Introduction and Epidemiology
The posterior approach to the glenohumeral joint is a critical surgical corridor, affording direct access to the posterior capsule, labrum, glenoid, and posterior humeral head. While less commonly utilized than its anterior counterpart—the deltopectoral approach—its precise application is indispensable for a range of complex shoulder pathologies. These include posterior instability, posterior glenoid bone defects, reverse Hill-Sachs lesions, and specific intra-articular fracture patterns. The evolving understanding of glenohumeral biomechanics and the increasing sophistication of advanced imaging modalities have enhanced the orthopedic surgeon's ability to accurately diagnose and surgically manage these conditions, leading to a greater appreciation for the posterior surgical exposure.

Epidemiologically, posterior glenohumeral instability represents a distinct and often underdiagnosed clinical entity. Though less prevalent than anterior instability, it accounts for approximately 2% to 10% of all shoulder instability events. These injuries frequently result from specific mechanisms, most notably high-energy trauma (such as motor vehicle accidents where a force is applied to an adducted, internally rotated arm), seizure disorders, or electrical shock. Such mechanisms produce severe, involuntary muscular contractions that overcome the stabilizing structures of the posterior shoulder, leading to characteristic pathoanatomic lesions. These lesions include posterior labral tears (reverse Bankart lesions), impaction fractures of the anteromedial humeral head (reverse Hill-Sachs lesions), and posterior glenoid bone loss.
Chronic posterior instability can lead to progressive glenoid erosion, posterior decentering of the humeral head, and rapid development of secondary osteoarthritic changes if left unaddressed. Furthermore, the posterior approach serves as a cornerstone in revision total shoulder arthroplasty, or in complex primary arthroplasty cases requiring specific glenoid component placement, structural bone grafting for severe B2 or C-type glenoids (Walch classification), or management of severe posterior humeral head retroversion. Mastery of this approach is therefore fundamental for the orthopedic surgeon specializing in shoulder and elbow reconstruction.
Surgical Anatomy and Biomechanics
A thorough understanding of the regional anatomy is paramount for the safe and effective utilization of the posterior approach. The precise navigation of fascial planes, muscular intervals, and neurovascular structures dictates surgical success and minimizes catastrophic iatrogenic complications.
Superficial Landmarks and Incision
The primary superficial landmark for the posterior approach is the spine of the scapula. This subcutaneous osseous prominence is easily palpable and serves as a reliable guide for incision placement. The acromion, the lateral continuation of the scapular spine, also provides a key reference point for defining the deltoid origin and protecting the axillary nerve.
The spine of the scapula forms the most prominent palpable landmark posteriorly, extending medially from the vertebral border to terminate laterally as the acromion.

An incision can be centered over this landmark, typically extending inferiorly from the posterolateral corner of the acromion, running parallel to the lateral border of the scapula for approximately 5 to 7 cm. The length of the incision is dictated by the required exposure for the specific pathology, whether it be a localized capsulolabral repair or a more extensive structural bone block procedure.

