Master ABOS Orthopedic Board Review: Bone Tumors, GIO & Neurofibromatosis | Part 1

Key Takeaway
This ABOS Board Review provides challenging multiple-choice questions on essential orthopedic topics. Master the diagnosis and management of diverse benign and malignant bone tumors, understand glucocorticoid-induced osteoporosis mechanisms and treatments, and review the clinical features and orthopedic complications of Neurofibromatosis Types 1 and 2 for exam success.
Master ABOS Orthopedic Board Review: Bone Tumors, GIO & Neurofibromatosis | Part 1
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Which of the following correctly describes the underlying molecular pathophysiology in Neurofibromatosis Type 1 (NF1)?
Explanation
Question 2
A 6-year-old child with NF1 presents with established anterolateral bowing and non-union of the tibia.
What is the primary histological finding at the site of the pseudoarthrosis that impairs healing?
Explanation
Question 3
A 14-year-old male is diagnosed with high-grade conventional osteosarcoma of the distal femur. What is the standard first-line neoadjuvant chemotherapy regimen?
Explanation
Question 4
Which radiographic feature in a patient with NF1 is most predictive of rapid progression of dystrophic scoliosis?
Explanation
Question 5
What is the primary function of the protein mutated in Neurofibromatosis type 1?
Explanation
Question 6
A 10-year-old boy with NF1 presents with a short, sharply angulated thoracic scoliosis. Radiographs show rib penciling and severe vertebral scalloping. What is the most appropriate surgical management?
Explanation
Question 7
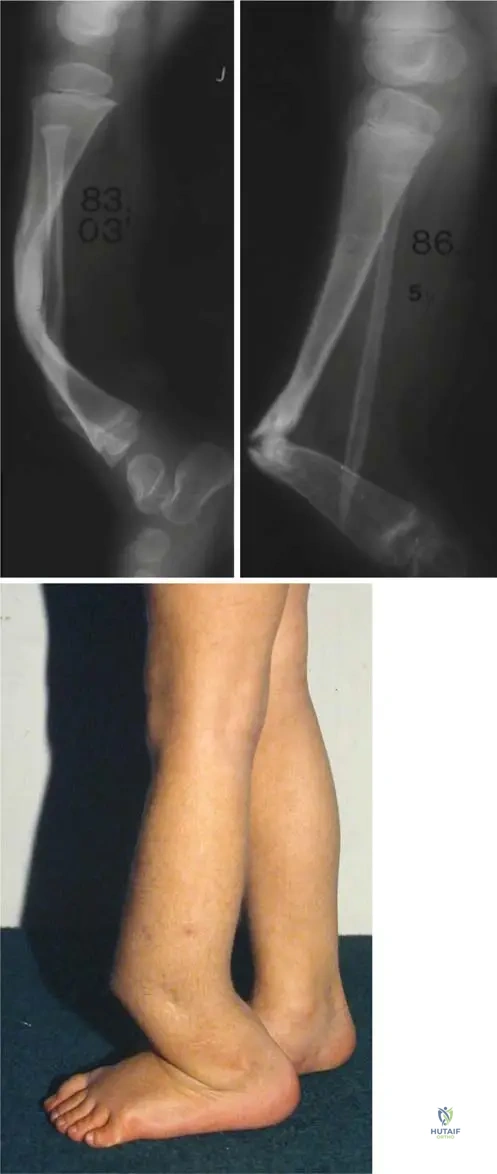
A 2-year-old child with NF1 presents with anterolateral bowing of the tibia and an impending fracture as seen in the clinical and radiographic image.
What is the gold standard surgical principle for managing established tibial pseudoarthrosis in this condition?
Explanation
Question 8
A 16-year-old male with a history of bilateral retinoblastoma develops a conventional osteosarcoma of the distal femur. This patient is most likely to harbor a germline mutation in which of the following genes?
