

Orthopaedic Surgery Board Exam Review: ABOS Part I & AAOS OITE Prep Questions | Part 22210
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 29-year-old, left-hand-dominant male presents to clinic complaining of left arm and shoulder pain for the last three days. The patient is an avid weight-lifter and was doing the bench press when his arm began to bother him. He has been using ice and resting with mild relief but has not been able to use his left arm for anything more than carrying light-weight objects. He is also having difficulty with simple activities such as putting on his shirt. On physical examination, the patient has ecchymosis and a prominent cord-like structure on the anterior left axilla. He has significant weakness with left shoulder adduction and internal rotation. He has a negative Hawkins sign and a negative Yergason sign.
Based on the information obtained thus far, which of the following is the most likely diagnosis?

Explanation
Correct Answer: B
The patient's presentation is classic for a pectoralis major muscle (PMM) rupture. The mechanism of injury (weight-lifting, bench press), acute onset of pain, ecchymosis, and the presence of a prominent cord-like structure in the anterior axilla (representing the continuous fascia of the PMM) are highly indicative. Significant weakness with shoulder adduction and internal rotation further supports this diagnosis, as these are primary functions of the pectoralis major. The patient's young age makes a rotator cuff tear less likely, and the negative Yergason sign rules out a biceps tendon rupture. Poland syndrome is a congenital absence of the PMM, which would present differently and not as an acute injury. Pectoralis minor muscle rupture is exceedingly rare and would not typically present with these specific findings.
Question 2
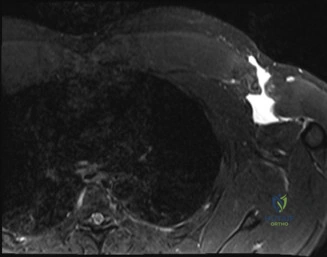
The same 29-year-old male presents with suspected pectoralis major muscle rupture. Radiographs of the shoulder were normal. What is the most appropriate next step in management?
Explanation
Correct Answer: C
While pectoralis major muscle (PMM) injuries are primarily diagnosed clinically, Magnetic Resonance Imaging (MRI) is the imaging modality of choice to evaluate the extent and location of a PMM tendon injury. MRI provides excellent soft tissue detail, allowing for assessment of the tear type (partial vs. complete), location (musculotendinous junction, tendinous insertion, muscle belly), and degree of retraction, which is crucial for surgical planning. Ultrasound is a reasonable alternative, particularly to avoid surgical delay, but it is highly user-dependent and may not provide the comprehensive detail of an MRI. Computed tomography (CT) is not ideal for soft tissue evaluation. Further radiographic evaluation of the humerus or contralateral shoulder is unlikely to provide additional diagnostic information regarding the PMM injury, as initial radiographs of the injured shoulder were already obtained and are often normal in these cases, primarily looking for bony avulsions.
Question 3
After evaluating the MRI, the patient is diagnosed with a complete rupture of the pectoralis major tendon. He is a young, active patient. What is the recommended first step in management?
Explanation
Correct Answer: A
For a young, active patient with a complete pectoralis major muscle (PMM) rupture, surgical repair is generally indicated to restore strength and function. However, immediate surgical intervention is not typically required. The first step in management, regardless of the definitive treatment plan, should be rest, ice, compression, and pain control (RICE). Sling immobilization in an adducted and internally rotated position helps to minimize tension on the torn tendon and prevent further retraction. While there is no absolute consensus on the ideal timing for repair, delaying surgery for 4 to 8 weeks allows for the acute swelling and ecchymosis to subside, which can facilitate surgical dissection and reduce complications. Options B and D risk further tendon retraction. Option C represents a nonoperative protocol, which is generally reserved for elderly or low-demand patients, or partial/muscle belly ruptures. Option E, immediate surgery, is usually not necessary and can be complicated by acute swelling and bleeding.
Question 4
All of the following are reported complications of operative management of a pectoralis major muscle injury, EXCEPT?
Explanation
Correct Answer: B
Numbness in the distribution of C6 has not been reported as a complication of pectoralis major muscle (PMM) injury repair. The C6 dermatome primarily covers the lateral forearm, thumb, and index finger. During surgical repair of a PMM rupture, the nerves most at risk are the lateral and medial pectoral nerves, which innervate the pectoralis muscles. Re-rupture of the tendon is a known complication, reported as high as 7.7%. Postoperative infection is a significant concern due to the location in the axillary area, which has a higher bacterial burden. Both heterotopic ossification and hematoma are also recognized complications following operative management of PMM injuries.
Question 5
A 50-year-old, right-hand-dominant female presents to clinic with posterior right shoulder pain and sometimes a loud noise while using her right upper extremity for overhead activities. Her pain is concentrated over the superomedial border of her scapula, but she also says her pain is underneath her shoulder blade. What is most bothersome is the fact that she is unable to brush her hair because of the discomfort she experiences. She reports that it started as only noise several years prior, but over the last several months she has developed debilitating pain with overhead activities. She works as a salon hair stylist and denies a history of trauma to her right upper extremity.
Which of the following is the most likely diagnosis?
Explanation
Correct Answer: E
The patient's history is highly characteristic of scapulothoracic bursitis, also known as snapping scapula syndrome. Key features include the long-standing history of a 'loud noise' (crepitus) preceding the onset of pain, pain concentrated over the superomedial border of the scapula and underneath the shoulder blade, and exacerbation with overhead activities (e.g., brushing hair, working as a hair stylist). Scapulothoracic crepitus can lead to symptomatic bursitis over time. Impingement syndrome, rotator cuff tendinitis, and supraspinatus tears typically present with pain in the anterior or lateral shoulder, often without the prominent 'snapping' or 'noise' component, and are less likely to localize pain specifically to the superomedial scapular border. Suprascapular nerve entrapment would primarily cause weakness and atrophy of the supraspinatus and infraspinatus muscles, which is not described as the primary complaint in this case.
Question 6
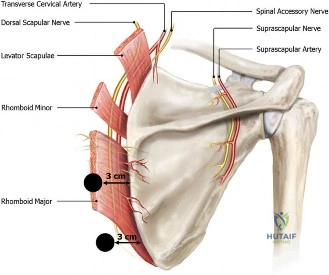
The patient's symptoms fail to improve after 6 months of conservative management. Radiographs and a three-dimensional CT scan were obtained, revealing an anterior “horn-like” projection at the superomedial angle of the scapula. Surgical intervention is planned using a modified mini-open approach with arthroscopy-assisted bursectomy. Portals are placed 3 cm medial to the medial scapular border.
Which structure(s) are avoided with this portal placement?
Explanation
Correct Answer: C
The dorsal scapular artery and nerve are critical structures that run beneath the rhomboid minor and major muscles, approximately 1 to 2 cm medial to the medial scapular border. Therefore, placing portals 3 cm medial to the medial scapular border is a technique designed to safely avoid injury to these neurovascular structures. The long thoracic nerve is located more laterally and is rarely endangered unless dissection extends too far laterally. The suprascapular nerve and spinal accessory nerve are typically at risk if portals are placed superior to the scapular spine. The deep branch of the transverse cervical artery becomes the dorsal scapular artery, so avoiding the dorsal scapular artery also implies avoiding its direct precursor in this region.
Question 7
A superomedial scapular resection as well as bursectomy is performed. While dissecting laterally, the suprascapular notch becomes visible in the operative field. What structure runs superficial to the transverse scapular ligament?
