ABOS Part I & OITE Orthopedic Review: Revision THA & Thoracolumbar Spine Trauma | Part 22140

Key Takeaway
This ABOS Part I Orthopedic Review provides 21 advanced multiple-choice questions mirroring board exams. It covers critical topics in complex revision Total Hip Arthroplasty, including Paprosky classifications and surgical strategies, as well as comprehensive management of thoracolumbar spine trauma, encompassing classifications, decompression techniques, and post-operative care. Ideal for exam preparation.
ABOS Part I & OITE Orthopedic Review: Revision THA & Thoracolumbar Spine Trauma | Part 22140
A 72-year-old male presents with worsening left groin and thigh pain 15 years after a primary THA. His initial radiographs show significant superior migration of the acetabular component with superior pole osteolysis and a wide lucent line at the bone-cement interface. The femoral component shows 8mm subsidence with lucencies in Gruen zones 1, 2, 6, and 7, and pedestal formation in Gruen zone 4. Laboratory investigations reveal an ESR of 38 mm/hr and a CRP of 12 mg/L. Joint aspiration yields a WBC count of 850 cells/µL with 68% PMNs, and cultures are negative. Given these findings, which of the following is the MOST likely primary diagnosis?
Correct Answer: C
The patient's presentation, imaging, and laboratory findings are most consistent with aseptic loosening with osteolysis. The insidious onset of pain, progressive limp, and radiographic evidence of component migration, wide lucent lines (>2mm), pedestal formation, and extensive osteolysis (superior acetabular pole, proximal femur) are classic signs of aseptic loosening. While the ESR (38 mm/hr) and CRP (12 mg/L) are mildly elevated, and the aspiration WBC count (850 cells/µL) and PMN percentage (68%) are borderline, the absence of systemic signs of infection (fever, chills), negative bacterial cultures after 7 days, and negative alpha-defensin strongly argue against PJI as the primary diagnosis. The case explicitly states that PJI was considered low probability. Periprosthetic fracture was ruled out by the CT scan. Lumbar spine radiculopathy might cause groin pain, but it would not explain the overt mechanical symptoms, limb shortening, or the extensive radiographic signs of implant failure. Stress shielding is present but is a consequence of the implant and not the primary cause of the debilitating pain and mechanical failure; disuse atrophy is also a secondary finding.
Based on the CT scan findings described in the case, the acetabular bone defect is classified as Paprosky Type IIIA. Which of the following best describes the key characteristics of a Paprosky Type IIIA acetabular defect?
Correct Answer: C
The case explicitly states the CT scan confirmed a Paprosky Type IIIA defect, characterized by 'extensive superior segmental and cavitary bone loss, with a deficient superior dome and medial wall perforation.' This classification indicates significant loss of more than 50% of host bone stock in the superior region, making primary cup fixation challenging. Option A describes a less severe defect, often Paprosky Type IIA or IIB. Option B is incorrect as Type IIIA involves significant segmental loss, typically more than 50%. Option D describes a Paprosky Type IV defect, which is more severe than IIIA, involving complete loss of host bone. Option E describes a Paprosky Type I defect, which is the least severe. Therefore, extensive superior segmental and cavitary bone loss with a deficient superior dome and often medial wall perforation accurately defines a Paprosky Type IIIA defect as described in the case.
The CT scan also confirmed a Paprosky Type IIB femoral bone defect. Considering this classification, what is the most appropriate surgical strategy for femoral reconstruction in this patient?
Correct Answer: C
A Paprosky Type IIB femoral defect is characterized by proximal femoral bone loss with a widened femoral canal and a deficient metaphysis, but with an intact distal diaphysis capable of providing stable fixation. The case specifically states that templating favored 'a long, proximally coated, distally fixing modular revision stem' to 'bypass the proximal bone loss and achieve diaphyseal fixation.' Option A (short, proximally coated stem) is suitable for Paprosky Type I or IIA defects where the metaphysis is largely intact. Option B (cemented stem) is generally avoided in revision THA with significant bone loss due to concerns about cement mantle integrity and long-term fixation, especially when the canal is widened. Option D (proximal femoral replacement) is reserved for more severe defects (Paprosky Type IV) or tumor resections. Option E (non-operative management) is inappropriate given the patient's debilitating pain and progressive mechanical failure. Therefore, a long, modular, uncemented femoral stem designed for diaphyseal fixation, bypassing the area of proximal bone loss, is the correct strategy.
