Orthopedic & Rheumatology Board Review: JIA, Bone Tumors, Syringomyelia Cases | Part 8
Key Takeaway
This orthopedic board review provides challenging MCQs on Juvenile Idiopathic Arthritis (JIA), bone tumors (sarcomas, benign lesions), and Syringomyelia. It covers diagnosis, management, radiographic features, and complications like Charcot arthropathy. Essential for mastering complex musculoskeletal and rheumatologic cases for your ABOS exam.
Orthopedic & Rheumatology Board Review: JIA, Bone Tumors, Syringomyelia Cases | Part 8
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 35-year-old male presents with a painless burn on his right hand. Neurological examination reveals a loss of pain and temperature sensation in a cape-like distribution over his shoulders and upper extremities, while light touch and proprioception remain intact.
Which of the following neuroanatomical structures is primarily affected in the early stages of this condition?
Explanation
Question 2
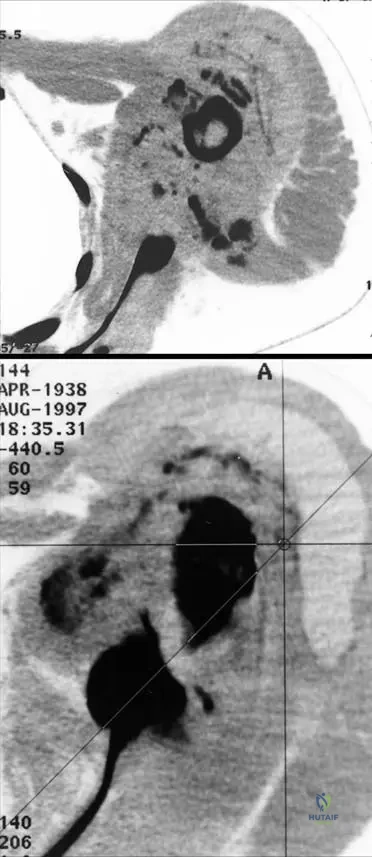
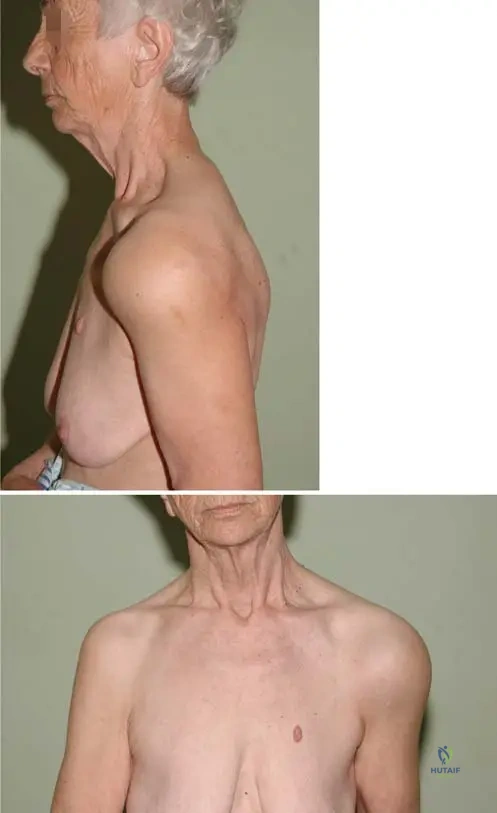
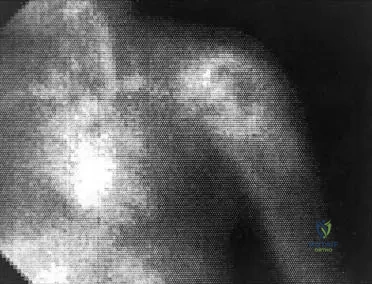
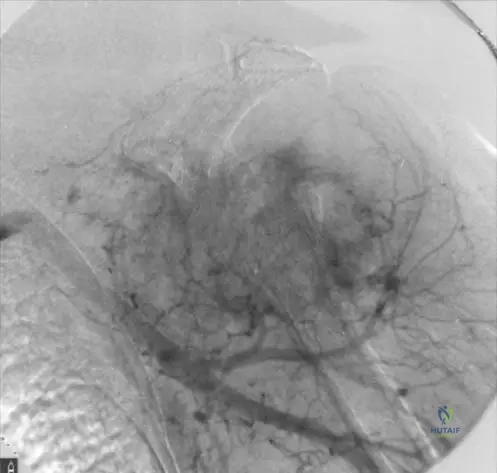
A 48-year-old woman presents with severe, progressive right shoulder swelling and instability over the last 6 months. She reports minimal pain despite significant deformity. Radiographs show extensive bone resorption of the humeral head and glenoid with intra-articular loose bodies.