Explanation
Correct Answer: D
This is a classic anatomical relationship tested in orthopedic surgery. The suprascapular artery runs superficial (or over) the transverse scapular ligament, while the suprascapular nerve travels deep (or under) the ligament, through the suprascapular notch. This anatomical arrangement is often remembered by the mnemonic 'Army over Navy' (Artery over Nerve). The transverse cervical artery is a more proximal vessel, and its deep branch becomes the dorsal scapular artery, which is not directly associated with the suprascapular notch in this manner. The spinal accessory nerve and long thoracic nerve are not closely associated with the transverse scapular ligament or suprascapular notch.
Question 8
A 42-year-old female presents to the office for follow up after sustaining a minimally displaced radial head fracture 3 months prior. She states she was initially treated in long-arm splint by the ER and did not follow up with an orthopaedic surgeon until now. Per her report, she removed the splint 4 weeks after the injury, but did not move her elbow due to pain. She now has no pain but is unable to reach that hand to her face or head. The remaining history is significant for previous ulnar nerve surgery for which she is unable to provide details. On physical examination, her upper extremity is normal except for limited flexion/extension, measured to be 80 to 50 degrees by goniometer. In addition, she has a well-healed surgical incision about the medial elbow, consistent with a previous surgery on her ulnar nerve. Her images are shown.
What is the diagnosis?

Explanation
Correct Answer: A
This patient presents with an 'early post-traumatic intrinsic joint contracture.' The term 'early' is defined as within 6 months of the injury; this patient is 3 months post-injury. 'Intrinsic' causes of elbow stiffness refer to problems within the joint itself, such as articular incongruity, loose bodies, or severe osteoarthritis. In this case, the minimally displaced radial head fracture, even if healed, can lead to subtle incongruity or altered joint mechanics contributing to the stiffness. The prolonged immobilization and subsequent lack of motion due to pain also contribute. 'Extrinsic' causes involve structures outside the joint, such as capsular tightness, muscle contracture, heterotopic ossification, or skin contractures. While capsular tightness is likely present, the primary underlying cause stemming from the intra-articular fracture classifies it as intrinsic. Given the timeframe, it is not 'late' (greater than 6 months), and while there may be extrinsic components, the initial classification based on the radial head fracture points to an intrinsic cause.
Question 9
The 42-year-old female with an early post-traumatic intrinsic joint contracture of the elbow, 3 months post-radial head fracture, has limited flexion/extension (80 to 50 degrees). What is the preferred first line of treatment at this time?
Explanation
Correct Answer: C
For most cases of post-traumatic elbow stiffness, especially within the early timeframe (first 6 months), daily supervised physical therapy combined with static or dynamic progressive splinting is the preferred first line of treatment. Significant gains in elbow motion can be achieved within the first 3 to 6 months of initiating this conservative regimen, and improvement can continue for up to a year. If the contracture is primarily due to capsular tightness, operative management may not even be required. Manipulation under anesthesia (A) or surgical releases (B, D) are typically reserved for cases that fail an adequate trial of conservative therapy. Serial casting (E) can be part of conservative management but is often combined with or follows intensive physical therapy.
Question 10
If surgical intervention is warranted for the 42-year-old female with a stiff elbow, and she has a limitation of elbow flexion of 90 to 100 degrees, which of the following structures needs to be prophylactically addressed when performing an osteocapsular release?
Explanation
Correct Answer: A
Prophylactic treatment of the ulnar nerve (typically decompression or transposition) should be performed before an osteocapsular release in patients with significant elbow stiffness, especially if flexion is limited to 90-100 degrees or less. Anatomic studies have demonstrated that the cubital tunnel significantly decreases in size with elbow flexion greater than 90 degrees, leading to a corresponding increase in pressure on the ulnar nerve. After an osteocapsular release, the elbow's range of motion, particularly flexion, is expected to improve. This increased flexion can place the ulnar nerve under greater tension or compression, potentially exacerbating pre-existing neuropathy or inducing new symptoms. Given the patient's history of previous ulnar nerve surgery, the nerve is already vulnerable, making prophylactic management even more critical. The other structures listed are important for elbow stability or anatomy but are not typically prophylactically addressed in the same manner to prevent iatrogenic nerve compression from increased range of motion.
Question 11
A 68-year-old male with a history of essential hypertension undergoes an elective total knee arthroplasty. On post-operative day 0, his blood pressure is persistently 190/100 mmHg despite adequate pain control. He is alert, oriented, and denies chest pain or shortness of breath. His urine output is 50 mL/hr. What is the most appropriate initial management strategy?
Explanation
Correct Answer: A
Acute post-operative hypertension (BP >180/110 or >160/90 with risk factors/symptoms) requires prompt management to prevent complications such as myocardial ischemia, stroke, or surgical site hematoma. IV Labetalol is an excellent first-line agent for rapid blood pressure control in this setting, as it offers both alpha and beta-adrenergic blockade, reducing systemic vascular resistance and heart rate. Oral Nifedipine is typically used for less acute control. Increasing IV fluids would likely exacerbate hypertension in an euvolemic patient. While an ECG and enzymes are important if symptoms suggestive of cardiac ischemia were present, they are not the immediate management for asymptomatic hypertension. Reassurance is insufficient for such elevated blood pressure.
Question 12
A 35-year-old male presents to the emergency department after a high-speed motor vehicle collision with a Glasgow Coma Scale of 14, an open tibia fracture, and a clinically unstable pelvis on examination. His blood pressure is 80/40 mmHg, heart rate is 130 bpm, and respiratory rate is 26 bpm. He is pale and diaphoretic. What is the MOST critical immediate intervention after establishing airway and breathing?
Explanation
Correct Answer: B
In a hypotensive trauma patient with a clinically unstable pelvis, immediate application of a pelvic binder is a critical life-saving intervention. An unstable pelvic fracture can lead to massive hemorrhage from venous plexuses and arterial injury, and external compression can significantly reduce blood loss. While fluid resuscitation (crystalloids, blood products), TXA, and diagnostic exams (FAST) are all crucial components of trauma management, controlling the source of hemorrhage from the pelvis takes immediate precedence in this scenario to stabilize the patient's hemodynamics. Rapid IV access and fluid infusion should occur concurrently.
Question 13
A 72-year-old female undergoes a total hip arthroplasty. On post-operative day 1, she develops new-onset confusion, headache, and nausea. Labs reveal a serum sodium (Na+) of 122 mEq/L, serum osmolality of 250 mOsm/kg, and urine osmolality of 480 mOsm/kg. She has received 4 liters of D5 0.45% Normal Saline intravenously since surgery. Her physical exam is notable for euvolemia. What is the most likely cause of her hyponatremia?
Explanation
Correct Answer: B
This patient's presentation with euvolemic hyponatremia (Na+ 122 mEq/L), inappropriately concentrated urine (urine osmolality 480 mOsm/kg, which is >100 mOsm/kg in the setting of hyponatremia), and a relatively low serum osmolality (250 mOsm/kg) in the post-operative setting is highly suggestive of SIADH. Surgical stress, pain, and certain medications (e.g., opioids) can all stimulate ADH release. The administration of hypotonic fluids (D5 0.45% NS) further exacerbates the condition. CSW typically presents with hypovolemia. Hypovolemic hyponatremia would show signs of dehydration. Hyperglycemic pseudohyponatremia would be accompanied by significant hyperglycemia. Primary polydipsia would result in dilute urine (urine osmolality <100 mOsm/kg).
Question 14
A 25-year-old male suffers a severe crush injury to his leg after an industrial accident. On arrival at the ED, his BP is 100/60 mmHg, HR 110 bpm. Labs show K+ 6.2 mEq/L, Cr 2.5 mg/dL, and a significant myoglobinuria. What is the most immediate life-threatening electrolyte abnormality to address?
