Master ABOS Board Review: Scleroderma, Dwarfism, Infections, Osteomalacia | Part 26
20 Jun 2026
49 min read
42 Views

Key Takeaway
This ABOS Board Review covers critical topics for orthopaedic surgeons, including systemic sclerosis manifestations, mesomelic dwarfism types and genetics, iatrogenic orthopaedic infection diagnosis and management, and the pathophysiology and clinical features of osteomalacia and rickets. Prepare for your board exam with these essential questions and explanations.
Master ABOS Board Review: Scleroderma, Dwarfism, Infections, Osteomalacia | Part 26
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
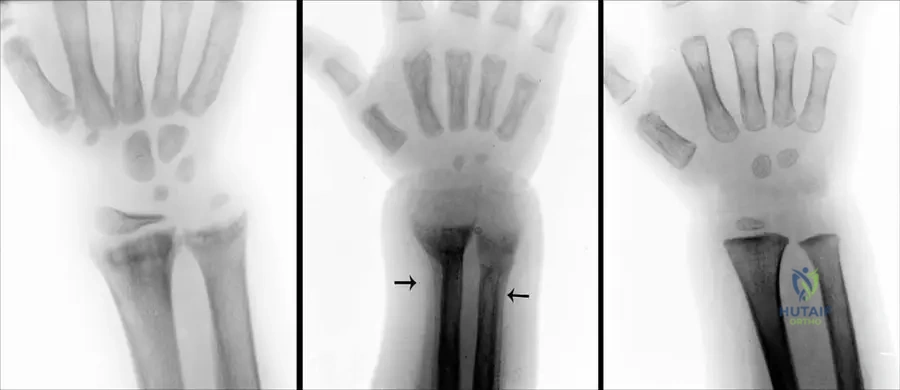
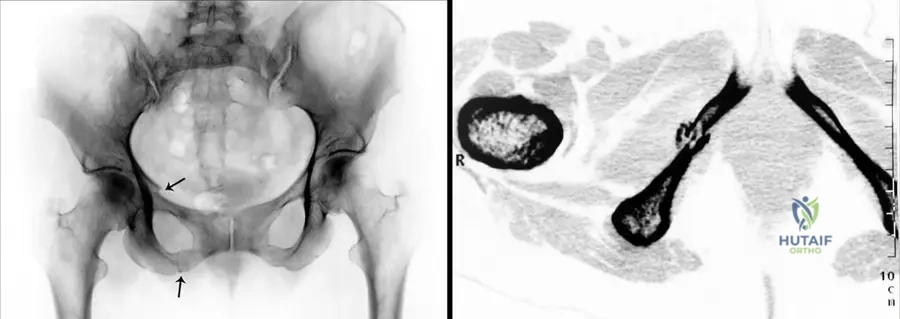
A 55-year-old female presents with vague generalized bone pain and proximal muscle weakness. Pelvic radiograph shows a transverse radiolucency in the superior pubic ramus.
Which of the following laboratory profiles is most consistent with her diagnosis?
Which of the following laboratory profiles is most consistent with her diagnosis?

Explanation
The patient has osteomalacia, characterized by defective bone mineralization resulting in Looser zones (pseudofractures). Laboratory findings typically include low to normal calcium, low phosphate, elevated alkaline phosphatase, and secondary hyperparathyroidism.
Question 2
A 42-year-old female with a history of systemic sclerosis presents with severe pain and a non-healing ulcer on the tip of her index finger. Radiographs show resorption of the terminal phalangeal tuft. Which of the following autoantibodies is most strongly associated with this specific radiographic finding?
Explanation
Acro-osteolysis and calcinosis cutis are classic hand manifestations of limited cutaneous systemic sclerosis (CREST syndrome). This syndrome is most strongly associated with anti-centromere antibodies.
Question 3
A 6-month-old male with a known FGFR3 mutation presents with failure to thrive and episodes of central sleep apnea. What is the most appropriate next step in management?
Explanation
Central sleep apnea in an infant with achondroplasia is highly suggestive of cervicomedullary compression at the foramen magnum. An MRI is required to evaluate the severity of stenosis before considering urgent suboccipital decompression.