Explanation
Question 9
A 45-year-old female presents with persistent, unprovoked deep shoulder pain. Radiographs reveal a stippled calcific lesion in the proximal humerus with endosteal scalloping affecting 80% of the cortical thickness. What is the most likely diagnosis?
Explanation
Question 10
Which chromosomal translocation is the diagnostic hallmark of Ewing sarcoma?
Explanation
Question 11
A 30-year-old female presents with an expansile, lytic lesion in the distal femur extending to the subchondral bone. Biopsy confirms a Giant Cell Tumor. What is the mechanism of action of Denosumab, a frequently used neoadjuvant therapy?
Explanation
Question 12
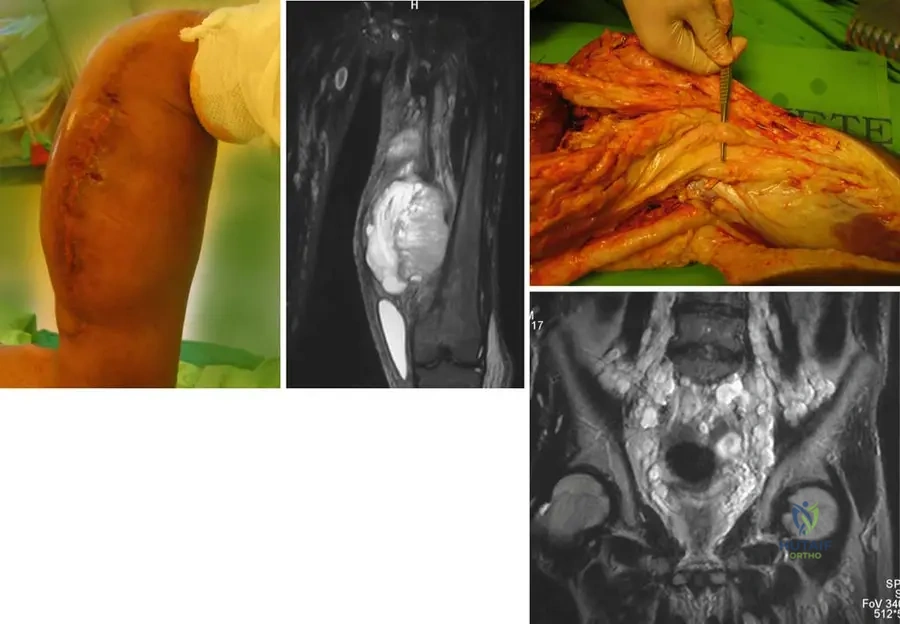
A 35-year-old male with NF1 presents with a rapidly enlarging, painful mass in his left thigh that originated from a long-standing plexiform neurofibroma. What is the most likely diagnosis?
Explanation
Question 13
Multiple Hereditary Exostoses (MHE) is inherited in an autosomal dominant pattern. Mutations in EXT1 and EXT2 genes disrupt the synthesis of which of the following?
Explanation
Question 14
A 12-year-old girl presents with a "shepherd's crook" deformity of the proximal femur, precocious puberty, and large café-au-lait spots with irregular borders. This syndrome is caused by a somatic mutation affecting which signaling pathway?
Explanation
Question 15
A 22-year-old male presents with chronic back pain that is poorly relieved by NSAIDs. Imaging reveals a 2.5 cm lytic lesion with central ossification in the posterior elements of L4. What is the most likely diagnosis?
Explanation
Question 16
A 65-year-old male presents with generalized bone pain and a pathological fracture of the proximal humerus. Radiographs show multiple punched-out lytic lesions, but a technetium-99m bone scan is negative. What is the most appropriate initial diagnostic laboratory test?
Explanation
Question 17
A 55-year-old male with a history of renal cell carcinoma presents with a painful, impending pathological fracture of the proximal femur due to a large lytic metastasis. What is the most critical pre-operative intervention prior to prophylactic stabilization?
Explanation
Question 18
A 28-year-old male presents with a slow-growing, painful mass near his knee joint. Radiographs reveal a soft tissue mass with stippled calcifications. Biopsy demonstrates a biphasic pattern of spindle and epithelial cells. What is the characteristic genetic mutation?