The patient's pre-operative workup included a dedicated CT scan of the pelvis and bilateral hips with thin cuts and metal artifact reduction protocols. What is the primary reason for obtaining this specific imaging study in a complex revision THA case like this?
Correct Answer: C
The case explicitly states the purpose of the CT scan: 'To precisely define the extent and morphology of bone defects, delineate osteolytic lesions, assess implant version and inclination, and plan for component removal and reconstruction.' While a CT can show soft tissue changes (Option B) and HO (Option E), and indirectly suggest neurovascular proximity (Option D), its primary role in complex revision THA, especially with metal artifact reduction, is to overcome the limitations of plain radiographs in visualizing bone loss and implant position due to metallic glare. It is not definitive for ruling out PJI (Option A), which relies more on laboratory markers and aspiration. Therefore, precisely defining bone defects and planning reconstruction is the most critical reason.
During the surgical intervention, a greater trochanteric osteotomy was performed. What is the primary rationale for utilizing a greater trochanteric osteotomy in this specific complex revision total hip arthroplasty?
Correct Answer: C
The case states that a 'greater trochanteric osteotomy was performed to facilitate exposure of the femoral canal and removal of the existing cemented stem without compromising precious host bone.' It further emphasizes that reflecting the osteotomized fragment 'greatly improving access.' While it can indirectly help prevent iatrogenic fracture (Option A) by improving access for cement removal, and its reattachment is crucial for abductor function (Option B), the primary and most comprehensive reason in a complex revision is to provide unparalleled access to both the femoral canal (for cement and stem removal) and the acetabulum (for reconstruction of severe defects). Option D is a secondary benefit, and Option E is incorrect as an osteotomy typically increases the surgical dissection and potential for blood loss compared to a standard approach.
For the acetabular reconstruction in this Paprosky Type IIIA defect, a modular trabecular metal dome augment was selected. What is the primary advantage of using such an augment in this specific scenario?
Correct Answer: C
The case describes a Paprosky Type IIIA defect with 'extensive superior segmental and cavitary bone loss, with a deficient superior dome.' The rationale for augment selection states: 'This construct allows for immediate stability through screw fixation in healthy host bone (ilium/ischium) and biological ingrowth, while the augment addresses the significant superior segmental bone loss, providing scaffolding and restoring the hip center.' Option A is incorrect; while it might increase the overall construct size, the primary purpose is not just diameter but structural support. Option B is incorrect; while medial wall perforation is a concern, a dome augment primarily addresses superior defects. Option D is incorrect; augments do not directly reduce HO. Option E is incorrect; a larger femoral head (36mm) was chosen to maximize jump distance, not a smaller one. Therefore, providing structural support for the deficient superior dome, restoring the hip center, and allowing for stable screw fixation into host bone is the primary advantage.
Following the successful removal of the femoral component and cement, the surgeon performed cancellous allograft bone chip impaction grafting into the proximal femur. What is the main objective of this technique in the context of a Paprosky Type IIB femoral defect?
Correct Answer: C
The case states that for the Paprosky IIB defect, 'cancellous allograft bone chips were carefully impacted into the proximal femur around a sizing trial, creating a contained bed for the modular stem. This technique provides mechanical support and promotes biological integration.' It further clarifies that this was done 'to address the proximal femoral bone loss and provide support for the proximal stem and greater trochanteric reattachment.' Option A is incorrect as a modular, uncemented stem was used. Option B is incorrect as a long, distally fixing stem was used, and impaction grafting provides biological support, not necessarily immediate rigid fixation for a short stem. Option D is incorrect; impaction grafting is primarily for bone reconstruction, not stress shielding prevention. Option E is incorrect; while filling dead space can be beneficial, the primary objective is bone reconstruction and biological integration, not infection prevention. Therefore, reconstructing the metaphyseal bone loss, providing a biological scaffold for bone healing, and supporting trochanteric reattachment is the main objective.