Question 4
A 2-year-old child presents with a limp and refuses to bear weight. Laboratory tests show an ESR of 45 mm/h and a CRP of 3.2 mg/dL. Joint aspiration reveals 60,000 WBCs/mcL. Standard agar cultures show no growth at 48 hours. What is the most likely causative organism?
Explanation
Kingella kingae is a fastidious Gram-negative organism and is now a leading cause of septic arthritis in children aged 6 to 36 months. It requires inoculation into BACTEC blood culture bottles or prolonged culture for optimal isolation.
Question 5
A 48-year-old male develops progressive lower extremity weakness and multiple insufficiency fractures. Laboratory workup reveals profound hypophosphatemia, normal calcium, normal parathyroid hormone, and inappropriately low 1,25-dihydroxyvitamin D. What is the pathophysiologic mechanism of this patient's condition?
Explanation
This presentation is classic for tumor-induced (oncogenic) osteomalacia. It is caused by a benign mesenchymal tumor secreting FGF-23, which inhibits both renal phosphate reabsorption and 1-alpha-hydroxylase activity.
Question 6
A newborn is noted to have short-limbed dwarfism, bilateral clubfeet, hitchhiker thumbs, and swelling of the external ear pinnae. A defect in which of the following is most likely responsible for this condition?
Explanation
Diastrophic dysplasia is an autosomal recessive disorder caused by a mutation in the SLC26A2 gene, which encodes a sulfate transporter. This leads to under-sulfated proteoglycans in cartilage, manifesting clinically with cauliflower ears and hitchhiker thumbs.
Question 7
A 62-year-old male presents with increasing pain and malodorous drainage from a chronic sinus tract in his tibia that has been present for 35 years following an open fracture. A recent biopsy of the tract reveals malignant cells. What is the most common histologic subtype of this malignancy?
Explanation
Marjolin's ulcer is a rare, aggressive malignancy arising in chronically inflamed or scarred skin, such as a chronic osteomyelitis draining sinus tract. Squamous cell carcinoma is the most common histologic type, often requiring wide excision or amputation.
Question 8
A 50-year-old female with systemic sclerosis presents with a painfully ischemic, cyanotic long finger digit despite conservative warming measures. Which of the following medications acts as a first-line therapy to promote vasodilation in this acute setting?
Explanation
Raynaud's phenomenon in scleroderma can lead to severe digital ischemia and tissue loss. Calcium channel blockers like nifedipine are the first-line medical therapy to induce vasodilation and improve peripheral perfusion.
Question 9
A 5-year-old boy presents with progressive bowing of his legs and short stature. His mother has a similar history and required bilateral corrective osteotomies as a teenager. Genetic testing confirms a PHEX mutation. Which of the following is the hallmark of the indicated medical treatment?
Explanation
X-linked hypophosphatemic rickets is caused by a PHEX mutation resulting in elevated FGF-23 and renal phosphate wasting. Treatment requires supplementation with both oral phosphate and active vitamin D (calcitriol) to prevent secondary hyperparathyroidism.
Question 10
A 7-year-old boy with a known type II collagen (COL2A1) mutation is scheduled for bilateral hip reconstruction due to coxa vara. Preoperative assessment must include which of the following imaging modalities?
Explanation
Spondyloepiphyseal dysplasia congenita (SEDc) is associated with odontoid hypoplasia and atlantoaxial instability. Preoperative cervical spine clearance is mandatory to prevent catastrophic spinal cord injury during anesthesia intubation.
Question 11
A 65-year-old male undergoes a two-stage revision for a chronic prosthetic joint infection. The organism isolated is Methicillin-sensitive Staphylococcus aureus. The success of targeted antibiotic therapy in this setting depends heavily on penetrating a biofilm. Which of the following antibiotics is most critical to include in the regimen for its unique anti-biofilm activity?
Explanation
Staphylococcal species produce a thick exopolysaccharide glycocalyx biofilm that protects sessile bacteria from standard antibiotics. Rifampin has unique efficacy in penetrating biofilms and is typically used adjunctively in orthopaedic implant infections.
