ABOS Part I Orthopaedic Surgery Exam Review: Trauma, Fractures & Compartment Syndrome | Part 22144
Key Takeaway
This ABOS Part I Orthopaedic Trauma Review module offers 21 advanced multiple-choice questions mirroring ABOS Part I and AAOS OITE exams. It covers high-yield clinical cases in orthopaedic trauma, including acute compartment syndrome diagnosis and management, complex tibial fracture classification and surgical fixation (IM nailing), and critical postoperative care. Ideal for board preparation.
ABOS Part I Orthopaedic Surgery Exam Review: Trauma, Fractures & Compartment Syndrome | Part 22144
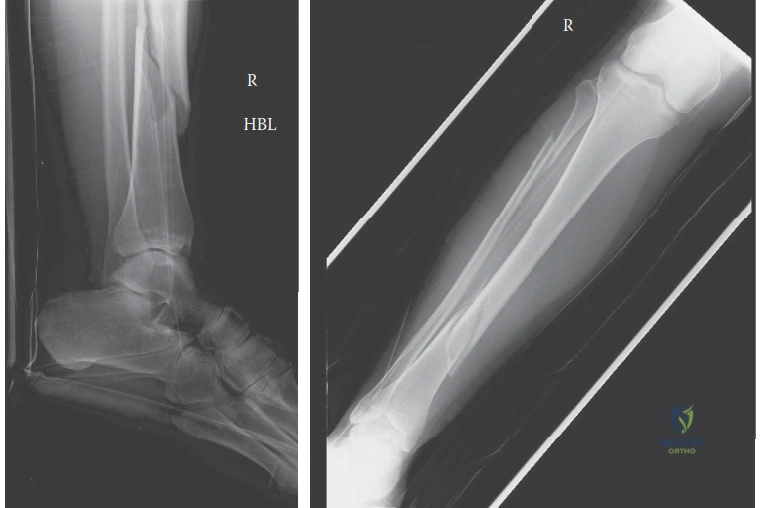
A 38-year-old male presents with the right lower extremity injury shown in the radiograph below, following a high-velocity motorcycle collision. His past medical history includes Type 2 Diabetes Mellitus (HbA1c 6.8%) and a 15 pack-year smoking history. The fracture is classified as AO/OTA 42-B3 with a Tscherne Grade 2 closed soft tissue injury. Given these factors, which of the following is the MOST significant long-term complication risk directly attributable to the patient's comorbidities and injury characteristics?

Correct Answer: C
The patient's comorbidities, Type 2 Diabetes Mellitus and a significant smoking history, are well-established risk factors for impaired fracture healing. Diabetes alters bone microarchitecture, impairs cellular responses to trauma, and causes microvascular disease, all of which compromise the angiogenic response critical for callus formation. Smoking induces profound peripheral vasoconstriction, reducing cutaneous and osseous blood flow, and carbon monoxide causes tissue hypoxia. This combination significantly elevates the risk of delayed union, nonunion, and surgical site infection, particularly in the watershed areas of the tibial diaphysis. Therefore, delayed union or nonunion is the most significant long-term complication directly attributable to these factors.
Option A (Acute compartment syndrome) is an acute, immediate complication, not a long-term one, and while the patient is at high risk due to the high-energy mechanism, it's not directly caused by his chronic comorbidities in the same way healing complications are.
Option B (Popliteal artery injury) is an acute vascular complication, which was ruled out by the intact distal pulses and brisk capillary refill on initial examination. While possible with high-energy trauma, it's not a long-term risk directly linked to diabetes or smoking in the context of fracture healing.
Option D (Deep peroneal nerve palsy) is an acute neurological complication, which was ruled out by the intact neurological exam. Again, not a long-term risk directly linked to the comorbidities.
Option E (Post-traumatic arthritis of the knee) is a long-term complication, but the CT scan definitively ruled out intra-articular extension into the tibial plateau, making this an extra-articular diaphyseal injury. Therefore, post-traumatic arthritis of the knee joint itself is not a primary concern for this specific fracture pattern, assuming anatomical reduction of the shaft.
During the initial clinical assessment, the patient's lower leg compartments were tense and swollen but remained compressible. Pain with passive stretch of the ischemic muscles was elicited but not deemed disproportionate to the severe underlying fracture. Given the high-energy mechanism and evolving soft tissue edema, the orthopedic team maintained a low threshold for invasive intracompartmental pressure monitoring. Which of the following Delta P values would serve as the absolute indication for emergent four-compartment fasciotomies in this patient?