What is the most appropriate initial management for this specific shoulder pathology?
Explanation
Question 3
A 13-year-old male presents with a left-sided thoracic scoliotic curve that has rapidly progressed by 15 degrees in the last 6 months. On physical examination, he has absent superficial abdominal reflexes on the left side.
What is the most appropriate next step in evaluation?
Explanation
Question 4
Which of the following associated conditions is most commonly identified on imaging in a patient diagnosed with syringomyelia?
Explanation
Question 5
A 24-year-old female with long-standing polyarticular Juvenile Idiopathic Arthritis (JIA) is scheduled for a bilateral total hip arthroplasty due to severe secondary osteoarthritis. Which of the following preoperative assessments is most critical for preventing a catastrophic intraoperative complication?
Explanation
Question 6
A 5-year-old girl is diagnosed with oligoarticular Juvenile Idiopathic Arthritis primarily affecting her right knee. She has an antinuclear antibody (ANA) positive titer. In addition to monitoring for leg length discrepancies, what mandatory screening must be instituted?
Explanation
Question 7
During a total hip arthroplasty in a young adult with advanced Juvenile Idiopathic Arthritis (JIA), the surgeon must be prepared for which of the following common anatomic challenges?
Explanation
Question 8
A 16-year-old male with a history of systemic JIA is currently treated with Etanercept. He sustained an anterior cruciate ligament tear and is scheduled for reconstruction. What is the recommended perioperative management of his biologic medication?
Explanation
Question 9
A 14-year-old male is diagnosed with high-grade osteosarcoma of the distal femur. He undergoes 10 weeks of neoadjuvant chemotherapy followed by wide surgical resection. Pathologic analysis of the resected specimen reveals 95% tumor necrosis. What does this finding indicate?
Explanation
Question 10
A 12-year-old boy presents with knee pain and a large soft tissue mass around the proximal fibula. Biopsy reveals small round blue cells. Molecular analysis confirms a t(11;22) chromosomal translocation. Which fusion protein is typically generated by this translocation?
Explanation
Question 11
When performing an incisional biopsy of a suspected malignant primary bone tumor in the lower extremity, which of the following principles must be strictly adhered to?
Explanation
Question 12
A 55-year-old male presents with deep pelvic pain. Radiographs reveal a large, destructive lesion in the ilium with 'rings and arcs' calcification. Biopsy confirms conventional high-grade chondrosarcoma. What is the mainstay of treatment?
Explanation
Question 13
A 22-year-old female presents with a destructive, eccentric, lytic lesion in the distal radius subchondral bone. Histology shows sheets of mononuclear cells with numerous multinucleated giant cells. Which targeted pharmacological therapy is indicated if the tumor is deemed unresectable or for massive recurrence?
Explanation
Question 14
A 6-year-old boy with oligoarticular JIA presents with an asymmetric gait. His right knee is swollen and warm but painless. On examination, his right leg is 2 cm longer than his left. What is the most likely mechanism for this leg length discrepancy?