Question 12
A 9-year-old girl presents with waddling gait, short stature, and early-onset osteoarthritis of the hips. Her facial features are entirely normal. Radiographs reveal delayed, fragmented epiphyseal ossification and normal interpedicular distances in the lumbar spine. Which gene is most likely mutated?
Explanation
Pseudoachondroplasia is caused by mutations in the Cartilage Oligomeric Matrix Protein (COMP) gene. Unlike achondroplasia, these patients have normal facial features, normal intelligence, and lack spinal stenosis (due to normal interpedicular distances).
Question 13
A 50-year-old patient with end-stage renal disease undergoes a transiliac bone biopsy. The histomorphometric analysis demonstrates wide osteoid seams and an increased mineralization lag time.
Which of the following underlying mechanisms best explains this specific finding?
Which of the following underlying mechanisms best explains this specific finding?
Explanation
Osteomalacia in renal osteodystrophy is characterized by wide osteoid seams due to defective mineralization. This results primarily from the failing kidney's inability to synthesize 1-alpha-hydroxylase, causing a deficiency in active vitamin D.
Question 14
A 14-year-old female presents for evaluation of shoulder hypermobility. She can easily approximate her shoulders anteriorly in the midline. Examination reveals delayed eruption of permanent teeth. What is the genetic inheritance pattern and associated gene mutation for this condition?
Explanation
Cleidocranial dysplasia presents with hypoplastic or absent clavicles, delayed cranial suture closure, and dental abnormalities. It is inherited in an autosomal dominant pattern due to a mutation in the RUNX2 (CBFA1) transcription factor.
Question 15
A 7-year-old child with sickle cell disease presents with fever, focal tibial pain, and swelling. MRI suggests diaphyseal osteomyelitis. Aspiration and blood cultures yield a Gram-negative, motile, non-lactose fermenting bacillus. What is the most appropriate directed antibiotic therapy?
Explanation
Children with sickle cell disease are uniquely predisposed to Salmonella osteomyelitis, which is a Gram-negative, non-lactose fermenting bacillus. Third-generation cephalosporins (like ceftriaxone) or fluoroquinolones are the treatments of choice.
Question 16
A 12-year-old boy presents with mild short stature, generalized joint pain, and an early waddling gait. Radiographs show delayed epiphyseal ossification in multiple joints and a double-layered appearance of the patella on the lateral view. Spine radiographs are notably normal. What is the most likely diagnosis?
Explanation
Multiple epiphyseal dysplasia (MED) primarily affects the epiphyses with minimal spinal involvement, differentiating it from spondyloepiphyseal dysplasia (SED). The double-layered patella is a classic radiographic hallmark of the disease.
Question 17
Which of the following radiographic findings is most characteristic of the spine in a patient with achondroplasia?
Explanation
In achondroplasia, the interpedicular distance classically narrows from L1 to L5, unlike the normal widening seen in unaffected individuals. This anatomic anomaly heavily predisposes these patients to severe lumbar spinal stenosis.
Question 18
A 45-year-old female with systemic sclerosis (scleroderma) presents with chronic hand pain and fingertip ulcerations. Which of the following radiographic findings is most specifically associated with her condition?
Explanation
Acro-osteolysis, which is the resorption of the terminal phalangeal tufts, along with calcinosis cutis, are classic radiographic manifestations of scleroderma in the hand. These occur secondary to severe microvascular ischemia.
Question 19
A 55-year-old man presents with generalized bone pain and profound muscle weakness. Laboratory studies reveal hypophosphatemia, normal serum calcium, elevated alkaline phosphatase, and elevated FGF-23 levels. What is the most likely etiology of his osteomalacia?
Explanation
Tumor-induced (oncogenic) osteomalacia is a paraneoplastic syndrome caused by small phosphaturic mesenchymal tumors that inappropriately secrete FGF-23. Elevated FGF-23 leads to profound renal phosphate wasting and subsequent osteomalacia.
Question 20
A newborn is evaluated for severe limb shortening, a 'hitchhiker thumb' deformity, cauliflower ears, and a rigid cervical kyphosis. A mutation in which of the following genes is responsible for this condition?