Correct Answer: B
The case explicitly states that 'A Delta P calculation (diastolic blood pressure minus intracompartmental pressure) of less than 30 mmHg would serve as the absolute indication for emergent four-compartment fasciotomies.' This is a critical threshold used in the diagnosis of acute compartment syndrome, particularly when clinical signs are equivocal or the patient's mental status is altered. A Delta P of less than 30 mmHg indicates that the intracompartmental pressure is approaching the diastolic pressure, compromising capillary perfusion and leading to tissue ischemia.
Options A, C, D, and E represent incorrect thresholds or incorrect pressure calculations. While some literature may cite slightly different thresholds or use MAP, the specific value and calculation (DBP - ICP < 30 mmHg) provided in the case is the one to adhere to for this question.
The radiograph below shows a severely displaced, comminuted fracture of the proximal third of the tibial diaphysis. This specific deformity pattern, characterized by apex anterior (procurvatum) and apex lateral (valgus) angulation, is classic for proximal third tibial fractures. Which of the following is the primary deforming force responsible for the apex anterior angulation of the proximal fragment?
Correct Answer: C
The case explicitly states, 'This specific deformity pattern is classic for proximal third tibial fractures and is driven by the unopposed pull of the extensor mechanism (quadriceps via the patellar tendon) on the proximal fragment, drawing it into extension.' The patellar tendon inserts onto the tibial tubercle, which is part of the proximal fragment. When the tibia fractures proximally, the quadriceps muscle, acting through the patellar tendon, pulls the proximal fragment anteriorly and into extension, creating the apex anterior (procurvatum) deformity.
Option A (Gastrocnemius muscle pull) and Option B (Soleus muscle pull) primarily act on the ankle (plantarflexion) and are attached more distally or posteriorly, contributing to shortening or posterior displacement of the distal fragment, but not the apex anterior deformity of the proximal fragment.
Option D (Pes anserinus muscle group pull) and Option E (Iliotibial band tension) exert variable varus/valgus and rotational forces on the proximal tibia, contributing to the apex lateral (valgus) deformity, but not the primary apex anterior angulation.
Following initial radiographs, a dedicated computed tomography (CT) scan of the right knee and proximal tibia with fine axial cuts and multiplanar reconstructions was ordered. What is the MOST critical reason for obtaining this CT scan in a high-energy proximal third tibial shaft fracture?
Correct Answer: C
The case highlights the critical importance of the CT scan: 'While plain radiographs provide the macroscopic architecture of the diaphyseal injury, they are notoriously insensitive for detecting occult intra-articular extension into the tibial plateau. Literature indicates that up to 20% to 30% of high-energy proximal third tibial shaft fractures possess an unrecognized coronal or sagittal split propagating into the articular surface. The presence of an intra-articular component drastically alters the surgical algorithm...' Therefore, ruling out occult intra-articular extension is the most critical reason, as it fundamentally changes the surgical approach.
Option A (To assess the exact geometry of the medullary canal for intramedullary nail templating) is a valid reason for a CT, but it is secondary to ruling out intra-articular involvement, which dictates whether nailing is even appropriate.
Option B (To identify unrecognized posterior malleolar fractures) is less common with proximal third injuries compared to distal third spiral fractures, and while CT can show it, it's not the primary indication for a *proximal* tibial shaft fracture.
Option D (To evaluate the extent of soft tissue injury and identify fracture blisters) is primarily done clinically and with MRI if needed, not typically the main reason for a CT in this context.
Option E (To confirm the presence of a concomitant fibula fracture) is usually evident on plain radiographs, and while CT will show it, it's not the *most critical* reason for ordering the scan.
The surgical plan for this patient involves a Suprapatellar Intramedullary Nailing technique. What is the primary biomechanical advantage of utilizing the suprapatellar approach with the knee in a semi-extended position (15-20 degrees of flexion) for a proximal third tibial diaphyseal fracture, compared to a traditional infrapatellar approach with hyper-flexion?
Correct Answer: C
The case explicitly states, 'The critical advantage of the suprapatellar approach is patient positioning. The limb is positioned with the knee in a semi-extended posture, resting on a sterile bump at approximately 15 to 20 degrees of flexion. This semi-extended position dramatically reduces the tension on the extensor mechanism, neutralizing the primary deforming force that causes procurvatum.' This directly addresses the challenge of apex anterior malalignment in proximal tibial fractures.
Option A (It allows for easier access to the distal interlocking screws) is incorrect; distal interlocking is typically performed freehand or with a jig, and the approach to the knee does not significantly impact this.