Musculature and Internervous Planes
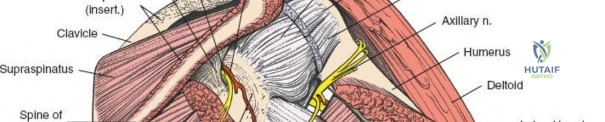
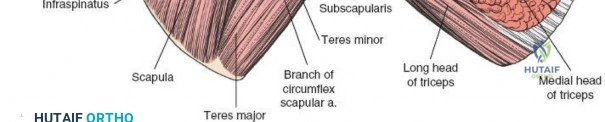
The posterior aspect of the shoulder is characterized by layers of musculature overlying the scapula and glenohumeral joint. From superficial to deep, these include the trapezius, latissimus dorsi, deltoid, and the rotator cuff muscles (supraspinatus, infraspinatus, teres minor). The deep fascia of the arm invests these muscles, creating compartments relevant to surgical dissection.
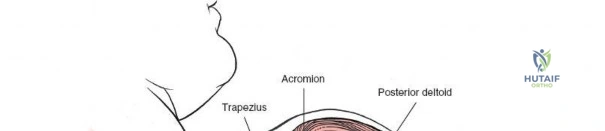
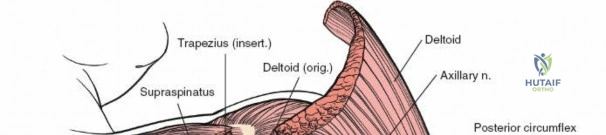
The deltoid forms the most superficial muscular layer overlying the rotator cuff posteriorly. Its posterior fibers originate from the spine of the scapula and the posterior acromion. The deltoid is innervated by the axillary nerve (C5, C6). A common technique involves splitting the deltoid fibers, typically in line with the posterior fibers, to expose the underlying infraspinatus and teres minor.
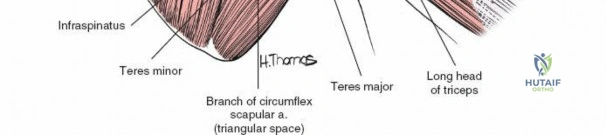
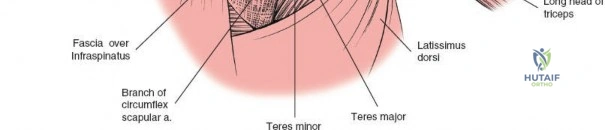
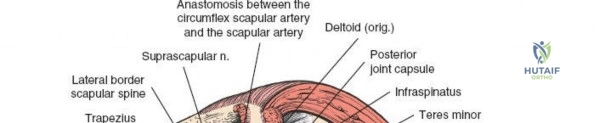
The true internervous plane utilized in the deep dissection lies between the infraspinatus (innervated by the suprascapular nerve) and the teres minor (innervated by the axillary nerve). Identifying this interval is critical. The teres minor can often be distinguished from the infraspinatus by a distinct fascial raphe and the difference in muscle fiber orientation; the infraspinatus fibers run more horizontally, while the teres minor fibers run obliquely superiorly and laterally toward the greater tuberosity.
Neurovascular Considerations
Navigating the posterior shoulder requires meticulous attention to two primary neurovascular structures the axillary nerve and the suprascapular nerve.
The axillary nerve exits the axilla posteriorly through the quadrilateral space. The boundaries of this space are the teres minor superiorly, the teres major inferiorly, the long head of the triceps medially, and the surgical neck of the humerus laterally. The nerve, accompanied by the posterior circumflex humeral artery, courses transversely across the deep surface of the deltoid. When splitting the deltoid, the surgeon must not extend the split further than 5 cm distal to the posterior acromion to avoid transecting the main trunk of the axillary nerve.

The suprascapular nerve courses through the suprascapular notch, supplies the supraspinatus, and then traverses the spinoglenoid notch to innervate the infraspinatus. At the level of the spinoglenoid notch, the nerve lies approximately 1.5 to 2.0 cm medial to the posterior glenoid rim. Deep retractor placement on the posterior glenoid neck must be carefully managed to avoid compression or traction injury to the suprascapular nerve.
Glenohumeral Biomechanics
The posterior capsulolabral complex is the primary static restraint to posterior glenohumeral translation. The posterior band of the inferior glenohumeral ligament (IGHL) is particularly critical; it becomes taut in internal rotation and flexion, acting as a hammock to support the humeral head. Surgical reconstruction via the posterior approach must aim to restore the tension and anatomical footprint of this complex. Over-tensioning the posterior capsule can lead to obligate anterior translation of the humeral head and severe external rotation deficits, highlighting the need for precise, anatomically based capsulorrhaphy.
Indications and Contraindications
The decision to utilize a posterior approach hinges on precise pathoanatomic diagnosis. While arthroscopic techniques have largely supplanted open posterior surgery for isolated soft-tissue posterior Bankart lesions, the open posterior approach remains vital for complex bony pathology, revision surgery, and arthroplasty.
Pathology Dictating Posterior Exposure
The classic indication for an open posterior approach is posterior glenohumeral instability associated with significant bony defects. When posterior glenoid bone loss exceeds 15% to 20% of the glenoid width, soft tissue repair alone is associated with unacceptably high failure rates. In these scenarios, a structural bone block (e.g., iliac crest autograft or distal tibia allograft) is indicated.
Similarly, large reverse Hill-Sachs lesions (engaging defects involving >20-25% of the articular surface) may require addressing through a posterior approach, although anterior approaches (like the McLaughlin procedure or Neer modification) are also utilized depending on the specific morphology and the need to address concomitant anterior pathology.