Explanation
Correct Answer: C
Severe crush injuries lead to rhabdomyolysis, which causes the release of intracellular contents into the bloodstream. Hyperkalemia is a critical and potentially life-threatening complication due to its direct effects on cardiac electrical stability, leading to arrhythmias. While hypocalcemia, hyperphosphatemia, and metabolic acidosis are also common in rhabdomyolysis, hyperkalemia poses the most immediate threat to life and requires urgent treatment (e.g., calcium gluconate for cardiac stabilization, insulin/glucose, beta-agonists, dialysis). The question asks for the most immediate life-threatening electrolyte, which is hyperkalemia.
Question 15
During total knee arthroplasty under spinal anesthesia, a 75-year-old patient's blood pressure drops to 70/40 mmHg. Heart rate is 50 bpm. The patient is well-hydrated preoperatively. What is the most appropriate initial pharmacologic intervention?
Explanation
Correct Answer: B
Spinal anesthesia often causes hypotension and bradycardia due to sympathetic blockade. Phenylephrine, a pure alpha-1 adrenergic agonist, causes peripheral vasoconstriction, effectively raising blood pressure without significantly increasing heart rate (which is already low). Epinephrine and Norepinephrine are potent vasopressors and inotropes, typically reserved for more profound or refractory shock. Atropine is useful for bradycardia but does not directly address the hypotension due to vasodilation. Labetalol would worsen both hypotension and bradycardia.
Question 16
A 60-year-old male with chronic back pain presents for elective lumbar laminectomy. Pre-operatively, his home medications include Lisinopril. On the morning of surgery, his BP is 155/95 mmHg. What is the most appropriate management of his Lisinopril on the day of surgery?
Explanation
Correct Answer: C
ACE inhibitors (like Lisinopril) are typically held on the day of surgery due to their potential to cause refractory hypotension under anesthesia, especially with spinal or epidural blocks. While some studies suggest continuing them, the current consensus for elective surgery usually leans towards holding them. The blood pressure should be monitored, and if dangerously high, an alternative short-acting antihypertensive (e.g., IV Labetalol or Hydralazine) can be administered. Re-initiating post-operatively when the patient is stable is generally safe. Taking it as usual carries risk. Administering an IV beta-blocker might be an option for acute hypertension but not the standard management for holding an ACEi. Half-dosing does not eliminate the risk.
Question 17
A 29-year-old male with a femur fracture undergoes intramedullary nailing. During reaming, the anesthesiologist observes a sudden decrease in SpO2, hypotension (BP 70/40 mmHg), and an increase in end-tidal CO2. The surgical field is free of significant bleeding. What is the most likely cause?
Explanation
Correct Answer: A
Fat embolism syndrome (FES) is a classic complication of long bone fractures, particularly during intramedullary reaming, where marrow contents are forced into the circulation. The triad of respiratory insufficiency, neurological symptoms, and petechial rash is characteristic, but acute intraoperative FES can manifest as sudden hypoxemia, hypotension, and an increase in end-tidal CO2. This is due to mechanical obstruction and chemical irritation of the pulmonary vasculature by fat globules. Pulmonary embolism (thrombotic) usually doesn't have the same acute increase in ETCO2, and is less common acutely during reaming. Local anesthetic toxicity typically presents with CNS excitation or depression, and/or cardiovascular collapse with wide QRS or arrhythmias. Venous air embolism is also a possibility but often occurs earlier in the case, and ETCO2 changes can vary. Pneumothorax would cause hypoxemia and hypotension but not typically an increase in ETCO2 unless it led to profound hypoventilation.
Question 18
A 55-year-old female with a known history of severe rheumatoid arthritis and chronic steroid use is scheduled for a total wrist arthroplasty. Her baseline blood pressure is 110/70 mmHg. What is a critical perioperative consideration regarding her steroid regimen?
Explanation
Correct Answer: C
Patients on chronic corticosteroid therapy (especially at doses equivalent to prednisone >5 mg/day for >3 weeks) are at risk of adrenal insufficiency during surgical stress. The hypothalamic-pituitary-adrenal (HPA) axis can be suppressed, preventing an adequate endogenous cortisol response. Therefore, a 'stress dose' of corticosteroids (e.g., hydrocortisone) is crucial perioperatively to prevent adrenal crisis, which can manifest as hypotension, hypoglycemia, and shock. Discontinuing or decreasing the dose without replacement would be dangerous. Switching to inhaled steroids is irrelevant for systemic stress response. Monitoring for hyperglycemia is important but secondary to preventing adrenal crisis.
Question 19
A 68-year-old male post-op total hip arthroplasty develops delirium and his serum sodium is 160 mEq/L. He is hypovolemic with a urine output of 180 mL/hr, urine osmolality 150 mOsm/kg. His blood glucose is 120 mg/dL. What is the appropriate rate of sodium correction for this hypernatremia?
Explanation
Correct Answer: B
Correction of hypernatremia should be gradual to prevent cerebral edema. A rapid decrease in serum sodium can cause water to shift into brain cells, leading to cerebral edema, seizures, and neurological damage. The general recommendation is to decrease serum sodium by no more than 10-12 mEq/L over the first 24 hours, and then by 18 mEq/L per 48 hours, or 0.5 mEq/L/hour. Rapid correction within 6 hours or by 20-24 mEq/L in 24 hours is too aggressive. The patient is symptomatic (delirium), requiring correction. Correcting with D5W at 500 mL/hr is too rapid and does not account for the gradual nature of correction.
Question 20
During cementation of a prosthetic component in a total hip arthroplasty, the patient's blood pressure drops acutely to 70/40 mmHg, and oxygen saturation decreases to 88%. What is the most likely cause?
Explanation
Correct Answer: B
Bone cement implantation syndrome (BMIS) is a well-recognized complication during cemented orthopedic procedures, particularly total hip arthroplasty. It is triggered by the absorption of bone cement monomers and release of vasoactive substances and microemboli (fat, air, marrow, cement) into the circulation, especially during reaming, femoral preparation, and cement pressurization. BMIS can manifest as sudden hypotension, hypoxemia, pulmonary hypertension, and cardiac arrhythmias, leading to cardiovascular collapse. While fat embolism syndrome is related, BMIS specifically encompasses the broader constellation of cardiopulmonary changes during cementation. The other options are less likely to occur precisely during cementation.
Question 21
A 68-year-old female presents after a fall on an outstretched hand (FOOSH) with a 'dinner fork' deformity of her right wrist. Radiographs confirm a dorsally displaced, dorsally angulated, comminuted distal radius fracture with an associated ulnar styloid fracture. Initial closed reduction under hematoma block achieves reasonable alignment, but post-reduction radiographs show a residual dorsal tilt of 15 degrees, radial shortening of 4 mm, and a positive ulnar variance of 2 mm. The fracture extends into the articular surface. Which of the following is the most significant indication for surgical intervention in this patient?
Explanation
Correct Answer: D
The most significant indication for surgical intervention in this scenario is the persistent dorsal tilt and radial shortening after reduction. While comminution, age, and ulnar styloid fracture are relevant factors, residual displacement parameters (dorsal tilt > 10 degrees, radial shortening > 3 mm) after initial attempts at closed reduction signify an unstable fracture that is likely to lose reduction, leading to malunion and functional impairment. These unstable parameters typically mandate surgical stabilization to restore and maintain anatomical alignment, preventing complications like pain, decreased range of motion, and post-traumatic arthritis. An ulnar styloid fracture alone is rarely an absolute indication unless it significantly contributes to DRUJ instability, which is not explicitly stated as the primary driver here. Comminution contributes to instability but the resultant unacceptable alignment after reduction is the direct surgical trigger.