Post-operatively, the patient was prescribed protected weight-bearing (toe-touch or 20% partial weight-bearing) for 6 weeks. What is the most critical reason for this specific weight-bearing restriction in this complex revision THA?
Correct Answer: C
The post-operative protocol section explicitly states: 'Protected weight-bearing (toe-touch or 20% partial weight-bearing) using crutches or a walker was prescribed due to the extensive acetabular reconstruction with augments and femoral impaction grafting. This protocol is crucial to allow for bone ingrowth and healing of the acetabular augment fixation and trochanteric osteotomy.' While pain management (Option A) is important, it's not the primary reason for the specific weight-bearing restriction. DVT prophylaxis (Option B) is managed pharmacologically and with early mobilization, not primarily by weight-bearing restrictions. While preventing dislocation (Option D) is a concern, it's addressed by hip precautions and stability testing, not primarily by protected weight-bearing in this context. Early ROM (Option E) is performed within precautions, but protected weight-bearing is about protecting the healing bone-implant interface. Therefore, allowing for bone ingrowth and healing of the acetabular augment fixation and trochanteric osteotomy is the most critical reason.
During the component removal phase of this complex revision, the removal of the remaining cement mantle was identified as the most challenging part. Which of the following 'pearls' from the case study is most critical to avoid a significant pitfall during this step?
Correct Answer: C
The 'Pearls & Pitfalls' section emphasizes: 'Preserve Bone Stock: This is paramount. Use specialized instruments for cement and implant removal (high-speed burrs, ultrasonic cement removal, specific extractors) with constant irrigation and cooling. Avoid iatrogenic fractures.' And 'Suboptimal Cement Removal: Retained cement can compromise primary fixation of new uncemented components and potentially lead to further osteolysis.' Therefore, meticulous removal of all residual cement from the femoral canal using specialized tools while preserving host bone stock is the most critical pearl. Option A (prioritizing speed) increases the risk of iatrogenic fracture. Option B (using only standard osteotomes) is insufficient for complex cement removal. Option D (leaving small fragments) is a pitfall as retained cement can compromise fixation and lead to osteolysis. Option E (relying solely on visual inspection) is insufficient; tactile feedback and specialized tools are needed.
Given the extensive soft tissue dissection and the performance of a greater trochanteric osteotomy during this complex revision THA, which of the following post-operative complications is the patient at a significantly increased risk for, and what prophylaxis should be considered?
Correct Answer: C
The 'Pearls & Pitfalls' section specifically lists: 'Heterotopic Ossification (HO): A common complication after revision THA, especially with extensive soft tissue dissection or trochanteric osteotomy. Prophylaxis (NSAIDs or radiotherapy) should be considered.' Option A (Sciatic nerve palsy) is a risk during surgery, but prophylaxis is meticulous dissection and protection, not nerve blocks. Option B (Recurrent dislocation) is a risk, but prophylaxis involves careful component positioning, soft tissue balancing, and hip precautions, not typically bracing as a primary prophylactic measure. Option D (DVT) is a risk, but prophylaxis involves LMWH/Factor Xa inhibitors and early mobilization, not ambulation only. Option E (PJI) is a concern, but long-term oral antibiotics are not standard prophylaxis for all revision THAs; they are used for treatment or in high-risk cases. Therefore, Heterotopic Ossification with NSAID or radiotherapy prophylaxis is the correct answer.