Explanation
Diastrophic dysplasia is an autosomal recessive condition caused by a defect in the sulfate transporter gene, SLC26A2. Classic clinical features include the hitchhiker thumb, cauliflower ear deformity, and severe cervical kyphosis.
Question 21
When treating a periprosthetic joint infection caused by Staphylococcus aureus with retention of the hardware, rifampin is often added to the antibiotic regimen. What is the primary mechanism of action of rifampin?
Explanation
Rifampin is highly effective against biofilm-associated Staphylococci in periprosthetic joint infections due to its ability to penetrate biofilms and target stationary-phase bacteria. It works by inhibiting DNA-dependent RNA polymerase.
Question 22
A 6-year-old boy with X-linked hypophosphatemia (XLH) continues to have progressive lower extremity bowing despite standard oral phosphate and calcitriol therapy. Which of the following targeted therapies directly addresses the underlying pathophysiology?
Explanation
Burosumab is an FDA-approved monoclonal antibody that binds to and inhibits FGF-23. It is a highly effective targeted therapy for X-linked hypophosphatemia (XLH), addressing the root cause of the renal phosphate wasting.
Question 23
An infant with achondroplasia is being evaluated by a pediatric orthopedist. The parents report episodes of apnea and increased tone in the extremities. What is the most critical anatomical region to evaluate immediately?
Explanation
Foramen magnum stenosis in achondroplasia can cause lethal cervicomedullary compression, presenting as central sleep apnea, hypotonia, or hyperreflexia. Immediate evaluation with an MRI of the craniocervical junction is required.
Question 24
A 45-year-old female presents with diffuse bone pain. Radiographs demonstrate bilateral pseudofractures of the medial femoral neck.
If an iliac crest bone biopsy with double tetracycline labeling is performed, what is the expected histologic finding?
If an iliac crest bone biopsy with double tetracycline labeling is performed, what is the expected histologic finding?
Explanation
The classic histologic finding in osteomalacia is an excess of unmineralized osteoid (increased osteoid seam width) and a prolonged mineralization lag time on tetracycline labeling. Radiographically, Looser zones (pseudofractures) are a hallmark sign.
Question 25
In children, acute hematogenous osteomyelitis most frequently affects which specific anatomic region of the long bone?
Explanation
Pediatric acute hematogenous osteomyelitis typically begins in the metaphysis. The sluggish blood flow in the looping venous sinusoids adjacent to the physis creates an ideal low-oxygen environment for bacterial seeding.
Question 26
A 5-year-old child presents with disproportionate short stature and waddling gait. Unlike typical achondroplasia, the child has completely normal facial features and head circumference. Genetic testing reveals a mutation in the COMP gene. What is the diagnosis?
Explanation
Pseudoachondroplasia is caused by a mutation in the Cartilage Oligomeric Matrix Protein (COMP) gene. Unlike achondroplasia, patients have normal facial features and head size, but suffer from disproportionate short stature and early-onset osteoarthritis.
Question 27
A patient with CREST syndrome is referred for orthopedic evaluation of painful subcutaneous nodules in the digits that occasionally extrude a chalky white material. Which specific autoantibody is most closely associated with this patient's systemic disease?
Explanation
CREST syndrome (a limited cutaneous form of scleroderma) is strongly associated with Anti-centromere antibodies. The chalky white extrusions describe calcinosis cutis, the 'C' in CREST.
Question 28
Which of the following statements most accurately distinguishes the underlying pathophysiology of osteomalacia from that of osteoporosis?
Explanation
Osteomalacia is fundamentally a defect in bone mineralization, resulting in unmineralized osteoid and a decreased mineral-to-matrix ratio. Osteoporosis involves a loss of total bone mass, but the remaining bone has a normal mineral-to-matrix ratio.
Question 29
In the pathogenesis of periprosthetic joint infections, what is the primary function of the bacterial glycocalyx?
Explanation
The glycocalyx (exopolysaccharide matrix) is a defining feature of bacterial biofilms in orthopedic implant infections. It acts as a mechanical and biochemical barrier that protects stationary-phase bacteria from both antibiotics and host immune clearance.
Question 30
A 4-year-old child presents with a short trunk, severe coxa vara, and atlantoaxial instability. Radiographs demonstrate delayed ossification of the capital femoral epiphyses and a barrel-shaped chest. Genetic testing reveals a mutation in COL2A1. What is the diagnosis?