Explanation
Question 15
A 68-year-old man complains of severe lower back pain and fatigue. Radiographs show multiple 'punched-out' lytic lesions in his skull and pelvis. Which of the following tests is the most appropriate next step to confirm the suspected diagnosis?
Explanation
Question 16
A 19-year-old male reports right thigh pain that is worse at night and dramatically relieved by ibuprofen. Imaging shows a 0.8 cm radiolucent nidus surrounded by dense sclerotic bone in the femoral diaphysis. What is the treatment of choice if he fails medical management?
Explanation
Question 17
A 40-year-old patient presents with pain in the proximal humerus. MRI shows a cartilaginous lesion. Which of the following MRI findings most strongly supports a diagnosis of low-grade chondrosarcoma rather than a benign enchondroma?
Explanation
Question 18
In a patient with known syringomyelia who presents with rapidly progressive neuropathic arthropathy (Charcot joint) of the elbow, what is the primary pathophysiological mechanism leading to joint destruction?
Explanation
Question 19
A patient with systemic Juvenile Idiopathic Arthritis is scheduled for cervical spine fusion due to basilar invagination. Which of the following airway complications is most frequently anticipated in this specific patient population by the anesthesia team?
Explanation
Question 20
A 30-year-old female presents with dull aching in her distal femur. Imaging shows an ill-defined, sclerotic, intramedullary lesion. Biopsy reveals woven bone stroma lacking osteoblastic rimming, forming a permeative pattern. Which of the following is an absolute contraindication for limb-salvage surgery in this disease?
Explanation
Question 21
A 45-year-old male presents with massive, painless swelling of his right shoulder and noticeable crepitus on range of motion. Neurological examination reveals a loss of pain and temperature sensation in a 'cape-like' distribution over his shoulders and back, but intact light touch and proprioception.
Based on the clinical presentation, what is the most likely diagnosis of the shoulder pathology?
Explanation
Question 22
In the pathogenesis of the neurological deficits seen in the patient from the previous question, which spinal cord structure is initially affected by the expanding central cystic cavity?
Explanation
Question 23
A 4-year-old girl is diagnosed with pauciarticular juvenile idiopathic arthritis (JIA). Her laboratory tests reveal she is ANA positive and Rheumatoid Factor (RF) negative. According to current guidelines, what is the most appropriate screening protocol for extra-articular manifestations in this patient?
Explanation
Question 24
A 12-year-old girl with long-standing systemic juvenile idiopathic arthritis presents with neck stiffness. Radiographs of the cervical spine are obtained. Which of the following is the most characteristic cervical spine radiographic finding in this condition?
Explanation
Question 25
A 12-year-old boy presents with a permeative, diaphyseal lesion in his femur with a periosteal 'onion-skin' reaction. A biopsy is performed. Which specific chromosomal translocation is most strongly associated with this tumor?
Explanation
Question 26
A 15-year-old male is diagnosed with conventional high-grade osteosarcoma of the distal femur. He undergoes 10 weeks of neoadjuvant chemotherapy followed by wide surgical resection. Pathologic analysis of the resected tumor is performed. Which of the following is the most significant prognostic factor for long-term survival?
Explanation
Question 27
A 32-year-old female presents with a purely lytic, eccentric lesion in the epiphysis extending into the metaphysis of the distal femur. A biopsy reveals numerous multinucleated giant cells in a stroma of mononuclear cells. If medical therapy is considered, which drug specifically targets the primary molecular pathway driving this tumor?
Explanation
Question 28
A 55-year-old male presents with a proximal humerus lesion displaying characteristic 'rings and arcs' of calcification on radiographs. Biopsy confirms a grade 2 chondrosarcoma. What is the most appropriate definitive management?
Explanation
Question 29
A 14-year-old female presents for evaluation of a newly noted left thoracic scoliosis. Neurological examination reveals absent abdominal reflexes. What is the most appropriate next step in management?