Question 22
Regarding the surgical management of unstable Colles fractures with volar locking plates, which anatomical landmark is crucial to avoid hardware impingement on the flexor tendons and potential rupture?
Explanation
Correct Answer: C
The volar watershed line is a critical anatomical landmark in volar plating of distal radius fractures. Plates placed distal to this line, or with screws protruding distally, risk irritation and rupture of the flexor tendons, particularly the flexor pollicis longus (FPL). The watershed line represents the ridge where the volar capsule and ligaments attach, marking the safe zone for plate placement proximally. Lister's tubercle is on the dorsal aspect, the pronator quadratus covers the plate proximally and protects tendons, but proper plate positioning relative to the articular surface, guided by the watershed line, is paramount for preventing distal tendon impingement.
Question 23
A 45-year-old construction worker sustains a highly comminuted, intra-articular Colles fracture (Frykman Type IV). After closed reduction, radiographs show significant residual articular step-off (>2mm) and metaphyseal comminution with loss of radial height. He has no neurovascular deficits. What is the most appropriate definitive management strategy?
Explanation
Correct Answer: C
For a highly comminuted, intra-articular distal radius fracture with significant articular step-off and metaphyseal comminution in a relatively young, active patient, ORIF with a volar locking plate is generally considered the gold standard. A volar locking plate provides rigid fixation, allows for accurate restoration of articular congruence, and permits early mobilization, which is crucial for functional recovery. External fixation alone might not adequately reduce and maintain articular fragments, and K-wires are often insufficient for highly comminuted or intra-articular patterns. Cast immobilization would predictably result in malunion and severe functional deficit given the instability and articular involvement.
Question 24
Which of the following is NOT typically considered a stable parameter after closed reduction of a Colles fracture?
Explanation
Correct Answer: D
An articular step-off of 3 mm is NOT considered a stable or acceptable parameter. Generally, an articular step-off or gap of >2 mm is considered unstable and an indication for surgical management, especially in active patients, due to the high risk of post-traumatic arthritis. Radial inclination of 22 degrees, volar tilt of 5 degrees (neutral to slight volar is acceptable for Colles), radial length difference of 2 mm (usually <3mm difference is acceptable), and ulnar variance of 0 mm (neutral) are all generally within acceptable post-reduction radiographic parameters for stable Colles fractures.
Question 25
A 72-year-old patient undergoes closed reduction and casting for a Colles fracture. Three weeks post-reduction, they develop increasing pain, swelling, skin discoloration, and temperature changes in the affected hand, out of proportion to the injury. Active and passive range of motion of the digits is severely limited. What is the most likely diagnosis?
Explanation
Correct Answer: D
The constellation of symptoms including increasing pain, swelling, skin discoloration, temperature changes (autonomic dysfunction), and severely limited digital motion, out of proportion to the injury and occurring weeks after reduction, is highly suggestive of Complex Regional Pain Syndrome (CRPS) Type I, also known as Reflex Sympathetic Dystrophy (RSD). This condition is a common complication after distal radius fractures. Compartment syndrome is an acute emergency, typically occurring within hours to days, characterized by severe pain with passive stretching and potentially paresthesias and pallor, which is not the typical presentation here. Median nerve compression usually presents with specific sensory and motor deficits. EPL rupture causes a specific loss of thumb extension, and ulnar styloid nonunion would primarily cause focal pain and possibly DRUJ instability, not generalized hand symptoms.
Question 26
Which median nerve symptom is most common in the acute phase following a Colles fracture?
Explanation
Correct Answer: C
In the acute phase following a Colles fracture, compression or contusion of the median nerve at the carpal tunnel level is common due to swelling and hematoma. This typically presents as paresthesia (numbness and tingling) in the median nerve distribution: the thumb, index finger, middle finger, and radial half of the ring finger. Thenar muscle atrophy is a sign of chronic median nerve compression. Sensory loss in the ulnar digits indicates ulnar nerve involvement. Wrist drop indicates radial nerve palsy. Tinel's sign over the cubital tunnel relates to ulnar nerve compression at the elbow.
Question 27
What is the primary goal of surgical fixation of a Colles fracture with a volar locking plate?
Explanation
Correct Answer: C
The primary goal of surgical fixation, particularly with a volar locking plate, for an unstable Colles fracture is to restore anatomical alignment (radial length, inclination, and volar tilt) and articular congruence (if intra-articular), and to provide sufficient stability to allow for early range of motion of the wrist and digits. Early mobilization is critical to prevent stiffness, promote cartilage healing, and improve functional outcomes. While other options might be secondary benefits or unrelated, restoring anatomy and facilitating early motion are paramount.
Question 28
Which classification system for distal radius fractures emphasizes the involvement of the radiocarpal and radioulnar joints?
Explanation
Correct Answer: B
The Frykman classification system is widely used for distal radius fractures and is based on the involvement of the radiocarpal and radioulnar joints (articular vs. extra-articular, and presence/absence of ulnar styloid fracture). The AO classification is more complex and describes fracture patterns by location (metaphyseal), articular involvement (extra-articular, partial articular, complete articular), and comminution. Gartland and Werley primarily assess outcome. Universal classification is another system that considers similar parameters as Frykman. Fernandez classification is based on the mechanism of injury and fracture morphology.
Question 29
A common late complication of a malunited Colles fracture with significant dorsal angulation and radial shortening is:
Explanation
Correct Answer: A
A common late complication of a malunited Colles fracture, particularly with significant dorsal angulation, is rupture of the Extensor Pollicis Longus (EPL) tendon. The sharp dorsal prominence of the malunited distal radius can cause attrition and eventual rupture of the EPL tendon as it traverses Lister's tubercle. Avascular necrosis of the scaphoid is typically associated with scaphoid fractures. Acute carpal tunnel syndrome and compartment syndrome are early complications. Ulnar nerve palsy is less directly related to Colles malunion itself.
Question 30
When performing closed reduction of a Colles fracture, what is the correct sequence of maneuvers after adequate anesthesia?
Explanation
Correct Answer: C
The classic sequence for closed reduction of a Colles fracture involves: 1. Disimpaction and traction (to restore length and separate fragments), 2. Exaggeration of deformity (dorsiflexion) to unlock fragments, followed by volar translation, 3. Supination (to correct pronation of the distal fragment, which is common with dorsal displacement), 4. Ulnar deviation (to restore radial inclination), and 5. Palmar flexion (to correct dorsal angulation and maintain reduction). Therefore, traction, supination, ulnar deviation, and flexion are the key components after disimpaction.
Question 31
A 62-year-old male undergoes a total hip arthroplasty (THA) via a direct anterior approach. Postoperatively, he complains of numbness and burning pain over the lateral aspect of his thigh. Physical examination reveals diminished sensation in this distribution. Motor strength is intact. Which of the following nerves was most likely injured during the procedure?