Explanation
Spondyloepiphyseal dysplasia congenita (SEDC) is a type II collagenopathy caused by mutations in the COL2A1 gene. It classically presents with a short trunk, coxa vara, and atlantoaxial instability.
Question 31
A 10-year-old patient with achondroplasia develops progressive symptomatic genu varum. What is the primary anatomical driver of this deformity?
Explanation
Genu varum in achondroplasia is primarily caused by asymmetric growth, specifically the overgrowth of the fibula relative to the shorter tibia. This creates a deforming force that bows the tibia into varus.
Question 32
Which of the following correctly describes Kingella kingae, an increasingly recognized cause of pediatric osteoarticular infections?
Explanation
Kingella kingae is a fastidious Gram-negative bacillus and is a leading cause of septic arthritis and osteomyelitis in children aged 6 months to 4 years. Because it is difficult to culture on standard solid media, it is best isolated by inoculating synovial fluid directly into blood culture vials or using PCR.
Question 33
A hand surgeon is contemplating soft tissue release for severe joint contractures in a patient with diffuse cutaneous systemic sclerosis (scleroderma). What is the most critical perioperative complication the surgeon must anticipate?
Explanation
Patients with scleroderma suffer from severe peripheral microvascular disease (e.g., advanced Raynaud's). Any surgical intervention in the hand carries an exceedingly high risk of digital ischemia, necrosis, and non-healing wounds.
Question 34
A 2-year-old child presents with rickets-like skeletal deformities and early loss of deciduous teeth. Laboratory analysis shows marked osteomalacia with a notably low serum alkaline phosphatase level. What is the primary underlying defect?
Explanation
Hypophosphatasia is an inborn error of metabolism caused by mutations in the ALPL gene, leading to deficient tissue-nonspecific alkaline phosphatase (TNSALP) activity. It mimics rickets or osteomalacia radiographically but is distinctly characterized by low serum alkaline phosphatase.
Question 35
A child with a known mucopolysaccharidosis presents with progressive myelopathy. Radiographs reveal severe odontoid hypoplasia and atlantoaxial instability. Biochemical testing shows abnormal accumulation of keratan sulfate. Which syndrome does this patient have?
Explanation
Morquio syndrome (MPS IV) is characterized by the inability to degrade keratan sulfate. A hallmark and highly dangerous orthopedic manifestation of Morquio syndrome is odontoid hypoplasia, which leads to severe atlantoaxial instability and potential cervical myelopathy.
Question 36
In the lifecycle of a bacterial biofilm associated with orthopedic implants, what is the final stage that facilitates the spread of infection to new sites?
Explanation
The biofilm lifecycle consists of initial attachment, irreversible adherence, matrix maturation, and finally, detachment or dispersal. During dispersal, clumps of bacteria or planktonic cells are released to seed new areas, propagating the infection.
Question 37
A 4-year-old boy presents with progressive bowing of the lower extremities. Labs show normal serum calcium, low serum phosphate, and elevated alkaline phosphatase. Genetic testing reveals a mutation in the PHEX gene. Which of the following is the primary mechanism of this disease?
Explanation
X-linked hypophosphatemic rickets is caused by a PHEX mutation, resulting in excessive FGF23. Elevated FGF23 causes renal phosphate wasting and impairs 1-alpha-hydroxylase, leading to defective bone mineralization.
Question 38
A 45-year-old female with a history of systemic sclerosis presents with progressive shortening of her distal fingers and painful, chalky subcutaneous nodules on her fingertips. Radiographs reveal resorption of the terminal phalangeal tufts. What is the most appropriate initial management for the subcutaneous nodules if they become acutely inflamed but lack signs of systemic infection?
Explanation
The patient has calcinosis cutis and acro-osteolysis secondary to scleroderma. Initial treatment is medical with calcium channel blockers or intralesional steroids, as surgical excision is fraught with poor wound healing and infection risk.
Question 39
A 35-year-old male with achondroplasia presents with neurogenic claudication. He reports leg pain and numbness after walking 50 meters, which is relieved by sitting. Radiographs of the lumbar spine will most likely demonstrate which of the following anatomic abnormalities?