Explanation
Question 30
A 5-year-old boy has unilateral pauciarticular juvenile idiopathic arthritis predominantly affecting his right knee. If left untreated, what is the most likely long-term effect on his lower extremities?
Explanation
Question 31
An 18-year-old male complains of deep, aching pain in his proximal femur that is worse at night and dramatically relieved by ibuprofen. Imaging shows a 1 cm radiolucent nidus surrounded by dense reactive sclerosis. The pain is primarily mediated by high local concentrations of which of the following?
Explanation
Question 32
A 7-year-old girl is admitted with daily spiking fevers up to 39.5°C, a salmon-pink macular rash on her trunk, polyarthritis, and hepatosplenomegaly. Which of the following laboratory markers is most characteristically elevated out of proportion to other inflammatory markers in this specific condition?
Explanation
Question 33
A 13-year-old patient with a rapidly progressing 45-degree scoliosis curve is found to have a Chiari I malformation and a large cervicothoracic syrinx on MRI. What is the recommended sequence of surgical management?
Explanation
Question 34
A 40-year-old presents with a Charcot shoulder joint.
An MRI of the cervical spine and craniocervical junction is performed, showing a syrinx. Which cranial malformation is most frequently associated with this pathology?
Explanation
Question 35
When evaluating a cartilaginous lesion in the distal femur of a 45-year-old patient, which radiographic feature most strongly suggests a low-grade chondrosarcoma rather than a benign enchondroma?
Explanation
Question 36
An 8-year-old boy presents to the emergency department after a minor fall. Radiographs show a fracture through a central, radiolucent, cystic lesion in the proximal humerus metaphysis. A cortical fragment is seen resting at the dependent portion of the cyst ('fallen leaf' sign). What is the most appropriate initial management?
Explanation
Question 37
A 65-year-old male presents with widespread lytic bone lesions, renal insufficiency, and hypercalcemia. A diagnosis of Multiple Myeloma is established. Which of the following best describes the molecular mechanism responsible for the osteolytic bone lesions in this disease?
Explanation
Question 38
A 58-year-old male presents with a painful, destructive osteolytic lesion in the distal phalanx of his right thumb. Biopsy confirms metastatic adenocarcinoma. What is the most common primary malignancy to metastasize to locations distal to the knee or elbow (acrometastasis)?
Explanation
Question 39
A 50-year-old female with known syringomyelia presents with advanced Charcot arthropathy of the glenohumeral joint, experiencing severe instability and progressive loss of function that has failed extensive conservative management.
If surgical intervention is absolutely necessary, which procedure is generally considered the most appropriate salvage option despite high complication rates?
Explanation
Question 40
A 10-year-old girl with polyarticular juvenile idiopathic arthritis develops severe involvement of her temporomandibular joints (TMJs). Which of the following facial abnormalities is the expected consequence of chronic TMJ destruction during her growth phase?
Explanation
Question 41
A 4-year-old girl is diagnosed with oligoarticular Juvenile Idiopathic Arthritis (JIA) after presenting with a swollen, painless right knee. Laboratory testing reveals a positive antinuclear antibody (ANA). Which of the following is the most critical routine screening study required for this patient?
Explanation
Question 42
A 35-year-old male presents with painless burn scars on his hands. Neurological examination reveals loss of pain and temperature sensation in a 'cape-like' distribution over his shoulders and arms, but intact proprioception and vibratory sense.
What is the most likely diagnosis?
Explanation
Question 43
A 16-year-old boy presents with progressive right thigh pain that is noticeably worse at night and dramatically relieved by taking ibuprofen. Radiographs demonstrate a diaphyseal cortical thickening with a central radiolucent nidus measuring 8 mm. Which of the following is the most likely diagnosis?
Explanation
Question 44
A 14-year-old boy is diagnosed with a permeative diaphyseal lesion of the femur with an 'onion-skin' periosteal reaction. Biopsy confirms small round blue cells. Which of the following chromosomal translocations is most characteristic of this tumor?