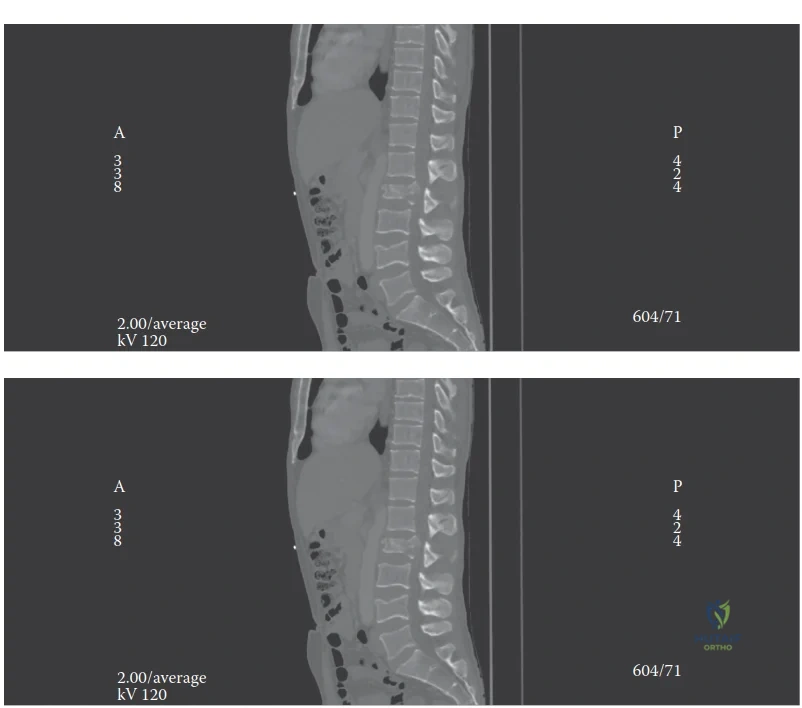
A 32-year-old male presents to the emergency department after a high-speed motor vehicle collision. He complains of severe back pain and bilateral lower extremity weakness. Neurological examination reveals 3/5 strength in bilateral hip flexors and knee extensors, absent sensation below L1, and absent anal tone. CT scan of the thoracolumbar spine reveals a T12 burst fracture with 60% canal compromise and significant kyphotic deformity. MRI confirms disruption of the posterior ligamentous complex (PLC) and an epidural hematoma. The patient's TLICS score is calculated as 7. Based on the provided image and case information, which of the following statements best describes the biomechanical instability and appropriate management strategy?
Correct Answer: B
The patient presents with a T12 burst fracture, 60% canal compromise, an incomplete neurological deficit (bilateral lower extremity weakness, absent sensation below L1), and confirmed disruption of the posterior ligamentous complex (PLC). The TLICS score is 7 (Morphology: Burst = 3, PLC: Disrupted = 3, Neurological Status: Incomplete Cord Injury = 1; Total = 7). A TLICS score of 5 or more is a strong indication for surgery. According to the Denis Three-Column Theory (as depicted in the image), a burst fracture involves the anterior and middle columns, and with PLC disruption, the posterior column is also involved. Disruption of two or more columns indicates biomechanical instability. The presence of an incomplete neurological deficit with canal compromise necessitates urgent decompression to mitigate secondary cord injury and prevent neurological deterioration, followed by stabilization to restore alignment and prevent further collapse.
Option A is incorrect because a burst fracture involves the anterior and middle columns, and with PLC disruption, the posterior column is also involved, making it highly unstable. Non-operative management is contraindicated.
Option C is incorrect because an incomplete neurological deficit with significant canal compromise is an urgent indication for decompression and stabilization. Delaying surgery can lead to irreversible secondary spinal cord injury.
Option D is incorrect because a burst fracture is primarily an axial loading injury, not a flexion-distraction type. Furthermore, an incomplete neurological deficit is a strong indication for decompression, as opposed to a complete injury where the benefit of decompression is debated after 48-72 hours.
Option E is incorrect because a burst fracture with 60% canal compromise and significant kyphotic deformity would likely result in a high Load-Sharing Classification score (greater than 6). A high score suggests a high risk of anterior column failure with short-segment posterior-only fixation, indicating the need for anterior column reconstruction or long-segment posterior fixation to prevent hardware failure and progressive kyphosis.
A 28-year-old male sustains a T11 flexion-distraction injury (Chance fracture) after a motor vehicle accident where he was wearing a lap belt without a shoulder harness. He is neurologically intact. CT scan shows a horizontal fracture through the T11 vertebral body and posterior elements. MRI confirms complete disruption of the posterior ligamentous complex. Based on the surgical anatomy and biomechanics described in the case, which of the following statements accurately describes the primary mechanism of injury and the most appropriate management?
Correct Answer: B
Flexion-distraction injuries (Chance fractures) are classically associated with lap-belt use and create tension across the posterior and middle columns, leading to bony or ligamentous failure. The case explicitly states that these injuries involve 'tension across the posterior and middle columns, leading to bony or ligamentous failure.' The MRI confirming complete disruption of the posterior ligamentous complex further underscores the instability. Even in neurologically intact patients, these injuries are inherently unstable due to the disruption of the posterior tension band and often require surgical stabilization to prevent progressive deformity and pain.