Explanation
Question 19
The gene mutated in Neurofibromatosis Type 1 (NF1) encodes for the protein neurofibromin. What is the normal cellular function of this protein?
Explanation
Question 20
A 7-year-old child with Neurofibromatosis Type 1 (NF1) presents with a rapidly progressive, 55-degree thoracic scoliotic curve. Radiographs show severe apical vertebral scalloping, rib penciling, and a short, sharp curve pattern. What is the most appropriate definitive management?
Explanation
Question 21
An 8-month-old infant with multiple café-au-lait spots is noted to have isolated anterolateral bowing of the tibia. Radiographs confirm a dysplastic tibia without a fracture.
What is the recommended initial management to alter the natural history of this condition?
Explanation
Question 22
During surgical resection of an established congenital pseudarthrosis of the tibia (CPT) in a patient with NF1, the thick, collar-like tissue surrounding the pseudarthrosis site is excised. What is the primary histological characteristic of this excised tissue?
Explanation
Question 23
A 15-year-old boy presents with knee pain. Radiographs reveal an eccentric, lytic lesion in the distal femoral epiphysis extending to the subchondral bone. Biopsy confirms a Giant Cell Tumor (GCT). Which cellular component is the true neoplastic cell, and which signaling molecule does it express to drive osteolysis?
Explanation
Question 24
A 28-year-old female with a known history of Neurofibromatosis Type 1 (NF1) and multiple plexiform neurofibromas presents with rapid enlargement and severe pain in a pre-existing thigh mass. Which of the following imaging modalities is considered the most sensitive for detecting malignant transformation in this patient?
Explanation
Question 25
A patient diagnosed with Ewing sarcoma undergoes cytogenetic testing. Which chromosomal translocation and resulting fusion gene is most classically associated with this malignancy?
Explanation
Question 26
Following neoadjuvant chemotherapy, a 16-year-old patient with conventional high-grade osteosarcoma undergoes wide surgical resection. The pathology report details the Huvos grading. What minimum percentage of tumor necrosis is required to be classified as a "good" histologic response?
Explanation
Question 27
A 13-year-old girl presents with pain in her left shoulder. Radiographs demonstrate a purely lytic, well-circumscribed lesion strictly localized to the proximal humeral epiphysis. She has open physes. What is the most likely diagnosis?
Explanation
Question 28
Which of the following primary carcinomas is most notorious for producing highly vascular, purely lytic osseous metastases that are largely resistant to radiation therapy, making wide resection or stabilization the preferred management?
Explanation
Question 29
A 9-year-old child with NF1 presents with a significant spinal deformity.
Reviewing the radiographs, all of the following are classic radiologic features of a dystrophic NF1 curve EXCEPT:
Explanation
Question 30
A 24-year-old female presents with a painless, slow-growing mass on the posterior aspect of her distal femur. Radiographs reveal a heavily ossified, lobulated mass on the cortical surface with a radiolucent cleft separating the tumor from the underlying cortex. What is the most likely diagnosis?
Explanation
Question 31
A 45-year-old patient presents with six large café-au-lait spots, axillary freckling, and Lisch nodules. He states his mother had similar skin findings and a leg deformity. What is the inheritance pattern and the chromosome involved in this disorder?
Explanation
Question 32
A 5-year-old boy is diagnosed with Neurofibromatosis type 1 (NF-1). Which of the following best describes the molecular pathophysiology of his condition?
Explanation
Question 33
A 3-year-old girl with Neurofibromatosis type 1 presents with anterolateral bowing of her left tibia. Radiographs show narrowing of the medullary canal and early cortical thickening. What is the natural history of this specific tibial deformity if left untreated?
Explanation
Question 34
A 10-year-old boy with NF-1 presents with a 45-degree short, sharp thoracic scoliotic curve. Radiographs demonstrate rib penciling, vertebral scalloping, and severe rotation. What is the most appropriate definitive management?