Explanation
Question 45
A 10-year-old boy with polyarticular JIA is scheduled for elective bilateral total hip arthroplasty due to severe joint destruction. During the preoperative assessment, which of the following cervical spine abnormalities must be carefully ruled out before administering general anesthesia?
Explanation
Question 46
A 55-year-old male presents with a painful, enlarging mass in his proximal femur. Radiographs show a destructive lytic lesion with 'popcorn' intralesional calcifications. Biopsy confirms a grade II conventional chondrosarcoma. What is the most appropriate primary management?
Explanation
Question 47
A 45-year-old patient with known syringomyelia presents with massive, painless swelling and instability of the right shoulder. Radiographs demonstrate severe articular destruction, loose bodies, and debris consistent with a neuropathic joint.
Which of the following mechanisms best explains this joint pathology?
Explanation
Question 48
A 28-year-old female presents with an expansile, purely lytic epiphyseal lesion of the distal femur extending to the subchondral bone. Biopsy confirms a Giant Cell Tumor. If the tumor is deemed surgically unresectable due to its size and location, which of the following pharmacological agents is most appropriate to downstage the tumor?
Explanation
Question 49
A 6-year-old boy presents with daily high spiking fevers, an evanescent salmon-pink macular rash on his trunk, generalized lymphadenopathy, and symmetric polyarthritis. Laboratory tests show elevated ferritin, CRP, and leukocytosis. What is the most likely diagnosis?
Explanation
Question 50
A 15-year-old male is suspected of having an osteosarcoma of the distal femur. A core needle biopsy is planned. Which of the following is a critical orthopedic oncology principle regarding the placement of the biopsy tract?
Explanation
Question 51
In a patient developing syringomyelia, the expanding syrinx initially causes bilateral loss of pain and temperature sensation while preserving touch and proprioception. Which specific spinal cord structure is compressed first to cause this presentation?
Explanation
Question 52
A 9-year-old boy sustains a minor fall and presents with arm pain. Radiographs reveal a central, purely radiolucent metaphyseal lesion in the proximal humerus with a cortical fragment resting at the bottom of the cyst. What is the most likely diagnosis?
Explanation
Question 53
A 5-year-old girl with active, untreated oligoarticular JIA affecting solely her left knee is evaluated in the orthopedic clinic. Which of the following growth disturbances is most likely to be observed in the affected limb during the active inflammatory phase?
Explanation
Question 54
A 65-year-old male presents with generalized bone pain, fatigue, and renal insufficiency. Radiographs of the skull and pelvis demonstrate numerous 'punched-out' purely lytic lesions without reactive sclerosis. What is the most common primary malignant bone tumor in this age group?
Explanation
Question 55
A 30-year-old female undergoes an MRI of the cervical spine due to progressive bilateral upper extremity weakness and sensory loss. The MRI reveals a large cervical syrinx. What is the most common congenital malformation associated with this finding?
Explanation
Question 56
A 12-year-old girl presents with knee pain. MRI of the distal femur demonstrates an eccentric, expansile metaphyseal lesion containing multiple cystic spaces with distinct fluid-fluid levels. Histology shows blood-filled spaces separated by cellular septa. What is the most likely diagnosis?
Explanation
Question 57
A 7-year-old child with systemic JIA suddenly deteriorates in the hospital, developing an unremitting fever, hepatosplenomegaly, and encephalopathy. Laboratory studies reveal a paradoxical sharp drop in the erythrocyte sedimentation rate (ESR), profound thrombocytopenia, and a serum ferritin level of 15,000 ng/mL. What life-threatening complication has developed?
Explanation
Question 58
A 22-year-old patient presents with multiple palpable, hard masses on his hands and severe deformities. Imaging reveals multiple enchondromas. Physical examination also reveals numerous bluish soft tissue nodules which are identified as hemangiomas. What is the diagnosis?