Explanation
Correct Answer: C
The patient's symptoms of numbness and burning pain over the lateral aspect of the thigh, without motor weakness, are classic for meralgia paresthetica, which is caused by compression or injury to the lateral femoral cutaneous nerve (LFCN). The direct anterior approach (DAA) to the hip is known to have a higher risk of LFCN injury due to the nerve's superficial course and its proximity to the surgical incision and retractors. While the DAA is associated with a lower dislocation rate and potentially faster recovery, this specific nerve injury is a recognized complication. The sciatic nerve (A) injury would typically cause weakness in the posterior thigh and leg muscles, and sensory loss in the posterior leg and foot. The femoral nerve (B) injury would cause weakness in hip flexion and knee extension, and sensory loss over the anterior thigh. The obturator nerve (D) injury would cause weakness in hip adduction and sensory loss over the medial thigh. The superior gluteal nerve (E) injury would cause weakness in hip abduction (Trendelenburg gait).
Question 32
A 6-year-old boy presents with a 3-month history of a painless limp and mild right hip pain, worse with activity. Physical examination reveals limited internal rotation and abduction of the right hip. Radiographs show flattening and increased density of the right femoral epiphysis. What is the most appropriate initial management strategy for this condition?
Explanation
Correct Answer: C
This clinical presentation and radiographic findings are classic for Legg-Calvé-Perthes disease (LCPD), which is avascular necrosis of the femoral head in children. The goal of treatment for LCPD, especially in a 6-year-old with significant involvement, is to contain the femoral head within the acetabulum to maintain its spherical shape during the revascularization and healing phases. This 'containment' can be achieved non-operatively with bracing (e.g., Scottish Rite brace, Petrie cast) or operatively with osteotomies (femoral or pelvic) if non-operative measures fail or are not suitable. Observation (B) alone is typically reserved for very young children (under 6) with minimal involvement. Core decompression (A) is for adult avascular necrosis. Total hip arthroplasty (D) is a salvage procedure for end-stage arthritis, not initial management for LCPD. Anti-inflammatory medications and physical therapy (E) are adjunctive for symptom management but do not address the underlying pathology or prevent deformity.
Question 33
A 48-year-old male presents to the emergency department with acute onset severe low back pain, bilateral leg weakness, saddle anesthesia, and new-onset urinary retention. He reports a history of chronic low back pain but these symptoms are new and rapidly progressing. What is the most appropriate immediate diagnostic and management step?
Explanation
Correct Answer: B
The patient's presentation with acute severe low back pain, bilateral leg weakness, saddle anesthesia, and urinary retention is highly suggestive of Cauda Equina Syndrome (CES). CES is a surgical emergency requiring urgent diagnosis and decompression to prevent permanent neurological deficits, particularly bowel and bladder dysfunction. The most appropriate immediate step is an urgent MRI of the lumbar spine to confirm the diagnosis and identify the level of compression, followed by emergent surgical decompression. Delay in treatment significantly worsens the prognosis. Corticosteroids (A) are not the primary treatment for CES. Physical therapy (C), epidural injections (D), and nerve conduction studies (E) are inappropriate and would cause critical delays in a rapidly progressing neurological emergency.
Question 34
A 7-year-old child falls onto an outstretched hand, sustaining an injury to the elbow. Radiographs show a fracture of the proximal ulna with an associated anterior dislocation of the radial head. Which of the following classifications best describes this injury pattern?
Explanation
Correct Answer: C
The description of a fracture of the proximal ulna with an associated dislocation of the radial head is the classic definition of a Monteggia fracture-dislocation. This injury pattern is crucial to recognize because the radial head dislocation can be easily missed if only the ulnar fracture is focused on. The Bado classification further categorizes Monteggia injuries based on the direction of radial head dislocation and the ulnar fracture pattern. Gartland Type III (A) refers to a displaced supracondylar humerus fracture. Salter-Harris Type II (B) is a physeal fracture involving the metaphysis. Galeazzi fracture-dislocation (D) involves a fracture of the distal radius with associated dislocation of the distal radioulnar joint. Essex-Lopresti injury (E) is a comminuted radial head fracture with disruption of the interosseous membrane and distal radioulnar joint dislocation.
Question 35
A 35-year-old male sustains a high-energy valgus injury to his knee in a motor vehicle accident. Radiographs show a comminuted fracture of the lateral tibial plateau with significant articular depression and widening. CT scan confirms a Schatzker Type VI fracture. Which of the following is the most appropriate definitive management?
Explanation
Correct Answer: C
A Schatzker Type VI tibial plateau fracture is a bicondylar fracture with dissociation of the metaphysis and diaphysis, often involving significant articular depression and comminution. These are high-energy injuries that typically require emergent open reduction and internal fixation (ORIF) with dual plating (medial and lateral) to restore articular congruity, mechanical alignment, and stability. Non-weight bearing and cast immobilization (A) are insufficient for such unstable and comminuted fractures. External fixation (B) might be used as a temporary measure for severe soft tissue injury (damage control orthopedics) but is not the definitive treatment for articular reconstruction. Knee arthrodesis (D) or unicompartmental knee arthroplasty (E) are salvage procedures for end-stage arthritis or specific unicompartmental disease, respectively, and are not indicated for acute, repairable fractures.
Question 36
A 55-year-old female presents with a long-standing, painful hallux valgus deformity that has failed conservative management including wider shoes and orthotics. Clinical examination reveals a severe deformity with a hallux valgus angle of 40 degrees and an intermetatarsal angle of 18 degrees. Radiographs confirm these measurements. Which of the following surgical procedures is most appropriate to address this deformity?
Explanation
Correct Answer: C
The patient presents with a severe hallux valgus deformity (HVA 40 degrees, IMA 18 degrees). For severe deformities, especially with a large intermetatarsal angle, a proximal metatarsal osteotomy or a fusion procedure is typically required to achieve adequate correction and stability. The Lapidus procedure, which involves fusion of the first metatarsocuneiform joint, is highly effective for correcting severe hallux valgus and reducing the intermetatarsal angle. Simple bunionectomy (A) is an exostectomy and does not correct the underlying bony deformity. A Chevron osteotomy (B) is a distal metatarsal osteotomy, suitable for mild to moderate deformities. Keller arthroplasty (D) is a resection arthroplasty, typically reserved for older, low-demand patients with severe arthritis, as it can lead to instability and transfer metatarsalgia. Arthrodesis of the first MTP joint (E) is a salvage procedure for severe arthritis or failed previous surgeries, not typically for primary hallux valgus correction in an active patient.
Question 37
A 14-year-old male presents with localized pain and swelling in his right femur for several months, accompanied by intermittent fever and weight loss. Radiographs show a lytic lesion in the diaphysis with a characteristic 'onion skin' periosteal reaction. Biopsy reveals small, round, blue cells. Which of the following is the most likely diagnosis?
Explanation
Correct Answer: B
The clinical presentation (adolescent, pain, swelling, systemic symptoms like fever and weight loss), radiographic findings (lytic diaphyseal lesion with 'onion skin' periosteal reaction), and histological description (small, round, blue cells) are classic for Ewing's sarcoma. Ewing's sarcoma is a highly malignant bone tumor, often affecting the diaphysis of long bones or flat bones, and is characterized by a specific chromosomal translocation (most commonly t(11;22)). Osteosarcoma (A) typically presents with a 'sunburst' or Codman's triangle appearance and involves the metaphysis. Chondrosarcoma (C) is a cartilage-forming tumor, usually in older adults, with a different radiographic and histological appearance. Osteoid osteoma (D) is a benign tumor characterized by a small lucent nidus and surrounding sclerosis, with pain relieved by NSAIDs. Fibrous dysplasia (E) is a developmental anomaly, not a malignant tumor, and has a 'ground-glass' appearance on radiographs.