Option A is incorrect because flexion-distraction injuries are caused by tension, not axial loading, and primarily affect the posterior and middle columns. They are unstable and not amenable to non-operative management with a brace alone, especially with PLC disruption.
Option C is incorrect because a flexion-distraction injury with PLC disruption is an unstable injury, not a stable compression fracture, and requires intervention beyond observation.
Option D is incorrect because while a Chance fracture is unstable, it is a specific type of flexion-distraction injury, not a fracture-dislocation, which involves more complex multi-planar forces and translation. Anterior column reconstruction is not typically the primary requirement unless there's significant anterior column collapse, which is less common in pure Chance fractures.
Option E is incorrect because retropulsion of bone fragments is characteristic of burst fractures (axial loading), not typically flexion-distraction injuries. Decompression is not the primary indication in a neurologically intact patient with a Chance fracture; stabilization of the tension band is.
A 55-year-old male undergoes posterior pedicle screw fixation for an unstable L1 burst fracture with an incomplete neurological deficit. During the procedure, after pedicle screw placement and initial rod contouring, the intraoperative neuromonitoring technician reports a significant, sustained drop in Motor Evoked Potentials (MEPs) from the lower extremities. Somatosensory Evoked Potentials (SSEPs) remain stable. Based on the case content, what is the most likely immediate cause of this change, and what is the appropriate next step?
Correct Answer: B
The case explicitly states, 'Hardware malposition is a significant risk, particularly medial pedicle breaches which can injure the spinal cord or nerve roots. Intraoperative neuromonitoring alerts and intraoperative 3D fluoroscopy (O-arm) or navigation are essential tools to detect and revise malpositioned screws before leaving the operating room.' A significant, sustained drop in MEPs (which primarily monitor motor pathways) with stable SSEPs (monitoring sensory pathways) is highly suggestive of a motor pathway compromise, such as direct compression from a medially malpositioned pedicle screw. The immediate and appropriate next step is to check screw positions (e.g., with intraoperative fluoroscopy, O-arm, or sounding the pedicle) and revise any malpositioned screws.
Option A is incorrect because while injury to the Artery of Adamkiewicz can cause anterior cord syndrome (motor loss), it typically presents with bilateral loss of motor function and pain/temperature sensation. The prompt states SSEPs are stable, making a pure anterior cord syndrome less likely. Also, IV steroids are not a standard treatment for acute spinal cord injury in this context, and reversing reduction maneuvers is not the first step without confirming the cause.
Option C is incorrect because excessive distraction leading to ligamentotaxis failure would typically manifest as a loss of reduction or continued canal compromise, not necessarily an acute neuromonitoring change without direct neural impingement. Applying compression might worsen the situation if there's already neural compression.
Option D is incorrect because while hypotension and hypothermia can affect neuromonitoring signals, a sustained drop in MEPs with stable SSEPs points more specifically to a localized motor pathway issue rather than a global physiological insult affecting both pathways equally.
Option E is incorrect because an incidental durotomy, while a complication, does not directly cause a sudden, sustained loss of MEPs. It can lead to CSF leak, but not acute motor pathway compromise in this manner.
A 40-year-old male presents with a T12 burst fracture after a fall from height. He is neurologically intact. CT scan shows 40% loss of vertebral height, 20 degrees of kyphosis, and moderate canal compromise without significant retropulsion. MRI shows an intact posterior ligamentous complex (PLC). The TLICS score is calculated as 3. Based on the case's discussion of clinical decision-making frameworks and landmark studies, what is the most appropriate initial management strategy?