Explanation
Question 59
As a cervical syrinx progressively enlarges ventrally, it begins to compress and destroy adjacent structures beyond the central commissure. Which of the following neurological findings in the upper extremities is a classic consequence of this ventral extension?
Explanation
Question 60
A 35-year-old male with a known long-standing asymptomatic distal femoral osteochondroma presents with new-onset, progressive pain and enlargement of the mass. An MRI is performed. Which of the following findings is most highly suspicious for secondary malignant transformation to a chondrosarcoma?
Explanation
Question 61
A 12-year-old girl with long-standing polyarticular Juvenile Idiopathic Arthritis (JIA) presents with new-onset clumsiness in her hands and hyperreflexia in her lower extremities. Which of the following is the most likely cervical spine radiographic finding?
Explanation
Question 62
A 28-year-old male presents with painless swelling and instability of his right shoulder over the past 6 months. Neurological examination reveals a loss of pain and temperature sensation over his shoulders and upper back, with preserved light touch and proprioception.
What is the underlying pathophysiology of his shoulder pathology?
Explanation
Question 63
In the management of high-grade intramedullary osteosarcoma, which of the following factors is considered the most significant predictor of overall patient survival?
Explanation
Question 64
Which of the following pediatric patients with Juvenile Idiopathic Arthritis (JIA) requires the most frequent slit-lamp examinations to screen for asymptomatic uveitis?
Explanation
Question 65
A 13-year-old boy presents with a rapidly progressive left-sided thoracic scoliosis and absent abdominal reflexes. MRI of the spine reveals a large syrinx extending from C5 to T8.
What is the most appropriate sequencing of treatment?
Explanation
Question 66
A 35-year-old female presents with knee pain. Radiographs show an eccentric, lytic lesion in the distal femur extending to the subchondral bone. Biopsy confirms Giant Cell Tumor (GCT). If medical management is considered prior to intralesional curettage to downstage the tumor, which agent is most appropriate?
Explanation
Question 67
A 6-year-old girl with persistent oligoarticular JIA affecting her right knee presents with a noticeable leg length discrepancy. Which of the following best describes the expected discrepancy and its mechanism?
Explanation
Question 68
A 14-year-old boy has an eccentric, expansile, lytic metaphyseal lesion in his proximal humerus. MRI demonstrates multiple fluid-fluid levels. Genetic analysis of the tissue would most likely reveal a translocation involving which of the following genes?
Explanation
Question 69
Which of the following is the most common etiology of syringomyelia in the pediatric population?
Explanation
Question 70
A 5-year-old boy with systemic Juvenile Idiopathic Arthritis (sJIA) suddenly develops unremitting fever, hepatosplenomegaly, purpura, and profound lethargy. Laboratory tests show marked hyperferritinemia, hypofibrinogenemia, and pancytopenia. What is the most critical immediate complication?
Explanation
Question 71
A 60-year-old man presents with deep thigh pain. Radiographs reveal a large diaphyseal lesion in the femur with endosteal scalloping greater than two-thirds of the cortical thickness and /"popcorn/" calcifications. What is the mainstay of treatment for this lesion?
Explanation
Question 72
When performing an incisional biopsy of a suspected malignant primary bone tumor in the distal femur, which of the following principles must be strictly adhered to?
Explanation
Question 73
Which of the following subsets of Juvenile Idiopathic Arthritis (JIA) carries the highest risk for developing chronic, asymptomatic anterior uveitis?
Explanation
Question 74
A 14-year-old female with long-standing polyarticular Juvenile Idiopathic Arthritis (JIA) is scheduled for a total hip arthroplasty. Before proceeding with endotracheal intubation, which of the following is the most critical preoperative radiographic evaluation?
Explanation
Question 75
A 45-year-old male presents with a painless, grossly swollen right shoulder. Examination reveals palpable crepitus, severe instability, and diminished pain and temperature sensation in the upper extremity.
What is the most likely underlying diagnosis?