Question 38
A 40-year-old male with a history of an open tibia fracture 2 years ago, treated with intramedullary nailing, presents with persistent pain, swelling, and a chronic draining sinus tract over the fracture site. Radiographs show cortical thickening and lucencies around the nail. Laboratory studies reveal a mildly elevated ESR and CRP. What is the most appropriate management strategy?
Explanation
Correct Answer: C
This patient's presentation is classic for chronic osteomyelitis, likely associated with retained hardware from a previous open fracture. The persistent draining sinus, pain, swelling, and radiographic changes (cortical thickening, lucencies) indicate ongoing infection. The cornerstone of chronic osteomyelitis treatment, especially with hardware, is aggressive surgical debridement of all infected and necrotic bone and soft tissue, removal of the hardware (if the fracture is healed or stable enough), followed by a prolonged course of targeted intravenous antibiotics based on intraoperative cultures. Oral antibiotics alone (A) are insufficient for established chronic osteomyelitis with sequestrum and biofilm formation on hardware. Removal of the nail alone (B) without debridement will likely lead to recurrence. Hyperbaric oxygen therapy (D) can be an adjunct but is not a primary treatment. While repeat cultures (E) are important, they must be obtained intraoperatively from bone and tissue, not just the draining sinus, and surgical debridement is still paramount.
Question 39
A 22-year-old female collegiate soccer player sustains a non-contact injury to her right knee during a game, reporting a 'pop' and immediate swelling. She is unable to continue playing. On examination, she has a large effusion, limited range of motion due to pain, and a positive Lachman test. Which of the following associated injuries is most commonly seen with this type of injury?
Explanation
Correct Answer: C
The patient's history (non-contact 'pop', immediate swelling, inability to play) and physical exam (effusion, positive Lachman) are highly suggestive of an acute anterior cruciate ligament (ACL) rupture. ACL injuries are frequently associated with other intra-articular injuries. Meniscal tears, particularly of the lateral meniscus (e.g., ramp lesion, root tear) or medial meniscus, are the most common associated injuries, occurring in 50-70% of acute ACL ruptures. The 'unhappy triad' (ACL, MCL, medial meniscus) is a classic but less common combination than isolated ACL with meniscal tear. While MCL sprains (B) can occur, meniscal tears are more prevalent. PCL tears (A) are typically from direct posterior trauma. Patellar tendon ruptures (D) are less common and present with a different mechanism and physical exam. Osteochondral fractures (E) can occur but are less frequent than meniscal tears.
Question 40
A 78-year-old female with a well-fixed cementless total hip arthroplasty (THA) from 10 years ago falls and sustains a periprosthetic femur fracture. Radiographs show a spiral fracture extending from just below the lesser trochanter down the femoral shaft, with the femoral stem intact and stable within the proximal fragment. There is no evidence of stem loosening. According to the Vancouver classification, which type of fracture does this represent, and what is the most appropriate management?
Explanation
Correct Answer: B
The Vancouver classification is used for periprosthetic femur fractures around a THA stem. The fracture described is a spiral fracture below the lesser trochanter, with the femoral stem intact and stable within the proximal fragment, and no evidence of stem loosening. This fits the criteria for a Vancouver Type B1 fracture. Type B1 fractures are characterized by a fracture around or just below the stem, with a well-fixed stem. The most appropriate management for a Vancouver Type B1 fracture is open reduction and internal fixation (ORIF) using plates and screws (e.g., locking plates, cables) to stabilize the fracture while retaining the well-fixed stem. Type A fractures (A) are trochanteric fractures, typically managed with ORIF. Type B2 (C) fractures involve a loose stem, requiring stem revision. Type B3 (D) fractures involve a loose stem with significant bone loss, requiring extensive revision and often allograft. Type C fractures (E) are distal to the stem, managed with ORIF, but the description places the fracture around the stem.
Question 41
A 72-year-old male presents to the emergency department with acute right groin pain, disproportionate to physical examination findings, and a tender, non-reducible mass. He reports mild nausea but denies vomiting or obstipation. His past medical history includes a laparoscopic appendectomy 5 years ago. On abdominal CT, a small bowel loop is noted partially entrapped in a femoral hernia sac, with mural thickening and surrounding fat stranding. Which of the following best describes this hernia type?
Explanation
Correct Answer: C
The scenario describes a Richter hernia, characterized by the incarceration of only a portion of the circumference of the bowel wall. This explains the disproportionate pain, tenderness, and lack of complete obstructive symptoms (like vomiting or obstipation) often seen with complete lumen occlusion. Despite the partial involvement, Richter hernias carry a very high risk of strangulation and gangrene due to the tight constriction of the involved bowel segment. A Littre hernia involves a Meckel's diverticulum, an Amyand hernia involves the appendix, and a Spigelian hernia occurs through the Spigelian aponeurosis. A sliding hernia involves a viscus that forms part of the hernia sac wall, typically retroperitoneal organs like the colon or bladder.
Question 42
Regarding the pathophysiology of a Richter hernia, which statement is most accurate?
Explanation
Correct Answer: C
A Richter hernia is defined by the incarceration of only a portion of the circumference of the bowel wall, most commonly the anti-mesenteric border. This distinct feature means that the bowel lumen is not fully occluded, explaining why patients may not present with classic signs of complete bowel obstruction such as vomiting, abdominal distention, or obstipation. However, the partial entrapment still subjects the involved bowel segment to severe ischemic compromise, leading to a high risk of strangulation, necrosis, and perforation, often at an accelerated rate compared to other hernia types due to the intense pressure on a small area. It can occur in any hernia type, not exclusively incisional, and most commonly involves the small intestine.
Question 43
A 45-year-old male with a history of recurrent inguinal hernias presents with acute, localized pain and a tender, firm lump in his left groin. He reports mild discomfort but is able to pass flatus and has had a recent bowel movement. Vital signs are stable. Given the high index of suspicion for a Richter hernia, what is the most critical immediate concern regarding this patient's condition?
Explanation
Correct Answer: C
The most critical immediate concern with a suspected Richter hernia is the rapid progression to bowel strangulation and perforation. While complete bowel obstruction is less common due to the partial involvement of the bowel wall, the tight constriction of the incarcerated segment leads to rapid ischemia, necrosis, and perforation. This can quickly escalate to peritonitis, sepsis, and a life-threatening emergency. Electrolyte imbalance from vomiting is less likely given the absence of complete obstruction, and while a fascial defect is present, the immediate life-threatening complication is strangulation. Chronic pain is a long-term issue, not an immediate critical concern.
Question 44
An 80-year-old patient undergoing rehabilitation after a total hip arthroplasty develops new onset of localized lower abdominal pain and tenderness at a previous laparoscopic cholecystectomy incision site. She reports being able to pass gas but has some difficulty with defecation. Examination reveals a subtle, firm, tender lump. Given her age and recent surgery, an occult Richter hernia should be considered. What imaging modality would be most sensitive for initial diagnosis?
Explanation
Correct Answer: C
A CT scan of the abdomen and pelvis with intravenous contrast is the most sensitive and specific imaging modality for diagnosing a Richter hernia. It can clearly visualize the incarcerated bowel segment, assess for mural thickening, fat stranding, and signs of ischemia (lack of enhancement, pneumatosis), and rule out other causes of abdominal pain. Plain abdominal radiographs are poor for soft tissue detail and often normal in Richter hernias without complete obstruction. Ultrasound can be helpful but is operator-dependent and may miss deeper or subtle hernias. MRI is also highly detailed but generally less available for acute emergencies and offers no significant advantage over CT for initial diagnosis. A barium enema is for colon evaluation and not suitable for acute small bowel pathology like a Richter hernia.
