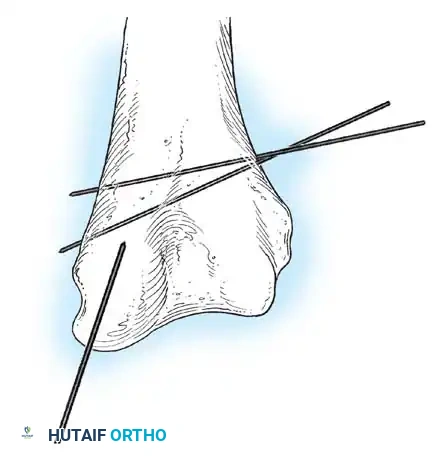
Once the joint is entered, the fracture hematoma is evacuated, and the interposed soft tissues (often the annular ligament or joint capsule) are extracted from the fracture site. The radial head is gently mobilized. Aggressive periosteal stripping must be absolutely avoided to preserve the fragile extraosseous blood supply. The fracture is reduced under direct vision. Due to the inherent instability of an open reduction, internal fixation is mandatory; periosteal sutures alone are biomechanically inadequate. Fixation is optimally achieved using two divergent, obliquely placed, smooth Kirschner wires driven from the radial head into the radial shaft. Transcapitellar (transarticular) wires should be avoided at all costs. While technically simpler to insert, transarticular wires traverse the joint space, carrying a prohibitively high risk of intra-articular breakage, cartilage damage, and septic arthritis, as documented extensively by Merchan and Fowles.

Advanced Reconstruction for Chronic Dislocations
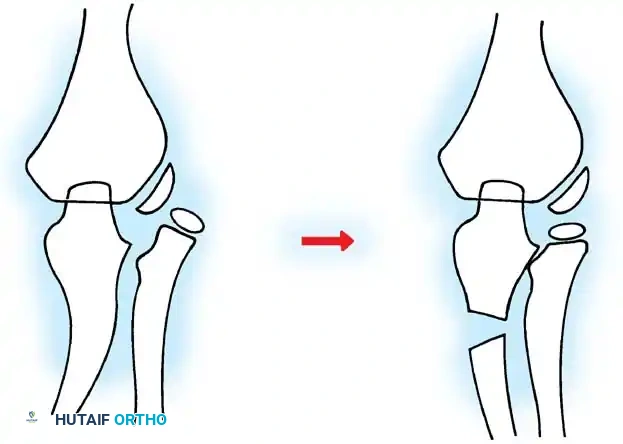
In complex scenarios involving chronic radial head dislocation—often a consequence of a missed acute injury, a Monteggia equivalent variant, or associated with plastic deformation of the ulna—simple open reduction of the radial head is biomechanically insufficient and doomed to fail. The chronically contracted interosseous membrane and the deformed ulna will inevitably force the radial head back into a dislocated position. In these challenging cases, the Hirayama Technique of ulnar osteotomy is the reconstructive procedure of choice. This technique leverages the interosseous membrane to dynamically pull the radial head back into the joint by overcorrecting the ulnar anatomy.
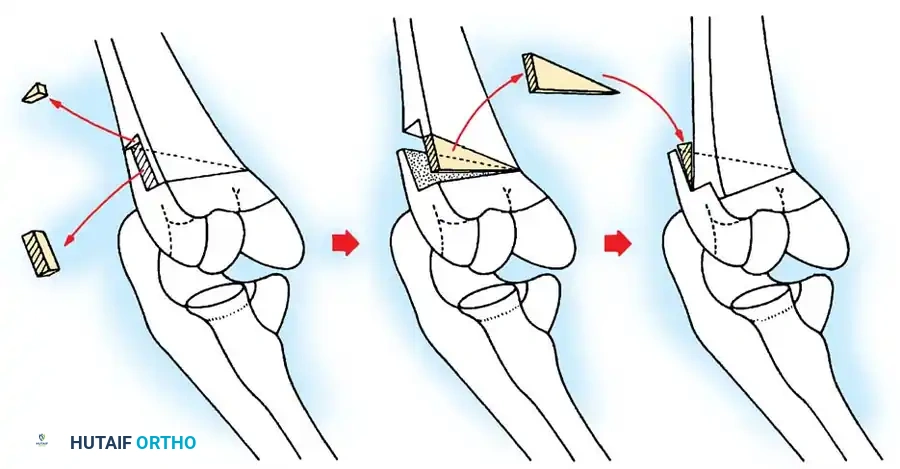
The procedure begins with a posterolateral approach to expose the radiohumeral joint and the proximal third of the ulna. Intra-articular scar tissue and the remnants of the hypertrophied annular ligament are excised to clear the radial notch. A subperiosteal transverse or oblique osteotomy of the ulna is performed approximately 5 cm distal to the tip of the olecranon. The critical step involves the controlled distraction and precise angulation of the osteotomy site. The ulna is distracted by approximately 1 cm to restore length. The direction of angulation is dictated by the direction of the radial head dislocation. For an anterior dislocation, the ulna is angulated posteriorly (creating a posterior convexity). For a lateral dislocation, the ulna is angulated medially. This overcorrection tightens the interosseous membrane, which acts as a tether, securely drawing the radial head into the radial notch. The osteotomy is then rigidly fixed with a dynamic compression plate pre-bent to approximately 15 degrees to maintain the overcorrection. The annular ligament is explicitly NOT repaired, as doing so in a chronic setting will severely restrict forearm rotation.