Option B (It reduces the risk of iatrogenic damage to the common peroneal nerve) is incorrect; the common peroneal nerve is at risk around the fibular neck, not typically from the knee entry portal for tibial nailing.
Option D (It provides a more direct line of sight to the fracture site for open reduction) is incorrect; intramedullary nailing is a minimally invasive technique, and the approach is for nail insertion, not open reduction of the fracture site itself.
Option E (It minimizes blood loss by avoiding the infrapatellar fat pad) is not the primary biomechanical advantage and is not a major factor in choosing the suprapatellar approach.
To achieve and maintain reduction and prevent the classic valgus and procurvatum deformity during intramedullary nailing of this proximal tibial fracture, blocking (Poller) screws were employed. Based on the typical deforming forces and the biomechanical principle of blocking screws, where should these screws be strategically placed in the proximal fragment?
Correct Answer: B
The case details the placement of blocking screws: 'To prevent the classic valgus and procurvatum deformity, two blocking screws were placed in the proximal fragment. One screw was placed in the posterior half of the proximal fragment (viewed laterally) to block the nail from translating posteriorly, thereby preventing procurvatum. A second screw was placed in the lateral half of the proximal fragment (viewed on AP) to prevent the nail from translating laterally, thereby preventing valgus.' The principle is to place the screws on the *concave* side of the anticipated deformity to guide the nail centrally.
Option A, C, D, and E describe incorrect placements that would either not effectively block the deformity or could exacerbate it.
The patient's fracture was classified according to the AO/OTA alphanumeric system. Based on the description of a 'severely displaced, comminuted fracture of the proximal third of the tibial diaphysis' with a 'dominant oblique configuration with a large, laterally displaced butterfly fragment,' which AO/OTA classification best describes this injury?
Correct Answer: C
The case explicitly states: 'The fracture was classified according to the AO/OTA alphanumeric system as a 42-B3 injury (Tibia, Diaphysis, Wedge fracture, Fragmented wedge).'
Let's break down the classification:
- 4: Lower leg (tibia/fibula)
- 2: Diaphysis (shaft)
- B: Wedge fracture (a fracture with an intact or reconstructible wedge fragment, which aligns with the 'large, laterally displaced butterfly fragment' description).
- 3: Fragmented wedge (indicating the wedge itself is comminuted or there are multiple fragments within the wedge).
Option A (41-A3) would be a proximal tibia extra-articular simple fracture.
Option B (42-A2) would be a diaphyseal simple oblique fracture.
Option D (43-C2) would be a distal tibia intra-articular multifragmentary fracture.
Option E (42-C3) would be a diaphyseal complex multifragmentary fracture, which is distinct from a wedge fracture.
The CT scan definitively ruled out intra-articular extension into the tibial plateau, confirming an extra-articular diaphyseal injury. If, however, the CT scan had revealed a bicondylar tibial plateau fracture (Schatzker VI) with metaphyseal-diaphyseal dissociation, how would the primary surgical management strategy for this patient fundamentally change?
Correct Answer: D
The case clearly states: 'If articular extension were present, the treatment paradigm would shift entirely towards articular reconstruction and dual plating, abandoning the intramedullary nail approach.' Bicondylar tibial plateau fractures (Schatzker VI) involve the articular surface and metaphyseal-diaphyseal dissociation. The primary goal in these injuries is anatomical reduction of the articular surface to prevent post-traumatic arthritis. Intramedullary nailing is generally contraindicated for significant intra-articular fractures because it cannot adequately reduce and stabilize the articular fragments and can even displace them. Dual plating constructs (medial and lateral) are typically used to achieve stable fixation of the articular block and metaphyseal components.
Option A (Intramedullary nailing would still be the preferred method, but with additional blocking screws) is incorrect; IM nailing is not suitable for significant intra-articular fractures.
Option B (The patient would be managed non-operatively with a long-leg cast) is incorrect; bicondylar tibial plateau fractures are unstable, high-energy injuries that almost always require surgical intervention.
Option C (Emergent four-compartment fasciotomies would be performed immediately, regardless of compartment pressures) is incorrect; fasciotomies are for compartment syndrome, not a primary treatment for the fracture itself, and are indicated based on clinical signs and/or pressure measurements.
Option E (External fixation would be applied as a definitive treatment, followed by delayed IM nailing) is incorrect; while external fixation might be used as a temporary measure (damage control) in severe open or highly comminuted cases, it's not the definitive treatment for a closed bicondylar plateau fracture, and delayed IM nailing is not the standard for articular fractures.