Question 45
Which of the following clinical findings is *least* typical for a patient presenting with an early, uncomplicated Richter hernia?
Explanation
Correct Answer: B
Significant abdominal distention is least typical for an early, uncomplicated Richter hernia because, by definition, only a portion of the bowel wall is entrapped, meaning the bowel lumen is usually not completely obstructed. Patients often present with localized tenderness, a palpable mass (which may be subtle), and pain disproportionate to the seemingly benign findings. They may experience mild nausea but often do not have projectile vomiting and can typically pass flatus and stools, distinguishing it from a complete bowel obstruction. Abdominal distention would suggest a more advanced stage with paralytic ileus secondary to peritonitis or development of a complete obstruction, which is less common initially.
Question 46
A 68-year-old female presents with acute right groin pain radiating to the medial thigh, associated with a tender, irreducible mass. She has a history of multiple prior abdominal surgeries. Imaging suggests a Richter hernia in a femoral location. As an orthopedic surgeon, what is a crucial aspect of the initial management plan you would emphasize for this patient, considering her immediate risk?
Explanation
Correct Answer: C
For a suspected Richter hernia, especially one that is tender and irreducible, urgent general surgery consultation for surgical exploration is paramount. Richter hernias carry a very high risk of strangulation and bowel necrosis, making them a surgical emergency. Delay can lead to catastrophic consequences like bowel perforation, peritonitis, and sepsis. Physical therapy, NSAIDs, and MRI of the hip are appropriate for orthopedic conditions but would be dangerously delayed and incorrect for an acute surgical emergency like an incarcerated hernia. While manual reduction can be attempted for some incarcerated hernias, it is often difficult and potentially harmful (e.g., reduction en masse) in a suspected Richter hernia, especially with signs of ischemia or tenderness, and should only be considered under specific circumstances and surgical readiness.
Question 47
In a patient presenting with an incarcerated hernia, what feature specifically raises the suspicion for a Richter hernia over a complete lumen obstructing hernia?
Explanation
Correct Answer: B
The most distinguishing feature of a Richter hernia, especially in its early stages, is the lack of complete bowel obstruction symptoms, such as significant abdominal distention, vomiting, and obstipation. This is because only a portion of the bowel wall is entrapped, allowing the lumen to remain patent. Despite this, the constricted portion is highly prone to strangulation. Vomiting and obstipation are classic signs of complete bowel obstruction, which are less typical for an early Richter hernia. Palpable crepitus suggests gas in soft tissues, often from perforation. Systemic signs of sepsis indicate a very late and complicated stage, and air-fluid levels indicate obstruction, which, again, is often absent or delayed in a Richter hernia.
Question 48
Which of the following scenarios should raise the highest suspicion for a Richter hernia in a patient presenting to an orthopedic clinic?
Explanation
Correct Answer: B
The most concerning scenario for an orthopedic surgeon indicating a potential Richter hernia is a patient with acute onset of right anterior thigh pain and a palpable, tender, firm mass in the femoral triangle. This presentation strongly suggests a femoral hernia, a common site for Richter incarceration. The pain radiating to the thigh is characteristic of femoral or obturator hernias due to nerve irritation. The other options describe common orthopedic pathologies (hip OA, spinal stenosis, hamstring strain) or an uncomplicated hernia (child with reducible bulge) that are less likely to be a life-threatening Richter hernia. While chronic groin pain can be due to various causes, an acute, tender, irreducible mass significantly changes the urgency.
Question 49
Post-operatively, a patient who underwent reduction and repair of a Richter hernia should be monitored closely for which of the following complications specific to ischemic bowel?
Explanation
Correct Answer: C
Perforation of the reduced, previously ischemic bowel segment (known as 'reperfusion injury' or 'retained ischemic segment' complications) is a critical post-operative concern after Richter hernia repair, especially if the viability of the bowel was questionable or borderline during surgery. Even if the segment appears viable at the time of reduction, ongoing ischemia can lead to delayed necrosis and perforation. All other options (DVT, wound infection, urinary retention, PE) are general post-operative complications, but delayed perforation due to a compromised bowel segment is highly specific and dangerous after ischemic bowel events.
Question 50
What is the primary reason Richter hernias carry a higher mortality rate compared to typical incarcerated hernias that cause complete bowel obstruction?
Explanation
Correct Answer: B
The primary reason for higher mortality in Richter hernias is the delayed diagnosis. Because the bowel lumen is not completely obstructed, patients often do not experience the classic symptoms of complete obstruction (vomiting, abdominal distention, obstipation). This subtle presentation can lead to a delay in seeking medical attention and, consequently, a delay in diagnosis and surgical intervention. By the time the diagnosis is made, the incarcerated segment has often progressed to strangulation, necrosis, and perforation, leading to severe peritonitis and sepsis, significantly increasing morbidity and mortality. Richter hernias are not necessarily larger or more complex, do not always involve multiple loops, and can occur in various age groups. While pain can be disproportionate, it's not always less severe; rather, the type of symptoms (lack of obstruction) causes diagnostic delay.
Question 51
A 25-year-old male sustains a high-energy trauma resulting in a vertical, completely displaced femoral neck fracture (Pauwels type III). He is hemodynamically stable and has no other associated injuries. What is the most appropriate surgical management to minimize the risk of varus collapse?
Explanation
Question 52
Which of the following physical examination findings is considered most highly specific for the diagnosis of cervical myelopathy?
Explanation
Question 53
A 12-year-old obese boy presents with progressive left groin and knee pain. Radiographs demonstrate a stable slipped capital femoral epiphysis (SCFE). Which of the following is an established indication for prophylactic in situ pinning of the asymptomatic contralateral hip?
Explanation
Question 54
A 16-year-old female presents with knee pain and swelling. Radiographs reveal a 'sunburst' periosteal reaction in the distal femur. Biopsy confirms high-grade intramedullary osteosarcoma.
Based on the Huvos grading system, what percentage of tumor necrosis following neoadjuvant chemotherapy indicates a favorable prognosis?

Explanation
Question 55
A 65-year-old female undergoes a total hip arthroplasty utilizing a ceramic-on-ceramic bearing surface. At her 2-year follow-up, she complains of a loud, audible squeaking sound from her hip during normal gait. Which of the following factors is most strongly associated with this phenomenon?
Explanation
Question 56
A 22-year-old male falls onto an outstretched hand and sustains a nondisplaced waist fracture of the scaphoid. What is the primary source of blood supply to the proximal pole of the scaphoid?
Explanation
Question 57
A 25-year-old athlete sustains a severe midfoot injury during a football game. Weight-bearing radiographs reveal widening between the medial and middle cuneiforms and a 'fleck sign' at the base of the second metatarsal. What structure is avulsed to create this specific radiographic finding?
Explanation
Question 58
During fracture healing, endochondral ossification requires an intermediate cartilage template. Which of the following transcription factors is essential for driving the differentiation of mesenchymal stem cells into chondrocytes?
Explanation
Question 59
A 40-year-old male presents with a high-energy Schatzker VI tibial plateau fracture. During the initial evaluation, he complains of escalating leg pain, particularly with passive stretch of the hallux, and paresthesias in the first web space. What is the most appropriate next step in management?
Explanation
Question 60
A 25-year-old male sustains a high-energy Pauwels type III femoral neck fracture. To minimize the risk of avascular necrosis, surgical fixation should respect the primary blood supply to the femoral head. Which of the following vessels provides the majority of the blood supply to the adult femoral head?