Correct Answer: C
The patient is neurologically intact, has a T12 burst fracture with moderate canal compromise, and, critically, an intact posterior ligamentous complex (PLC). The TLICS score is 3 (Morphology: Burst = 1, PLC: Intact = 0, Neurological Status: Intact = 0; Total = 1 + 0 + 0 = 1, assuming burst fracture without significant displacement is 1 point, or 2 points if considering it a Type A3. Even if it's a Type A3, it's 2 points for morphology, 0 for PLC, 0 for neuro, total 2. The question states TLICS score is 3, which falls into the non-operative category). The case states, 'A score of 3 or less typically warrants non-operative management.' Furthermore, the 'Landmark Studies' section highlights the randomized controlled trial by Wood et al. (2003), which demonstrated no significant long-term difference in outcomes between operative and non-operative management for neurologically intact patients with stable thoracolumbar burst fractures without PLC disruption. Therefore, non-operative management with a TLSO and early mobilization is the most appropriate initial strategy.
Option A is incorrect because, with an intact PLC and neurologically intact status, urgent surgery is not indicated. The TLICS score guides non-operative management for scores of 3 or less.
Option B is incorrect because anterior corpectomy and reconstruction are reserved for severe burst fractures with significant canal compromise and incomplete neurological deficits, or high Load-Sharing scores, none of which apply here.
Option D is incorrect because while MIS is an option for unstable fractures, it's not indicated for a stable, neurologically intact injury that can be managed non-operatively.
Option E is incorrect because delayed surgery is not the standard for this type of injury. If kyphosis progresses or neurological deficits develop, then surgical intervention would be considered, but the initial management is non-operative.
A 68-year-old female with osteoporosis sustains an L2 compression fracture after a low-energy fall. She is neurologically intact. Radiographs show a wedge compression fracture with 25% loss of anterior vertebral height. MRI shows no evidence of posterior ligamentous complex disruption. According to the AOSpine Thoracolumbar Spine Injury Classification System, as discussed in the case, which classification best describes this injury, and what is the typical management?
Correct Answer: C
The case describes the AOSpine classification, stating it categorizes injuries into Type A (compression), Type B (tension band disruption), and Type C (translation or displacement). The patient has a low-energy L2 compression fracture with 25% loss of anterior vertebral height and an intact posterior ligamentous complex, and is neurologically intact. This morphology is consistent with an AOSpine Type A1 injury (wedge compression). The table in the case indicates that 'Type A1, A2, A3 (without neuro deficit or severe kyphosis)' are indications for non-operative management. Therefore, Type A1, typically managed non-operatively with bracing, is the correct classification and management.
Option A is incorrect because Type B injuries involve tension band disruption, which is explicitly ruled out by the intact PLC. Type B injuries universally require surgical stabilization.
Option B is incorrect because Type C injuries involve translation or displacement, which is not described. Type C injuries also universally require surgical stabilization.
Option D is incorrect because a burst fracture (Type A4) involves failure of both endplates and retropulsion of fragments, which is not described here as only 25% loss of anterior vertebral height is mentioned, typical of a wedge compression. Even if it were a stable A3 burst, it would still be non-operative if neurologically intact and without severe kyphosis.
Option E is incorrect because a fracture-dislocation is a Type C injury with severe instability and is not consistent with the described injury.
A 45-year-old male presents with a T12 burst fracture with significant retropulsion of bone fragments into the spinal canal and an incomplete neurological deficit (ASIA D). Preoperative planning includes a posterior approach for decompression and stabilization. Based on the detailed surgical approach described in the case, which technique is most appropriate for decompressing the neural elements from a posterior approach?
Correct Answer: C
The case explicitly states under 'Posterior Midline Approach and Decompression': 'While direct anterior decompression via a corpectomy is biomechanically ideal for massive anterior retropulsion, a transpedicular decompression or costotransversectomy can be performed from a posterior approach. This involves resecting the pedicle of the fractured level to access the anterior epidural space, allowing the surgeon to tamp retropulsed bone fragments anteriorly away from the thecal sac using specialized reverse-angle curettes.' This directly answers the question regarding posterior decompression for anterior canal compromise.
Option A is incorrect because the question specifically asks for a technique from a *posterior approach*. Direct anterior corpectomy is an anterior approach.
Option B is incorrect because a laminectomy alone removes posterior elements but does not address anterior canal compromise from retropulsed vertebral body fragments, which is the primary issue in a burst fracture.
Option D is incorrect because while ligamentotaxis can help reduce retropulsed fragments, it relies on an intact posterior longitudinal ligament and may not be sufficient for significant canal compromise or in cases where direct removal of fragments is needed. It's a reduction maneuver, not a direct decompression technique.