The patient's neurovascular examination revealed palpable and symmetric dorsalis pedis and posterior tibial pulses (2+ bilaterally), brisk capillary refill, and intact motor and sensory function for the deep peroneal, superficial peroneal, and tibial nerves. Despite this reassuring baseline, continuous monitoring was required. Considering the anatomical vulnerability in proximal tibial fractures, which specific neurovascular structure is MOST susceptible to injury due to its tethered course through the interosseous membrane?
Correct Answer: C
The case specifically highlights the vulnerability: 'The popliteal artery bifurcates at the proximal border of the interosseous membrane, and the anterior tibial artery passes anteriorly through the hiatus in the interosseous membrane, tethering it and making it highly susceptible to shear forces in proximal tibial fractures.' This anatomical course makes the anterior tibial artery particularly prone to injury, even in closed fractures, due to its fixed position as it passes through the interosseous membrane.
Option A (Popliteal artery) is a major vessel at risk in knee dislocations or very proximal metaphyseal fractures, but the anterior tibial artery's specific tethering makes it uniquely vulnerable in proximal *tibial shaft* fractures.
Option B (Posterior tibial artery) is less commonly injured in proximal tibial shaft fractures compared to the anterior tibial artery, as it runs in the deep posterior compartment.
Option D (Sural nerve) and Option E (Saphenous nerve) are sensory nerves that are less critical and less frequently injured in a way that would cause major functional deficit compared to the major arteries or motor nerves.
During the intramedullary nailing procedure, sequential flexible reaming was performed. What is a significant benefit of reaming the medullary canal, particularly in the context of promoting fracture healing?
Correct Answer: C
The case states: 'Sequential flexible reaming was performed in 0.5-millimeter increments. Reaming generates autologous bone graft (osteogenic reamings) that is deposited at the fracture site, promoting secondary bone healing.' These reamings contain osteoprogenitor cells and growth factors, which are crucial for enhancing the biological environment at the fracture site and accelerating callus formation.
Option A (It minimizes the risk of fat embolization syndrome) is incorrect; reaming actually *increases* the risk of fat embolization syndrome due to increased intramedullary pressure, though the risk is mitigated by the open nature of the fracture hematoma.
Option B (It creates a larger canal to accommodate a wider nail, thus increasing stability) is partially true in that it allows for a larger nail, which can increase stability, but the *significant benefit for healing* is the autologous bone graft.
Option D (It reduces the need for distal interlocking screws) is incorrect; reaming does not affect the need for interlocking screws, which are essential for rotational and angular stability.
Option E (It prevents iatrogenic damage to the articular cartilage of the patellofemoral joint) is incorrect; the retropatellar cannula system with a protective Teflon sleeve is used to protect the articular cartilage, not the reaming process itself.
A 28-year-old male presents to the emergency department following a high-energy motor vehicle collision, sustaining a right open tibial diaphyseal fracture as shown in the radiograph below. Despite initial hemodynamic stability and palpable distal pulses, the patient's pain rapidly escalates to 10/10 VAS, described as unremitting and out of proportion to the injury, even after high-dose intravenous opioids. On examination, the right lower leg is markedly swollen, tense, and the anterior compartment feels 'wood-hard'. Passive plantarflexion of the ankle elicits excruciating pain. Which of the following findings, if present, would be the LEAST reliable indicator of impending irreversible muscle damage in this patient?
Correct Answer: D
The absence of the dorsalis pedis pulse (Option D) is the LEAST reliable indicator of impending irreversible muscle damage in acute compartment syndrome (ACS). This is a critical clinical pearl. Peripheral pulses are typically maintained until the intra-compartmental pressure exceeds the systolic arterial pressure, making pulselessness an exceedingly late and unreliable sign of ACS. By the time pulses are lost, irreversible myonecrosis and neurological damage have often already occurred. The case explicitly states, 'Crucially, the dorsalis pedis and posterior tibial pulses remained robust and palpable,' despite clear signs of ACS, highlighting this principle.
Option A (Diminished two-point discrimination in the first dorsal webspace) indicates early ischemic neurapraxia of the deep peroneal nerve, which innervates the anterior compartment. This is a significant and reliable sign of evolving ACS.
Option B (A differential pressure (ΔP) of 20 mmHg) is a highly reliable and objective indicator of critical ischemia. A ΔP of less than 30 mmHg (Diastolic Blood Pressure - Intra-compartmental Pressure) is the widely accepted threshold indicating inadequate tissue perfusion and the absolute necessity for emergent fasciotomy. A ΔP of 20 mmHg is well below this threshold.