Explanation
Question 61
A 22-year-old soccer player undergoes evaluation for a suspected ACL tear. During the pivot shift test, a clunk is felt as the knee is flexed past 20-30 degrees. Which anatomical structure is responsible for reducing the tibia during this maneuver?
Explanation
Question 62
An 11-year-old obese male presents with left groin pain and an obligatory external rotation of the hip during passive flexion. Radiographs confirm a slipped capital femoral epiphysis (SCFE). Prophylactic pinning of the contralateral asymptomatic hip is most strongly indicated in patients with which of the following underlying conditions?
Explanation
Question 63
A 19-year-old male falls onto an outstretched hand and sustains a fracture of the proximal pole of the scaphoid. He is counseled regarding the high risk of nonunion and avascular necrosis. The primary blood supply to the proximal pole of the scaphoid is derived from which of the following?
Explanation
Question 64
A 35-year-old male sustains a closed midshaft tibia fracture. Four hours post-injury, he complains of severe pain out of proportion to the injury. Which of the following pressure measurements is the most reliable threshold for diagnosing acute compartment syndrome and proceeding with four-compartment fasciotomies?
Explanation
Question 65
A 14-year-old boy presents with progressive knee pain and swelling. Radiographs reveal a destructive metaphyseal lesion of the distal femur with a "sunburst" periosteal reaction. Biopsy confirms osteosarcoma. Mutations in which of the following tumor suppressor genes are most strongly associated with the pathogenesis of this tumor?
Explanation
Question 66
A 65-year-old active female undergoes a primary total hip arthroplasty. To minimize wear, a ceramic-on-ceramic bearing surface is chosen. Which of the following is a recognized complication specifically associated with this bearing surface?
Explanation
Question 67
A 3-month-old female is being treated with a Pavlik harness for developmental dysplasia of the hip. At a follow-up visit, the mother notes that the child is no longer actively extending the knee on the treated side. This complication is most likely due to which of the following positioning errors?
Explanation
Question 68
A 45-year-old male recreational basketball player sustains an acute Achilles tendon rupture. He is discussing operative versus nonoperative management with his surgeon. Compared to nonoperative treatment with an early functional rehabilitation protocol, surgical repair is associated with which of the following outcomes?
Explanation
Question 69
A 21-year-old rugby player undergoes an MR arthrogram after recurrent anterior shoulder dislocations. The MRI demonstrates an anterior labral tear that is medially displaced and healed to the glenoid neck, with an intact anterior periosteum. What is the most likely diagnosis?
Explanation
Question 70
According to Perren's strain theory, primary bone healing occurs without callous formation under conditions of absolute stability. For primary bone healing to occur, the interfragmentary strain must be maintained below what percentage?
Explanation
Question 71
A 68-year-old female undergoes a total knee arthroplasty for severe valgus osteoarthritis. The surgeon plans a sequential lateral soft tissue release. Which of the following structures is the primary restraint to valgus instability when the knee is in 90 degrees of flexion?
Explanation
Question 72
A 32-year-old male is brought to the trauma bay after a motorcycle collision. Pelvic radiographs demonstrate widening of the pubic symphysis to 3.5 cm and widening of the anterior sacroiliac joints, consistent with an Anteroposterior Compression II (APC II) injury. Which of the following posterior pelvic ligaments remain intact in this injury pattern?
Explanation
Question 73
A 45-year-old female undergoes an open carpal tunnel release. To safely decompress the median nerve, the surgeon must be aware of the anatomical variations of the recurrent motor branch. What is the most common anatomical pathway of the recurrent motor branch of the median nerve in relation to the transverse carpal ligament?
Explanation
Question 74
A 55-year-old male presents with deteriorating handwriting, frequent dropping of objects, and a broad-based gait. On physical examination, flicking the distal phalanx of the middle finger results in reflexive flexion of the thumb and index finger. This clinical sign indicates pathology in which of the following anatomical locations?
Explanation
Question 75
A 9-year-old girl presents with pain and swelling in her diaphyseal femur. Radiographs show a permeative "onion-skin" lesion. A biopsy is sent for molecular testing. Which of the following chromosomal translocations is highly specific for the suspected diagnosis?
Explanation
Question 76
A 24-year-old football player sustains a hyperplantarflexion injury to his foot. Weight-bearing radiographs reveal widening of the interval between the first and second metatarsals. An injury to the Lisfranc ligament is suspected. What are the correct anatomical attachments of the Lisfranc ligament?
Explanation
Question 77
A 6-year-old boy falls from the monkey bars and sustains an extension-type supracondylar humerus fracture. Upon neurologic examination, he is unable to flex the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger. Which nerve has most likely been injured?
Explanation
Question 78
A 45-year-old male is involved in a high-speed motorcycle collision and sustains an APC-III pelvic ring injury. He is hemodynamically unstable upon arrival. Following application of a pelvic binder, his blood pressure remains 70/40 mmHg and his heart rate is 130 bpm. A FAST exam is negative. What is the most appropriate next step in management?
Explanation
Question 79
A 22-year-old collegiate football player undergoes a Latarjet procedure for recurrent anterior shoulder instability with significant glenoid bone loss. Postoperatively, he demonstrates weak elbow flexion and decreased sensation along the lateral aspect of his forearm. Which nerve was most likely injured during the procedure?
Explanation
Question 80
A 13-year-old obese male presents with acute-on-chronic left knee pain and an inability to bear weight. Radiographs confirm a slipped capital femoral epiphysis (SCFE). Which of the following is the most significant risk factor for the development of avascular necrosis (AVN) in this patient?
Explanation
Question 81
Which of the following best describes the mechanism of action of denosumab in the treatment of a giant cell tumor of bone?
Explanation
Question 82
A 68-year-old female presents with recurrent posterior dislocations following a primary total hip arthroplasty performed via a posterior approach. Radiographs demonstrate that the acetabular component is in 25 degrees of abduction and 0 degrees of anteversion. Which of the following is the most appropriate surgical management?
Explanation
Question 83
A 65-year-old male presents with deteriorating handwriting, difficulty buttoning his shirt, and gait clumsiness. Physical examination reveals a positive Hoffman's sign and hyperreflexia in both lower extremities. MRI of the cervical spine demonstrates multi-level spondylosis with severe cord compression and T2 signal hyperintensity in the spinal cord. What is the most appropriate management?
Explanation
Question 84
A 25-year-old male presents with persistent radial-sided wrist pain 8 months after a fall onto an outstretched hand. Radiographs reveal a scaphoid waist fracture nonunion with cystic changes and a "humpback" deformity. MRI confirms avascular necrosis of the proximal pole. What is the most appropriate surgical intervention?
Explanation
Question 85
A 15-year-old boy presents with progressive distal femur pain. Radiographs reveal a sunburst periosteal reaction and a permeative metaphyseal lesion. Biopsy confirms high-grade osteosarcoma. Which of the following represents the most appropriate treatment protocol?
Explanation
Question 86
A 35-year-old recreational basketball player feels a "pop" in his posterior ankle. Examination reveals a positive Thompson test and a palpable gap 4 cm proximal to the calcaneal insertion. He opts for non-operative management. Which of the following best describes the appropriate functional rehabilitation protocol?
Explanation
Question 87
A 42-year-old female sustains a high-energy Schatzker VI tibial plateau fracture. The limb is grossly swollen, and the patient has exquisite pain with passive stretch of the hallux. Stryker needle measurement reveals an anterior compartment pressure of 45 mmHg with a diastolic blood pressure of 60 mmHg. What is the next best step?
Explanation
None
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding abos-part-i-comprehensive-review-batch-93-1