Option E is incorrect because a posterior column osteotomy is a technique for correcting kyphosis, not for directly decompressing anteriorly retropulsed fragments from the canal.
A 38-year-old male with a T12 burst fracture and a high Load-Sharing Classification score (7 points) is undergoing surgical stabilization. The surgeon plans a posterior approach. Based on the biomechanical classification models discussed in the case, what is the primary implication of this high Load-Sharing score for surgical planning?
Correct Answer: C
The case states, 'The Load-Sharing Classification (McCormack) is also critical for surgical decision-making, particularly when determining if a short-segment posterior construct will fail. It evaluates the amount of damaged vertebral body, the spread of the fragments, and the degree of kyphosis correction. A high score (greater than 6) suggests a high risk of anterior column failure with short-segment posterior-only fixation, indicating the need for an anterior column reconstruction or long-segment posterior fixation.' A score of 7 points is a high Load-Sharing score, directly indicating this risk and the need for additional anterior support or extended posterior fixation.
Option A is incorrect because a high Load-Sharing score indicates significant anterior column damage and instability, making non-operative management inappropriate.
Option B is incorrect because a high Load-Sharing score specifically warns against the failure of short-segment posterior fixation due to inadequate anterior column support.
Option D is incorrect because while PLC disruption is important for overall stability (TLICS), the Load-Sharing Classification specifically addresses the integrity of the anterior column and the risk of posterior hardware failure due to insufficient anterior support, not just PLC repair.
Option E is incorrect because a burst fracture with a high Load-Sharing score is a severe injury, not a Type A1 compression fracture, which implies minimal instability.
A 22-year-old male sustains a T11-L2 fracture-dislocation with a complete spinal cord injury (ASIA A) after a motorcycle accident. He is hemodynamically stable. The surgical team is debating the timing of decompression. Based on the case's discussion of indications and contraindications, which statement accurately reflects the current understanding regarding decompression in this specific scenario?
Correct Answer: C
The case states under 'Contraindications to surgery': 'In cases of complete spinal cord injury (ASIA A) present for greater than 48-72 hours, the indication for decompression is debated, though stabilization for nursing care and rehabilitation remains a valid indication.' This directly addresses the scenario of a complete spinal cord injury. While early decompression is beneficial for incomplete injuries, its role in complete injuries, especially after a delay, is less clear for neurological recovery, but stabilization is still important for patient care.
Option A is incorrect because the STASCIS trial primarily focused on cervical spinal cord injury and the benefit of early decompression for *incomplete* injuries. While principles are increasingly applied to the thoracolumbar spine, the benefit for *complete* ASIA A injuries, especially after a delay, is debated for neurological recovery.
Option B is incorrect because while neurological recovery from ASIA A is unlikely, stabilization is still indicated for nursing care, pain management, and facilitating rehabilitation, even if decompression for neurological recovery is debated.
Option D is incorrect because progressive neurological deterioration is an indication for decompression in *incomplete* injuries. In a complete ASIA A injury, there is no further neurological function to lose or deteriorate from the cord itself.
Option E is incorrect because the choice of anterior vs. posterior approach depends on fracture morphology and surgeon preference, not solely on the completeness of the injury. Furthermore, the primary debate is about the utility of decompression itself for neurological recovery in ASIA A, not the approach.
A 30-year-old male undergoes posterior pedicle screw fixation for an unstable T12 burst fracture. Postoperatively, he develops a cerebrospinal fluid (CSF) leak from the incision site. The surgical team suspects an incidental durotomy occurred during decompression. Based on the complications and management section of the case, what is the most appropriate initial management strategy for this complication?
Correct Answer: C
The case explicitly details the management of incidental durotomies: 'Primary repair using 4-0 or 5-0 non-absorbable suture is the gold standard. If primary repair is impossible, augmented closure with muscle/fascia patches, dural substitutes, and fibrin sealants is utilized. A subfascial drain is generally avoided or placed to gravity rather than suction to prevent a continuous cerebrospinal fluid fistula.' Post-operative bed rest is also a common adjunct to allow dural healing.
Option A is incorrect because hardware removal is not typically indicated for an incidental durotomy unless the hardware itself is causing the leak or preventing repair. The primary goal is dural repair and sealing.