Option C (Inability to actively dorsiflex the ankle against gravity) signifies profound motor weakness of the tibialis anterior and other anterior compartment muscles, innervated by the deep peroneal nerve. The case describes a rapid decline in motor strength from 3/5 to 1/5, indicating significant muscle ischemia and nerve compromise.
Option E (Exquisite pain with passive stretch of the extensor hallucis longus) is one of the most sensitive and diagnostic clinical findings for ACS. The extensor hallucis longus is located in the anterior compartment, and passive plantarflexion of the ankle or passive flexion of the great toe stretches this muscle, eliciting severe, disproportionate pain due to ischemia.
The patient's open tibial fracture was initially classified as Gustilo-Anderson Type II. However, the rapid onset of acute compartment syndrome (ACS) in this high-energy injury raises concerns about the true extent of soft tissue damage. Which of the following statements best reflects the relationship between open fractures and acute compartment syndrome?
Correct Answer: C
Option C is correct. The case explicitly states, 'The presence of an open fracture is a critical clinical pearl: an open fracture does not adequately decompress the fascial compartments... In many series, the incidence of acute compartment syndrome in open tibial fractures is equal to, or even slightly higher than, that in closed fractures, likely due to the higher energy imparted to the soft tissue envelope.' This directly refutes the common misconception that an open wound prevents ACS.
Option A is incorrect. This is a dangerous misconception. The fascial defect in an open fracture is rarely large enough to allow sufficient extrusion of hematoma and edematous muscle to lower the intra-compartmental pressure below the ischemic threshold.
Option B is incorrect. As explained above, even a 2 cm laceration, while indicating an open fracture, is typically insufficient to decompress the entire compartment effectively.
Option D is incorrect. While major arterial injury can cause ischemia, the case describes robust and palpable distal pulses, ruling out acute arterial occlusion as the primary cause of ischemia. ACS is a localized pressure phenomenon, not a generalized arterial supply issue in this context.
Option E is incorrect. While infection prevention is crucial in open fractures, the primary indication for fasciotomy in ACS is to relieve critical intra-compartmental pressure, restore capillary perfusion, and prevent irreversible myonecrosis and neurological damage. Infection prevention is a secondary benefit of debridement and wound care, not the direct indication for fasciotomy itself.
During the initial orthopedic evaluation, the patient exhibited specific neurological deficits. Given the rapid decline in motor strength and altered sensation, which of the following nerve-compartment associations was most significantly affected in this patient, based on the clinical findings?
Correct Answer: C
Option C is correct. The case describes 'profound weakness' in active dorsiflexion of the ankle (tibialis anterior) and toe extension (EHL, EDL), with a rapid decline from 3/5 to 1/5. These muscles are located in the anterior compartment and are innervated by the deep peroneal nerve. Furthermore, 'diminished two-point discrimination in the first dorsal webspace' is a classic sensory deficit associated with deep peroneal nerve compromise, as this nerve provides sensation to this area. This combination of motor and sensory deficits points directly to significant involvement of the deep peroneal nerve within the anterior compartment.
Option A is incorrect. The tibial nerve innervates the superficial and deep posterior compartments. While the posterior compartments showed some edema, the case states the superficial posterior compartment (gastrocnemius/soleus) maintained 4/5 strength for plantarflexion, indicating less severe involvement compared to the anterior compartment.
Option B is incorrect. The superficial peroneal nerve innervates the lateral compartment (peroneus longus and brevis) and provides sensation to the lateral dorsum of the foot. While the lateral compartment showed a decline in eversion strength (3/5 to 2/5) and altered sensation, the deficits in the anterior compartment (deep peroneal nerve) were described as 'profound' and more rapidly deteriorating.
Option D is incorrect. The common peroneal nerve divides into the deep and superficial peroneal nerves. While it is at risk around the fibular neck, the specific deficits described are distal to this division, affecting the deep and superficial peroneal nerves individually within their respective compartments, rather than a global common peroneal nerve palsy.
Option E is incorrect. The saphenous nerve is a purely sensory nerve providing sensation to the medial aspect of the leg. The case does not describe specific deficits related to this nerve, and there is no distinct 'medial compartment' in the context of ACS, as the medial aspect of the tibia is subcutaneous.
The patient underwent emergent dual-incision four-compartment fasciotomy. During the anterolateral incision, the surgeon must carefully identify and protect specific neurovascular structures. Which of the following structures is most at risk during the release of the lateral compartment fascia, particularly near the fibular neck?