Explanation
Achondroplasia causes a characteristic progressive decrease in the interpedicular distance from L1 to L5, leading to severe lumbar spinal stenosis. This results in classic symptoms of neurogenic claudication.
Question 40
A 65-year-old male presents with chronic pain in his total knee arthroplasty, performed 3 years ago. Aspiration yields 3,500 WBC/uL with 75% PMNs. Alpha-defensin is positive. Synovial CRP is elevated. According to the 2018 ICM criteria, what is the next best step in management?
Explanation
The patient meets criteria for chronic periprosthetic joint infection (PJI). The gold standard treatment for chronic PJI in North America is a two-stage revision with an antibiotic spacer.
Question 41
A 52-year-old male presents with severe diffuse bone pain and muscle weakness. Radiographs reveal multiple pseudofractures (Looser zones).
Labs demonstrate marked hypophosphatemia. A whole-body DOTATATE PET scan reveals a small soft-tissue mass in the plantar aspect of the foot. Resection of this mass will most likely normalize the level of which of the following?
Labs demonstrate marked hypophosphatemia. A whole-body DOTATATE PET scan reveals a small soft-tissue mass in the plantar aspect of the foot. Resection of this mass will most likely normalize the level of which of the following?
Explanation
This is a classic presentation of tumor-induced (oncogenic) osteomalacia. The tumor autonomously secretes FGF23, which causes renal phosphate wasting; excision of the tumor cures the condition.
Question 42
A newborn is evaluated for multiple musculoskeletal anomalies. Examination reveals severe shortening of the limbs, bilateral clubfeet, "hitchhiker" thumbs, and swelling of the external ears (cauliflower ears). A mutation in which of the following genes is responsible for this condition?
Explanation
Diastrophic dysplasia is characterized by short stature, hitchhiker thumbs, cauliflower ears, and severe clubfeet. It is an autosomal recessive disorder caused by a mutation in the SLC26A2 sulfate transporter gene.
Question 43
A 50-year-old female with limited cutaneous systemic sclerosis (CREST syndrome) complains of hand stiffness and Raynaud's phenomenon. Which of the following autoantibodies is most highly associated with this patient's specific subtype of scleroderma?
Explanation
Anti-centromere antibodies are highly sensitive and specific for limited cutaneous systemic sclerosis (CREST syndrome). Anti-Scl-70 is associated with diffuse cutaneous systemic sclerosis.
Question 44
A 14-month-old girl presents with a limp and refusal to bear weight on the right leg. She has a low-grade fever and a recent upper respiratory infection. Inflammatory markers are mildly elevated. Blood cultures are negative, but a joint aspiration of the knee grows a fastidious Gram-negative coccobacillus on blood agar. What is the most likely causative organism?
Explanation
Kingella kingae is a common cause of pediatric septic arthritis and osteomyelitis in children under 4 years old. It is a fastidious Gram-negative organism that often follows upper respiratory infections.
Question 45
A bone biopsy from a patient with undiagnosed metabolic bone disease demonstrates abundant unmineralized osteoid seams that are abnormally thick (>15 micrometers). The mineralization lag time is significantly increased.
Which of the following conditions is most consistent with these histological findings?
Which of the following conditions is most consistent with these histological findings?
Explanation
Thickened, unmineralized osteoid seams and an increased mineralization lag time are the hallmark histological features of osteomalacia. This reflects defective mineralization of newly formed bone.
Question 46
A 5-year-old child presents with disproportionate short stature characterized by a short trunk and barrel chest. Radiographs reveal platyspondyly, delayed ossification of the femoral heads, and severe coxa vara. Visual and hearing assessments show myopia and sensorineural hearing loss. The primary defect involves which of the following collagens?
Explanation
Spondyloepiphyseal dysplasia congenita (SEDC) affects the spine and epiphyses, causing a short-trunk dwarfism with visual and hearing impairments. It is caused by mutations in the COL2A1 gene, which encodes Type II collagen.