Explanation
Question 35
A 14-year-old boy undergoes neoadjuvant chemotherapy followed by wide resection for a conventional high-grade osteosarcoma of the distal femur. Which of the following factors provides the most important prognostic information for his long-term survival?
Explanation
Question 36
A 12-year-old girl presents with a painful, swollen mid-thigh. Radiographs show a permeative diaphyseal lesion with an "onion-skin" periosteal reaction. A biopsy reveals sheets of uniform, small blue round cells. Which of the following genetic translocations is most characteristic of this diagnosis?
Explanation
Question 37
A 65-year-old man presents with deep, persistent pelvic pain. Radiographs reveal a large, ill-defined destructive lesion in the ilium with "ring and arc" calcifications. Core needle biopsy confirms a grade 2 conventional chondrosarcoma. What is the most appropriate primary treatment modality?
Explanation
Question 38
A 35-year-old man with a known history of Neurofibromatosis type 1 reports that a long-standing, palpable mass in his thigh has recently doubled in size and become exquisitely painful. MRI shows an enlarging, heterogeneous mass along the sciatic nerve. What is the most likely diagnosis?
Explanation
Question 39
A 4-year-old child with a history of multiple low-energy fractures, blue sclerae, and dentinogenesis imperfecta is being evaluated. The underlying molecular defect in this condition primarily affects which of the following processes?
Explanation
Question 40
A 28-year-old woman presents with knee pain. Radiographs show an eccentric, expansile, lytic lesion in the distal femur extending to the subchondral bone without a sclerotic margin. Biopsy shows multinucleated giant cells in a background of mononuclear stromal cells. If systemic medical therapy is indicated, which molecular pathway is the primary target?
Explanation
Question 41
A 5-year-old boy is diagnosed with Neurofibromatosis Type 1. Which of the following best describes the genetic pathophysiology of this condition?
Explanation
Question 42
A 14-month-old child with multiple café-au-lait macules presents with the following tibial deformity.
What is the initial orthotic management and primary natural history concern?
Explanation
Question 43
When performing an incisional biopsy of a suspected primary malignant bone tumor in the distal femur, which of the following is an absolute surgical principle?
Explanation
Question 44
A 10-year-old girl with NF1 presents with a rapidly progressing spinal deformity. Radiographs demonstrate short-segment, sharp angular curves with vertebral scalloping and rib penciling.
What is the most appropriate surgical strategy?
Explanation
Question 45
A 16-year-old boy presents with knee pain. Radiographs reveal a metaphyseal permeative lesion in the distal femur with a 'sunburst' periosteal reaction. What is the most important prognostic factor for his long-term survival following neoadjuvant chemotherapy and wide resection?
Explanation
Question 46
A 12-year-old boy presents with a diaphyseal femur mass, fever, and elevated ESR. Radiographs show an 'onion-skin' periosteal reaction. Cytogenetics reveal a t(11;22) translocation. Which fusion protein is characteristic of this tumor?
Explanation
Question 47
A 28-year-old female presents with knee pain. Radiographs show an eccentric, lytic epiphyseal lesion in the proximal tibia. Biopsy confirms Giant Cell Tumor (GCT). If medical management is considered prior to curettage to downstage the tumor, what is the mechanism of action of the preferred agent?
Explanation
Question 48
A 14-year-old boy complains of right thigh pain that is worse at night and dramatically relieved by ibuprofen. CT scan shows a 7 mm radiolucent nidus surrounded by dense sclerosis in the femoral diaphysis. What is the primary mediator responsible for his specific pain pattern?
Explanation
Question 49
A 55-year-old man presents with an enlarging, painful mass in his proximal femur. Radiographs show a lytic lesion with 'popcorn' calcifications and endosteal scalloping. What is the standard of care for a conventional high-grade chondrosarcoma?