Correct Answer: C
Option C is correct. The case states, 'The lateral fascia was released proximally toward the fibular head (taking extreme care to avoid the common peroneal nerve as it wraps around the fibular neck).' The common peroneal nerve is highly vulnerable as it courses superficially around the fibular neck before dividing into its deep and superficial branches. Iatrogenic injury to this nerve during proximal lateral compartment fasciotomy is a known complication.
Option A (Superficial peroneal nerve) is also at risk during the anterolateral incision, particularly as it exits the lateral compartment fascia to become subcutaneous in the distal third of the leg. The case mentions, 'The superficial peroneal nerve must be identified and protected; it typically exits the lateral compartment fascia to become subcutaneous in the distal third of the leg.' However, the question specifically asks about the risk 'near the fibular neck,' where the common peroneal nerve is most vulnerable.
Option B (Deep peroneal nerve) is located within the anterior compartment, deep to the tibialis anterior muscle, and is generally not at direct risk during the release of the lateral compartment fascia unless dissection is overly aggressive or misdirected.
Option D (Tibial nerve) is located in the deep posterior compartment, protected by the soleus and gastrocnemius muscles, and is at risk during the posteromedial incision, not the anterolateral incision near the fibular neck.
Option E (Anterior tibial artery) is located in the anterior compartment, deep to the muscles, and is generally well-protected during a standard fasciotomy unless dissection is excessively deep or uncontrolled.
Following the fasciotomy, the open tibial fracture was stabilized with an unreamed intramedullary nail. The decision to use an unreamed nail over a reamed nail or external fixation was made based on the patient's stable systemic status. What is the primary advantage of using an unreamed intramedullary nail in this specific clinical scenario (open fracture with acute compartment syndrome) compared to a reamed nail?
Correct Answer: C
Option C is correct. The case states, 'To minimize further endosteal vascular disruption and prevent additional elevation of intra-compartmental pressures, the canal was not reamed.' Reaming the medullary canal causes significant disruption to the endosteal blood supply, which is critical for fracture healing, and can transiently increase intra-compartmental pressures due to the heat generated and the introduction of marrow contents into the soft tissues. In a limb already compromised by ACS, avoiding this additional insult is paramount.
Option A is incorrect. Reamed nails generally provide superior biomechanical stability due to a tighter fit in the medullary canal and the ability to use a larger diameter nail. Unreamed nails are often chosen for their less invasive effect on the biology, not for superior stability.
Option B is incorrect. This statement is irrelevant to the comparison between reamed and unreamed nails, as both are intramedullary devices and do not involve pin tracts like external fixators. External fixators are associated with pin-tract infections, but this option incorrectly attributes the advantage to unreamed nails over reamed nails.
Option D is incorrect. Reamed nails, by providing better stability and potentially promoting faster healing (though this is debated), might allow for earlier weight-bearing in some contexts. Unreamed nails do not inherently enhance fracture healing to allow earlier full weight-bearing; in fact, the case mentions TDWB for 6 weeks due to the comminuted nature of the fracture and reliance on an unreamed construct.
Option E is incorrect. While unreamed nailing might be slightly faster by omitting the reaming steps, this is not the primary advantage in the context of ACS. The biological preservation is the key factor.
Postoperatively, the patient was transferred to the SICU for close monitoring. Aggressive intravenous fluid resuscitation was initiated, and serum creatine kinase (CK) levels, basic metabolic panels, and urine myoglobin were monitored. The patient's CK levels peaked at 8,500 U/L at 24 hours post-op. What is the primary goal of aggressive intravenous fluid resuscitation in this specific postoperative setting?
Correct Answer: C
Option C is correct. The case explicitly states, 'Aggressive intravenous fluid resuscitation with lactated Ringer's solution was initiated to maintain a high urine output (target > 100 mL/hour) to flush myoglobin through the renal tubules and prevent acute tubular necrosis.' This is a direct measure to combat the effects of rhabdomyolysis, a common complication of reperfusion injury after ACS, where damaged muscle releases myoglobin into the bloodstream, which can precipitate in the renal tubules and cause acute kidney injury.
Option A is incorrect. While hydration is generally good for DVT prevention, it is not the primary goal of aggressive fluid resuscitation in the context of rhabdomyolysis. Other measures like early mobilization and pharmacologic prophylaxis are more direct for DVT prevention.
Option B is incorrect. While fluid resuscitation can have some general effects on systemic inflammation, its primary role in this specific context is not to dilute inflammatory mediators to prevent SIRS. SIRS is a complex response, and fluid resuscitation is more targeted at organ protection from specific byproducts of muscle breakdown.