Complications, Incidence Rates, and Salvage Management
The surgical management of pediatric radial neck fractures is fraught with potential complications, many of which can lead to devastating, lifelong functional impairment. The most ubiquitous complication is the loss of forearm pronation and supination. This can result from inadequate reduction (leaving residual angulation > 45 degrees), prolonged immobilization, or the development of intra-articular adhesions. Premature physeal closure is another frequent sequela, occurring in up to 20% to 30% of cases, particularly following high-energy Salter-Harris type IV injuries or aggressive open reductions. While premature closure of the proximal radial physis generally results in minimal clinically significant limb length discrepancy (as the proximal physis contributes only 20% to the longitudinal growth of the radius), it can lead to relative overgrowth of the ulna and subsequent ulnocarpal impaction syndrome in adulthood.
Avascular necrosis (AVN) of the radial head is a catastrophic complication directly correlated with the severity of initial displacement and the invasiveness of the surgical intervention. The incidence of AVN approaches 10% to 20% in completely displaced fractures treated with open reduction. The disruption of both the intraosseous and extraosseous blood supply leads to osteocyte death, subsequent subchondral collapse, and profound joint incongruity. Clinically, AVN presents as insidious onset pain, progressive stiffness, and characteristic radiographic changes including sclerosis, fragmentation, and eventual flattening of the radial head. Proximal radioulnar synostosis is perhaps the most dreaded iatrogenic complication, occurring when the fracture hematoma organizes and ossifies across the
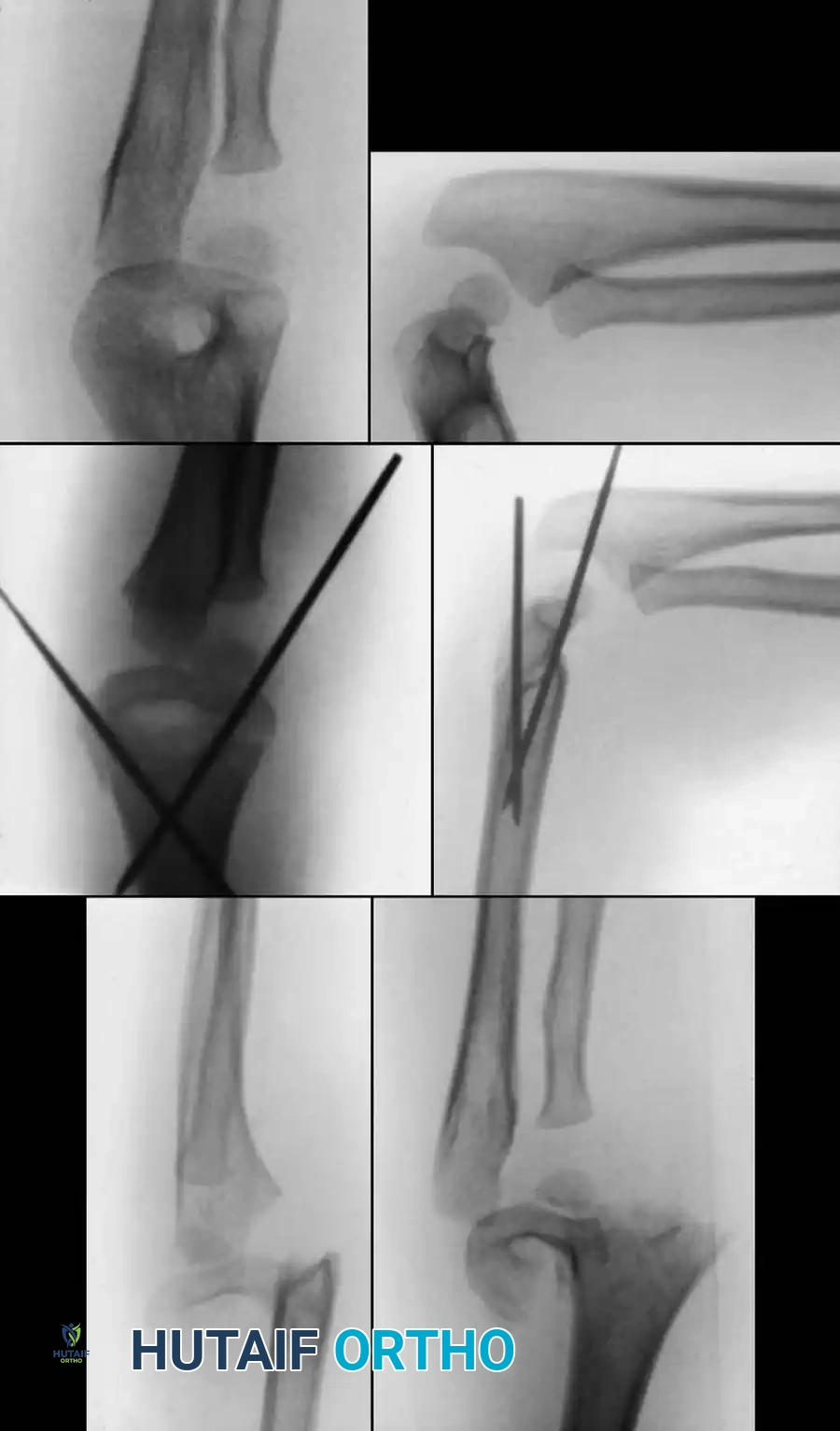
Clinical & Radiographic Imaging Archive