| Indication Category | Operative Indications (Posterior Approach) | Non-Operative Indications |
|---|---|---|
| Instability | Recurrent posterior instability with >20% glenoid bone loss | First-time atraumatic posterior subluxation |
| Bone Defects | Engaging reverse Hill-Sachs lesions requiring grafting | Voluntary habitual posterior dislocators (psychiatric overlay) |
| Fractures | Displaced posterior glenoid rim fractures (>5mm step-off) | Minimally displaced posterior glenoid fractures |
| Arthroplasty | Severe posterior glenoid wear (Walch B2/B3/C) requiring specific grafting | Patients with prohibitive medical comorbidities |
| Tumor/Infection | Resection of posterior glenohumeral neoplasms | Active, untreated systemic infection |
| Soft Tissue | Revision posterior capsulorrhaphy after failed arthroscopy | Atraumatic multidirectional instability (initially) |
Contraindications to the posterior approach include active local infection, severe medical comorbidities precluding anesthesia, and lack of a functioning anterior deltoid or subscapularis, which could lead to obligate anterior escape if the posterior restraints are over-tightened. Voluntary dislocators with a significant psychiatric component are generally considered a contraindication to operative stabilization until the underlying psychological factors are addressed.
Pre Operative Planning and Patient Positioning
Successful execution of the posterior approach requires exhaustive preoperative planning, relying heavily on advanced imaging modalities to quantify bone loss and delineate soft tissue integrity.
Advanced Imaging Protocols
Standard radiography must include a true anteroposterior (Grashey) view, a scapular Y view, and an axillary lateral view. The axillary view is paramount for assessing the concentricity of the humeral head within the glenoid vault and identifying posterior glenoid wear or acute fractures.

Computed Tomography (CT) is the gold standard for evaluating osseous architecture. 3D reconstructions with humeral head subtraction allow for precise quantification of posterior glenoid bone loss and calculation of glenoid retroversion. This is essential when planning a posterior bone block or determining the axis of correction for a glenoid component in total shoulder arthroplasty. Magnetic Resonance Imaging (MRI), preferably with intra-articular contrast (MRA), is utilized to evaluate the integrity of the posterior labrum, the posterior band of the IGHL, and the rotator cuff musculature.

Lateral Decubitus Positioning
While some surgeons prefer the beach chair position, the lateral decubitus position is highly advantageous for the posterior approach. The patient is placed in the lateral decubitus position on a beanbag with an axillary roll placed to protect the dependent brachial plexus.
The operative arm is draped free, allowing for full manipulation throughout the procedure. An articulated arm positioner (e.g., Spider or TRIMANO) can be utilized to hold the arm in varying degrees of forward elevation, internal rotation, and traction. This dynamic positioning is crucial; internal rotation tensions the posterior structures, facilitating identification of the intervals, while external rotation relaxes the capsule, aiding in retraction and deep exposure.
Detailed Surgical Approach and Technique
The surgical technique demands meticulous dissection and respect for the internervous planes to provide adequate exposure while preserving dynamic shoulder function.
Superficial Dissection and Deltoid Split
Following the incision from the posterolateral acromion extending distally toward the axillary fold, the subcutaneous tissues are sharply dissected to expose the deep fascia overlying the deltoid. Hemostasis is achieved using electrocautery.