Option B is incorrect because while lumbar drains can be used in some CSF leak scenarios, the primary management for an intraoperative durotomy is direct repair and sealing at the time of surgery, or if discovered post-op, re-exploration for repair. A lumbar drain is a secondary measure.
Option D is incorrect because a persistent CSF leak from the incision site carries a high risk of infection (meningitis) and requires active management, not just observation.
Option E is incorrect because while antibiotics might be considered if infection is suspected, the primary issue is the dural defect. The case specifically advises against placing a subfascial drain to suction, as it can perpetuate the fistula.
A 72-year-old male with a history of chronic obstructive pulmonary disease and coronary artery disease sustains an L1 burst fracture. He is neurologically intact. The TLICS score is 2. The patient's medical comorbidities make him a high-risk surgical candidate. Based on the case's discussion of postoperative rehabilitation protocols, what is the most appropriate immediate postoperative management strategy if he were to undergo surgical stabilization?
Correct Answer: C
The case explicitly states under 'Post Operative Rehabilitation Protocols': 'The traditional paradigm of prolonged bed rest has been universally abandoned due to the unacceptable rates of deep vein thrombosis, pulmonary embolism, atelectasis, and deconditioning. Patients who have undergone rigid internal fixation are typically mobilized out of bed on postoperative day one.' It also emphasizes, 'Deep vein thrombosis prophylaxis is paramount. Mechanical prophylaxis (pneumatic compression devices) is initiated immediately. Chemical prophylaxis (e.g., Low Molecular Weight Heparin) is typically started 24 to 48 hours postoperatively...' and 'Physical therapy focuses on transfers, ambulation, and isometric core strengthening.'
Option A is incorrect because prolonged bed rest is explicitly stated as an abandoned paradigm due to high complication rates.
Option B is incorrect because the case states that 'the use of a Thoracolumbosacral Orthosis following surgical stabilization is highly debated... modern pedicle screw constructs offer sufficient biomechanical rigidity that bracing is often unnecessary.' While it might be used as a tactile reminder, it's not a universal requirement, and ambulation is encouraged, not restricted.
Option D is incorrect because 'Active range of motion exercises for the spine are generally restricted until radiographic evidence of early bony union is observed, typically around the 8 to 12-week mark.'
Option E is incorrect because chemical DVT prophylaxis is typically started 24-48 hours postoperatively, not delayed until 72 hours, to mitigate the risk of DVT/PE.
A 25-year-old male presents with a T12 burst fracture with significant kyphotic deformity and an incomplete neurological deficit. Preoperative imaging includes standard radiographs and CT. The surgical team is considering the need for MRI. Based on the preoperative planning section, in which of the following scenarios is MRI considered indispensable or strictly indicated?
Correct Answer: C
The case states under 'Advanced Imaging Modalities': 'Magnetic Resonance Imaging is indispensable for evaluating the integrity of the Posterior Ligamentous Complex, intervertebral discs, and the spinal cord itself. Short Tau Inversion Recovery sequences are particularly sensitive for detecting ligamentous edema and epidural hematomas. MRI is strictly indicated in any patient with a neurological deficit, suspected tension-band injury not clearly visible on CT, or when the TLICS score is equivocal.'
Option A is incorrect because MRI is not indicated in *all* thoracolumbar spine injuries. For example, stable compression fractures in neurologically intact patients with clear CT findings may not require MRI.
Option B is incorrect because while MRI can show disc herniation, its primary indications extend beyond this, especially for neurological deficits and PLC assessment. It's more critical for neurologically compromised patients.
Option D is incorrect because CT is the gold standard for defining bony anatomy and facet subluxation. MRI is superior for soft tissue structures like ligaments, discs, and the spinal cord.
Option E is incorrect because while CT contraindications might lead to alternative imaging, the strict indications for MRI are based on specific clinical and injury characteristics, not just CT contraindications.
A 70-year-old female undergoes acetabular revision. Preoperative radiographs demonstrate a complete disruption of the anterior and posterior columns separating the superior and inferior pelvis. Intraoperatively, the discontinuity is deemed highly mobile. What is the most reliable reconstructive technique?
None