Explanation
Question 50
A 9-year-old boy with Neurofibromatosis Type 1 (NF1) presents with a rapidly progressing thoracic scoliosis. Radiographs demonstrate a short, sharp curve with vertebral scalloping, severe apical wedging, and penciling of the ribs. Which of the following is the most appropriate surgical strategy for this specific type of curve?
Explanation
Question 51
A 5-year-old child with NF1 presents with anterolateral bowing of the tibia and a frank pseudoarthrosis.
What is the gold standard surgical management to achieve union and maintain alignment in this condition?
Explanation
Question 52
A 32-year-old female presents with a destructive, expansile, purely lytic lesion in the distal femur epiphysis. Biopsy confirms a Giant Cell Tumor (GCT) of bone. She is treated preoperatively with denosumab. What is the primary mechanism of action of this medication in the context of GCT?
Explanation
Question 53
A 12-year-old boy presents with thigh pain and fever. Radiographs show a permeative diaphyseal lesion with an 'onion skin' periosteal reaction. A core needle biopsy is performed. Which of the following cytogenetic abnormalities is most characteristic of this diagnosis?
Explanation
Question 54
A 35-year-old male with a known diagnosis of Neurofibromatosis Type 1 reports rapid enlargement and new onset of severe, rest pain in a pre-existing plexiform neurofibroma in his thigh.
What is the most appropriate next step to evaluate for malignant transformation?
Explanation
Question 55
A 55-year-old male presents with shoulder pain. Radiographs reveal a large, destructive lesion in the proximal humerus with intralesional 'popcorn' calcifications. Biopsy confirms a grade 2 conventional chondrosarcoma. What is the most appropriate definitive management?
Explanation
Question 56
A 22-year-old male presents with dull, aching pain in his mid-back that is not significantly relieved by ibuprofen. Imaging shows a 3.5 cm lytic lesion with central mineralization in the posterior elements of T8. Histology demonstrates interlacing trabeculae of woven bone lined by prominent osteoblasts. What is the most likely diagnosis?
Explanation
Question 57
A 12-year-old female with Neurofibromatosis Type 1 (NF1) presents with a rapidly progressive 45-degree thoracic scoliosis. Radiographs demonstrate "penciling" of three adjacent ribs, severe vertebral body scalloping, and pronounced rotation. What is the most appropriate surgical management?
Explanation
Question 58
Which of the following accurately describes the genetic etiology of Neurofibromatosis Type 1 (NF1)?
Explanation
Question 59
A 4-year-old child presents with a congenital non-union of the tibia.
What is the typical direction of tibial bowing seen prior to fracture in patients with this condition?
Explanation
Question 60
A 35-year-old male presents with a rapidly expanding, painful mass in his left thigh. He has a known history of NF1 and multiple plexiform neurofibromas. Biopsy reveals a high-grade spindle cell sarcoma. Which of the following is the most likely diagnosis?
Explanation
Question 61
In the evaluation of primary pediatric bone tumors, which of the following cytogenetic abnormalities is considered pathognomonic for Ewing Sarcoma?
Explanation
Question 62
A 28-year-old woman presents with a lytic lesion in the distal femoral epiphysis extending to the subchondral bone. Biopsy shows mononuclear stromal cells and multinucleated giant cells. Which targeted therapy is most appropriate for extensive, unresectable disease?
Explanation
Question 63
A 16-year-old boy presents with multiple non-ossifying fibromas (NOFs), café-au-lait macules, and intellectual disability. Genetic testing for NF1 is negative. What is the most likely diagnosis?
Explanation
Question 64
A 30-year-old female presents with a low-grade osteosarcoma located on the posterior surface of the distal femur. What gene amplification is characteristically identified in this tumor?
Explanation
Question 65
A patient with NF1 undergoes an excisional biopsy of a symptomatic soft tissue mass. Histology reveals S-100 positive spindle cells with wavy nuclei in a myxoid stroma. What is the most appropriate classification of this tumor?