Option D is incorrect. While maintaining hemodynamic stability is always important post-trauma, the case states the patient was hemodynamically stable initially. The aggressive fluid resuscitation post-fasciotomy is specifically for myoglobinuria, not primarily for hypovolemia, unless it develops.
Option E is incorrect. While good systemic perfusion is beneficial for healing, aggressive fluid resuscitation is not a primary intervention specifically aimed at enhancing fracture healing. Its immediate goal is to prevent renal complications from rhabdomyolysis.
During the posteromedial fasciotomy incision, the surgeon must take specific precautions to protect the neurovascular bundle. Which of the following structures constitutes the primary neurovascular bundle at risk in the deep posterior compartment?
Correct Answer: C
Option C is correct. The case states, 'The neurovascular bundle (posterior tibial artery, vein, and tibial nerve) was identified and protected' during the release of the deep posterior compartment. This is the classic neurovascular bundle located in the deep posterior compartment of the leg.
Option A is incorrect. The superficial peroneal nerve is in the lateral compartment, and the anterior tibial artery is in the anterior compartment.
Option B is incorrect. The common peroneal nerve is around the fibular neck, and the popliteal artery is proximal to the leg compartments, in the popliteal fossa.
Option D is incorrect. The saphenous nerve and vein are located subcutaneously on the posteromedial aspect of the leg, superficial to the fascia, and are retracted anteriorly during the posteromedial incision, but they are not the deep posterior compartment neurovascular bundle.
Option E is incorrect. The sural nerve is a sensory nerve in the superficial posterior compartment, and the peroneal artery is a branch of the posterior tibial artery, located deep, but the primary bundle includes the main posterior tibial artery, vein, and tibial nerve.
The patient's fasciotomy wounds were initially left open and managed with negative pressure wound therapy (NPWT). A planned 'second look' surgery was performed at 48-72 hours. By postoperative day 7, the anterolateral wound still exhibited a 4 cm gap and required a split-thickness skin graft (STSG). What is the primary reason for leaving fasciotomy wounds open and delaying definitive closure?
Correct Answer: C
Option C is correct. The case explicitly states, 'The fasciotomy wounds were left open. Primary closure is absolutely contraindicated as it recreates the compartment syndrome.' The primary reason for leaving fasciotomy wounds open is to accommodate the significant post-ischemic edema and swelling that persists for several days. Attempting primary closure too early, before the edema has resolved, would re-elevate intra-compartmental pressures and lead to a recurrence of compartment syndrome, negating the entire purpose of the fasciotomy.
Option A is incorrect. While drainage of exudate is a benefit, it is not the primary reason for leaving the wounds open. NPWT helps manage exudate, but the fundamental reason is pressure relief.
Option B is incorrect. While serial debridement of necrotic muscle (if present) is a crucial part of the 'second look' surgery, the initial decision to leave the wounds open is primarily driven by the need to prevent recurrent compartment syndrome from edema, not solely for debridement. The case notes that in this patient, all muscle bellies remained viable.
Option D is incorrect. While open wounds allow for easier dressing changes and topical treatment, this is a practical consideration, not the primary physiological reason for leaving them open.
Option E is incorrect. While secondary intention healing can occur, the goal for fasciotomy wounds is typically delayed primary closure or skin grafting once edema resolves, to minimize scar burden and improve functional outcomes, rather than specifically promoting secondary intention healing for stronger scar tissue.
The patient's injured extremity was elevated strictly at the level of the heart postoperatively. What is the rationale behind this specific positioning strategy in the management of acute compartment syndrome?
Correct Answer: C
Option C is correct. The case states, 'The injured extremity was elevated strictly at the level of the heart. Elevation above the heart decreases the local arterial perfusion pressure, which can exacerbate ischemia in borderline perfused tissues, while dependent positioning increases venous congestion and edema.' This highlights the delicate balance required. Elevating the limb too high (above the heart) can compromise arterial inflow, especially in tissues that are already borderline ischemic. Conversely, allowing the limb to be dependent (below the heart) increases venous congestion and edema, which can counteract the decompression achieved by fasciotomy and potentially increase intra-compartmental pressure.
Option A is incorrect. While elevation generally promotes venous return, elevating *above* the heart can compromise arterial inflow, which is detrimental in a limb recovering from ischemia.
Option B is incorrect. Dependent positioning (below the heart) increases hydrostatic pressure, which can increase venous congestion and edema, not necessarily enhance arterial inflow in a beneficial way for ACS recovery.