Explanation
Question 76
In a patient who has undergone neoadjuvant chemotherapy and wide resection for a conventional osteosarcoma of the distal femur, which of the following histologic findings is the most significant prognostic indicator for long-term survival?
Explanation
Question 77
A 12-year-old boy presents with left-sided mid-back pain and is found to have a left thoracic scoliotic curve of 35 degrees. Abdominal reflexes are absent asymmetrically. What is the most appropriate next step in management?
Explanation
Question 78
A biopsy is planned for a suspected high-grade sarcoma of the distal femur. Which of the following is a critical principle when performing the incisional biopsy?
Explanation
Question 79
A 16-year-old girl is diagnosed with Ewing sarcoma of the femoral diaphysis. Cytogenetic analysis of the tumor cells is most likely to reveal which of the following translocations?
Explanation
Question 80
A 55-year-old male undergoes wide surgical resection for a conventional Grade II chondrosarcoma of the proximal femur. Which of the following best describes the role of adjuvant therapy for this condition?
Explanation
Question 81
A 6-year-old child with a known history of systemic-onset JIA (Still's disease) suddenly develops a high unremitting fever, hepatosplenomegaly, bleeding gums, and profound lethargy. Laboratory tests show a rapidly dropping platelet count and an exceptionally high serum ferritin level. What is the most likely diagnosis?
Explanation
Question 82
Giant Cell Tumor (GCT) of bone frequently causes significant local bone destruction. The osteolysis in GCT is driven by the interaction between RANKL and RANK. In this tumor, which cells express RANKL?
Explanation
Question 83
A 10-year-old girl is found to have a 45-degree right thoracic scoliosis and an enlarging cervicothoracic syrinx associated with a Chiari I malformation. What is the most appropriate management strategy?
Explanation
Question 84
A 16-year-old male complains of severe back pain, especially at night. Imaging reveals a 2.5 cm lytic lesion with central calcification in the posterior elements of L4. What is the most likely diagnosis?
Explanation
Question 85
A 7-year-old child with oligoarticular JIA affecting the right knee is noted to have a leg length discrepancy, with the right leg being 1.5 cm longer than the left. What is the primary mechanism causing this overgrowth?
Explanation
Question 86
A 50-year-old patient with known syringomyelia presents with massive, painless swelling and instability of the elbow joint.
The exact neuroanatomic lesion in syringomyelia that leads to this neuropathic joint typically originates in which structure of the spinal cord?
Explanation
Question 87
A 65-year-old male presents with bone pain and a pathologic fracture of the proximal humerus. Radiographs show multiple "punched-out" lytic lesions. A technetium-99m bone scan is performed and shows no significant uptake in the lesions. What is the most likely diagnosis?
Explanation
Question 88
A 30-year-old male presents with an eccentric, purely lytic lesion in the epiphysis of the distal femur extending to the subchondral bone. Biopsy confirms Giant Cell Tumor (GCT). If systemic therapy is considered, which of the following agents is most appropriate?
Explanation
Question 89
In patients with severe, long-standing Juvenile Idiopathic Arthritis (JIA) undergoing Total Hip Arthroplasty (THA), the surgeon must anticipate distinct anatomic challenges. Which of the following is most commonly encountered in this patient population?
Explanation
Question 90
A 22-year-old patient with Multiple Hereditary Exostoses (MHE) reports new, increasing pain and sudden growth of a previously stable lesion on the proximal tibia. What specific imaging finding is most indicative of malignant transformation?
Explanation
Question 91
Aneurysmal bone cysts (ABCs) are expansile, blood-filled cystic lesions. While they can be secondary to other tumors, primary ABCs are now known to be true neoplasms driven by a specific genetic rearrangement. Which gene translocation is diagnostic for a primary ABC?
Explanation
Question 92
Which of the following joint deformities is classically associated with the natural progression of untreated polyarticular Juvenile Idiopathic Arthritis in the hand and wrist?
Explanation
None