Explanation
Question 66
Regarding Glucocorticoid-Induced Osteoporosis (GIO) in orthopedic patients undergoing chronic steroid therapy, which mechanism primarily drives the rapid early bone loss?
Explanation
Question 67
A 10-year-old boy is found to have a well-circumscribed, eccentrically located, lytic lesion with a sclerotic margin in the distal tibial metaphysis on an incidental radiograph. He is asymptomatic. What is the most appropriate management?
Explanation
Question 68
A 5-year-old boy presents with six café-au-lait spots and axillary freckling. He is diagnosed with Neurofibromatosis Type 1 (NF1). The mutated gene in this condition normally functions to downregulate which of the following signaling pathways?
Explanation
Question 69
A 10-year-old female with Neurofibromatosis Type 1 presents with a rapidly progressive, short-segmented thoracic scoliosis. Radiographs reveal severe apical wedging, rib penciling, and evidence of dural ectasia. What is the most appropriate definitive management for this spinal deformity?
Explanation
Question 70
A 32-year-old female presents with a large, lytic epiphyseal lesion of the distal femur. Biopsy confirms Giant Cell Tumor of bone (GCT). If medical therapy with denosumab is considered prior to surgery, which cellular interaction is primarily targeted?
Explanation
Question 71
A 16-year-old male is undergoing treatment for localized high-grade conventional osteosarcoma of the proximal tibia. Following completion of neoadjuvant chemotherapy, surgical resection is performed. Which of the following findings is the most significant indicator of a poor overall prognosis?
Explanation
Question 72
A 12-year-old boy presents with thigh pain, fever, and a large diaphyseal mass in the femur with an "onion skin" periosteal reaction. Core needle biopsy demonstrates sheets of small round blue cells. Which chromosomal translocation is most characteristic of this diagnosis?
Explanation
Question 73
A 3-year-old girl with a known diagnosis of Neurofibromatosis Type 1 presents with the limb deformity shown in the provided clinical image.
This specific deformity most frequently progresses to which of the following complications if left untreated?
Explanation
Question 74
A 28-year-old male with a history of Neurofibromatosis Type 1 presents with a rapidly enlarging and newly painful mass in his left thigh. He has had a long-standing, painless plexiform neurofibroma in this location since childhood. What is the estimated lifetime risk for patients with NF1 to develop a Malignant Peripheral Nerve Sheath Tumor (MPNST)?
Explanation
Question 75
A 55-year-old male presents with deep pelvic pain. Imaging reveals a 12 cm destructive, permeative lytic lesion in the ilium with "popcorn" calcifications and cortical breakthrough. Biopsy confirms grade 3 conventional chondrosarcoma. What is the most appropriate primary treatment?
Explanation
Question 76
A 15-year-old male complains of right thigh pain that is significantly worse at night and dramatically improves 30 minutes after taking ibuprofen. Radiographs show a 1 cm radiolucent nidus surrounded by dense reactive sclerosis in the femoral diaphysis. What biochemical mediator is produced in excess by the central nidus, causing these classic symptoms?
Explanation
Question 77
A 65-year-old man presents with back pain and hypercalcemia. Radiographs show multiple "punched-out" lytic lesions in the skull and vertebral bodies. A bone marrow aspirate reveals >10% clonal plasma cells. Which of the following tests is most appropriate to confirm the presence of the abnormal protein associated with this condition?
Explanation
Question 78
A 14-year-old boy with a known history of Neurofibromatosis Type 1 undergoes a spine MRI due to worsening back pain and neurological symptoms, as shown in the provided clinical image.
Which of the following best describes the classical spinal manifestation demonstrated, which contributes to dystrophic spinal deformity in NF1?
Explanation
Question 79
A 9-year-old girl with Neurofibromatosis Type 1 presents with a rapidly progressive spinal curvature. Which of the following radiographic findings is most characteristic of dystrophic scoliosis in this patient?
Explanation
Question 80
A 4-year-old boy presents with the clinical deformity shown in the radiograph.
What is the recommended management for a frank pseudoarthrosis of the tibia in a patient with Neurofibromatosis type 1?