Option D is incorrect. While DVT is a concern, the primary reason for avoiding elevation above the heart is the risk of exacerbating ischemia by reducing arterial perfusion pressure, not primarily DVT risk.
Option E is incorrect. Dependent positioning increases edema and venous congestion, which is counterproductive to reducing swelling and promoting recovery after fasciotomy.
The patient's initial presentation included a 2 cm transversely oriented laceration over the anterior aspect of the distal third of the tibia. This was classified as a Gustilo-Anderson Type II open fracture. Given the high-energy mechanism and the rapid development of compartment syndrome, which of the following statements regarding the Gustilo-Anderson classification is most accurate in predicting the severity of soft tissue injury?
Correct Answer: C
Option C is correct. The Gustilo-Anderson classification primarily focuses on the size of the skin wound, the presence of contamination, and the extent of periosteal stripping. While it provides a general guide to the severity of the open injury, it does not fully quantify the underlying soft tissue energy absorption or the potential for deep tissue damage, especially in high-energy injuries. The case highlights this by stating, 'the high-energy mechanism (70 km/h MVC) suggested significant underlying soft tissue injury not immediately visible at the skin level, which was corroborated by the rapid onset of compartment syndrome.'
Option A is incorrect. The Gustilo-Anderson classification does not directly quantify muscle necrosis or nerve damage. These are clinical findings that evolve and are assessed separately.
Option B is incorrect. As demonstrated in this case, a Type II classification (laceration >1 cm without extensive soft tissue damage) does not reliably preclude severe complications like ACS, especially in high-energy trauma. The superficial wound may not reflect the deep tissue injury.
Option D is incorrect. This is a dangerous misconception, as discussed in the case. An open fracture, regardless of its Gustilo-Anderson type, does not guarantee adequate fascial decompression and does not prevent ACS.
Option E is incorrect. While the Gustilo-Anderson classification influences overall management (e.g., timing of definitive fixation, need for soft tissue coverage), it is not the primary determinant for choosing between reamed and unreamed intramedullary nailing. That decision is more influenced by factors like patient stability, presence of ACS, and surgeon preference regarding endosteal blood supply preservation.
The patient's pain was described as a deep, throbbing, and constant pressure, completely unrelieved by repositioning, elevation, or immobilization, and noticeably worse than initial assessment despite high-dose opioids. This pain profile is a hallmark of acute compartment syndrome. Which of the following characteristics of pain is considered the most sensitive and specific clinical sign for diagnosing acute compartment syndrome?
Correct Answer: D
Option D is correct. The case emphasizes, 'The patient reported excruciating, unremitting pain in his right lower leg, rated as 10/10 on the Visual Analog Scale. This pain severity persisted despite the administration of 10 mg of intravenous morphine sulfate by EMS en route, followed by an additional 50 mcg of intravenous fentanyl in the trauma bay. The patient described the pain as a deep, throbbing, and constant pressure that was completely unrelieved by repositioning, elevation, or immobilization... This pain profile was noticeably worse and out of proportion to the initial assessment... The most critical and diagnostic finding was the assessment of pain with passive stretch of the ischemic muscle groups.' This 'pain out of proportion' and severe pain with passive stretch are the most sensitive and specific clinical signs for ACS.
Option A is incorrect. Pain localized over the fracture site is expected with any fracture and is not specific to ACS.
Option B is incorrect. Pain that improves with limb elevation is typical for venous congestion or simple edema, but ACS pain is often unrelieved or even worsened by elevation if it compromises arterial inflow.
Option C is incorrect. ACS pain is classically described as 'unrelieved by standard doses of analgesia' or 'out of proportion' to the injury, meaning it persists despite significant pain medication.
Option E is incorrect. Sharp, shooting pain radiating distally is more characteristic of nerve impingement or direct nerve injury, not the deep, throbbing, pressure-like pain of ischemic muscle in ACS.
A 42-year-old male sustains a distal third femoral shaft fracture. Radiographs typically demonstrate an apex posterior angulation of the distal fragment. Which of the following muscles is the primary deforming force responsible for this specific angulation?
According to current literature and guidelines, which of the following is the single most critical factor in reducing the risk of deep infection in this patient?
Approximately 36 hours after admission, he becomes confused, tachypneic (RR 30), and develops a petechial rash over his axilla and conjunctiva. Arterial blood gas shows a PaO2 of 55 mmHg. What is the primary pathophysiologic mechanism underlying the pulmonary manifestations of this syndrome?
Which muscles are at the highest risk of ischemic necrosis due to their central and deep location in the volar forearm?
None