The posterior deltoid fascia is incised in line with its muscle fibers. The deltoid split is initiated bluntly, utilizing the surgeon's fingers or a periosteal elevator, separating the muscle fibers down to the subdeltoid bursa. It is imperative that this split does not extend beyond 5 cm distal to the posterior border of the acromion. To prevent inadvertent distal propagation of the split and subsequent axillary nerve injury, a stay suture (e.g., #1 Vicryl) is placed at the inferior apex of the deltoid split.
Deep Dissection and Interval Identification
Once the subdeltoid bursa is excised, the underlying rotator cuff is visualized. The key to the deep exposure is identifying the internervous plane between the infraspinatus and teres minor.
The distinction between these two muscles can be subtle. The surgeon should look for a fat stripe that often delineates the interval. Additionally, the fiber orientation is a critical guide: infraspinatus fibers are more transverse, while teres minor fibers are oblique.
Blunt dissection is used to separate these muscles. Retractors (such as Richardson or Kolbel retractors) are placed to maintain the interval. As the dissection proceeds medially toward the glenoid neck, the surgeon must remain cognizant of the suprascapular nerve and vessels traversing the spinoglenoid notch. Retractors placed on the posterior glenoid neck must be positioned carefully, avoiding deep, medial plunging that could compress the nerve against the base of the scapular spine.

Capsulotomy and Joint Exposure
With the infraspinatus retracted superiorly and the teres minor retracted inferiorly, the posterior joint capsule is exposed. The type of capsulotomy performed depends on the underlying pathology and the planned procedure.
For posterior instability requiring a capsular shift, a vertical capsulotomy is typically performed approximately 1 cm lateral to the glenoid rim. This leaves a sufficient medial cuff of tissue for subsequent repair and plication. Alternatively, a T-shaped capsulotomy can be utilized, with the transverse limb extending laterally toward the humeral head, providing excellent exposure of both the glenoid and the posterior humeral head.
Upon entering the joint, a Fukuda ring retractor or a similar humeral head retractor is placed to gently subluxate the humeral head anteriorly, providing a direct, en face view of the posterior glenoid and labrum.
Structural Repair and Fixation Strategies
If a posterior bony Bankart lesion or significant bone loss is present, the glenoid neck is prepared to a bleeding cancellous bed using a high-speed burr or osteotomes.
For a posterior bone block procedure, the graft (iliac crest or distal tibia) is contoured to match the defect. The graft is typically positioned flush with or slightly recessed (1-2 mm) from the articular cartilage to prevent accelerated chondrolysis of the humeral head. Fixation is achieved using two partially threaded cannulated screws (typically 3.5 mm or 4.0 mm) placed parallel to the articular surface. Biomechanical studies emphasize that the screws must engage the dense anterior cortex of the glenoid vault to ensure rigid fixation.
Layered Closure
Following the structural repair, the capsule is meticulously addressed. In cases of instability, an inferior-to-superior capsular shift is performed to obliterate the redundant inferior pouch and tension the posterior band of the IGHL. The capsule is repaired using non-absorbable sutures.
The infraspinatus and teres minor interval is allowed to fall back into position; it rarely requires formal suturing, though a few loosely tied absorbable sutures can be placed to approximate the fascia. The deltoid split is approximated with absorbable sutures, followed by standard closure of the subcutaneous tissue and skin.
Complications and Management
The posterior approach, while providing unparalleled access to the posterior shoulder, carries a distinct profile of potential complications. Mitigation requires meticulous surgical technique and a thorough understanding of salvage strategies.
Iatrogenic Nerve Injury
Neurologic injury is the most feared complication. The axillary nerve is at risk during the superficial deltoid split and during inferior retraction of the teres minor. The suprascapular nerve is vulnerable during medial dissection and retractor placement near the spinoglenoid notch.

| Complication | Estimated Incidence | Etiology / Risk Factor | Salvage / Management Strategy |
|---|---|---|---|
| Axillary Nerve Injury | 1% - 3% | Deltoid split >5cm distal to acromion; aggressive inferior retraction | Observation with EMG at 3 months; nerve exploration |
Clinical & Radiographic Imaging