Explanation
Question 81
A 16-year-old male presents with severe knee pain. Radiographs reveal a destructive, lytic metaphyseal lesion in the distal femur. MRI shows multiple fluid-fluid levels. Biopsy reveals highly pleomorphic, atypical spindle cells producing delicate, lacelike osteoid. What is the most likely diagnosis?
Explanation
Question 82
A 12-year-old boy presents with an aggressive diaphyseal mass in his femur. Biopsy reveals small, round blue cells positive for CD99. Which of the following chromosomal translocations is most strongly associated with this tumor?
Explanation
Question 83
A 45-year-old male with a history of multiple hereditary exostoses (EXT1 mutation) reports a newly growing mass on his proximal humerus. MRI shows a cartilage cap thickness of 3.5 cm. What is the most likely histological finding in this secondary malignancy?
Explanation
Question 84
A 28-year-old woman with Neurofibromatosis Type 1 reports rapid enlargement and new onset severe resting pain in a long-standing thigh mass. MRI reveals a large, heterogeneous mass along the sciatic nerve with central necrosis. What is the most important prognostic factor for her likely diagnosis?
Explanation
Question 85
A 32-year-old woman presents with a lytic epiphyseal lesion in her proximal tibia. Biopsy confirms Giant Cell Tumor (GCT) of bone. Because the tumor is deemed unresectable, medical therapy is initiated. The prescribed medication targets which of the following?
Explanation
Question 86
A 19-year-old male complains of severe, aching pain in his right shin that is worse at night and relieved by ibuprofen. Radiographs show a dense cortical thickening with a small 6 mm radiolucent nidus. What is the primary pain-generating mechanism in this lesion?
Explanation
Question 87
A 65-year-old male presents with back pain and a pathological fracture of the L4 vertebral body. Laboratory studies reveal hypercalcemia and anemia. Which of the following is the most appropriate next step in confirming the suspected diagnosis?
Explanation
Question 88
A 55-year-old man presents with an impending fracture of his right femur secondary to a lytic metastatic lesion. His primary cancer is known to be renal cell carcinoma. Before performing prophylactic internal fixation, which of the following interventions is most strongly recommended?
Explanation
Question 89
A pediatrician refers a 5-year-old child for an orthopedic evaluation of scoliosis. During the exam, you note multiple hyperpigmented macules on the child's trunk. According to the NIH diagnostic criteria for Neurofibromatosis Type 1, what is the minimum number and size of these macules required to meet this specific criterion in a prepubertal child?
Explanation
Question 90
A 15-year-old male presents with knee pain. Radiographs reveal a 2 cm eccentric, well-circumscribed, lytic lesion with a thin sclerotic rim located entirely within the distal femoral epiphysis. Histology shows polygonal chondroblasts and "chicken-wire" calcifications. What is the most common complication following intralesional curettage of this tumor?
Explanation
Question 91
A 25-year-old male presents with a slowly growing, painful soft tissue mass near his knee joint. Radiographs show fine stippled calcifications within the soft tissue mass. Biopsy reveals a biphasic pattern of spindle cells and epithelial cells. What is the associated cytogenetic abnormality?
Explanation
Question 92
A 9-year-old girl with Neurofibromatosis Type 1 (NF1) presents with a rapidly progressive thoracic scoliosis. Radiographs demonstrate a short-segmented, sharply angulated curve with vertebral body scalloping, severe apical wedging, and rib penciling.
What is the most appropriate surgical management for this patient's spinal deformity?
Explanation
Question 93
A 34-year-old male undergoes intralesional extended curettage and cementation for a Campanacci Grade III Giant Cell Tumor (GCT) of the distal femur. Because of extensive cortical thinning and soft tissue extension, he was treated with neoadjuvant denosumab for 6 months prior to surgery. Which of the following is the most clinically significant concern regarding the use of neoadjuvant denosumab followed by intralesional curettage in this setting?
Explanation
None