Question 47
A 72-year-old male with an infected total hip arthroplasty undergoes a two-stage revision. During the extraction of the components, thick biofilm is noted on the prosthesis. Which of the following describes the primary characteristic of the bacteria within the deeper layers of this biofilm?
Explanation
Bacteria embedded deep within a biofilm enter a stationary phase with a lowered metabolic rate (persister cells). This makes them highly recalcitrant to traditional antibiotics that target actively dividing cells.
Question 48
A patient with scleroderma presents with severe, refractory digital ischemia secondary to Raynaud's phenomenon, which has not responded to calcium channel blockers and PDE-5 inhibitors. What surgical intervention may be considered to improve digital perfusion?
Explanation
For refractory digital ischemia in scleroderma, digital sympathectomy involving stripping adventitia from the superficial palmar arch and digital arteries can relieve vasospasm. This helps heal ulcers and restore perfusion.
Question 49
A 7-year-old child presents with short-limb dwarfism, joint laxity, and early-onset osteoarthritis. Unlike achondroplasia, the patient's facial features and head circumference are completely normal. Radiographs show delayed epiphyseal ossification and irregular metaphyses. A mutation in the COMP (Cartilage Oligomeric Matrix Protein) gene is identified. What is the diagnosis?
Explanation
Pseudoachondroplasia presents with severe short-limb dwarfism but normal facies and normal intelligence, caused by a COMP gene mutation. Multiple epiphyseal dysplasia (MED) can also have COMP mutations but typically lacks the severe short-limb dwarfism seen here.
Question 50
A 60-year-old female with end-stage renal disease on hemodialysis presents with bilateral hip pain. Radiographs reveal pseudofractures in the femoral neck. Lab values show elevated PTH, hyperphosphatemia, and hypocalcemia. What is the primary cause of her impaired bone mineralization?
Explanation
In chronic kidney disease, the failing kidneys cannot properly convert 25-hydroxyvitamin D to active 1,25-dihydroxyvitamin D. This leads to hypocalcemia, secondary hyperparathyroidism, and renal osteodystrophy (osteomalacia).
Question 51
A 12-year-old boy is diagnosed with acute hematogenous osteomyelitis of the proximal tibia. Cultures grow Methicillin-resistant Staphylococcus aureus (MRSA). The patient has a known severe anaphylactic allergy to vancomycin. Which of the following intravenous antibiotics is the most appropriate alternative for targeting the MRSA?
Explanation
Daptomycin is an excellent bactericidal alternative for MRSA in patients with vancomycin allergies or intolerance. Clindamycin resistance in MRSA is increasing and depends on local antibiograms, making daptomycin a more reliable empiric IV choice.
Question 52
A 6-month-old infant with achondroplasia is noted to have central apnea, brisk deep tendon reflexes, and hypotonia. An MRI of the craniocervical junction is obtained. What is the most critical complication that must be ruled out or treated urgently in this patient?
Explanation
Infants with achondroplasia are at high risk for foramen magnum stenosis, which can cause cervicomedullary compression. Symptoms include sleep apnea, hyperreflexia, and hypotonia, often requiring urgent surgical decompression.
Question 53
An orthopedic surgeon is planning a total joint arthroplasty in a 68-year-old patient with long-standing systemic sclerosis. Which of the following perioperative complications is this patient at the HIGHEST risk of developing compared to the general population?
Explanation
Systemic sclerosis leads to significant microvascular obliteration and skin fibrosis. This places patients at an exceedingly high risk of wound dehiscence, delayed healing, and skin necrosis following surgical incisions.
Question 54
Which of the following radiographic findings is considered pathognomonic for osteomalacia and typically occurs on the compression side of the bone?
Explanation
Looser zones, or pseudofractures, are wide, transverse radiolucencies traversing part of the bone, frequently on the compression side. They are pathognomonic for osteomalacia.
Question 55
A 22-year-old sexually active female presents with acute onset of right knee pain, swelling, and fever. She also reports migrating polyarthralgia over the past three days and a few painless pustular skin lesions on her hands. Synovial fluid aspiration shows 45,000 WBC/uL. What is the most likely pathogen?
Explanation
Disseminated gonococcal infection classically presents in young, sexually active patients with migratory polyarthritis, tenosynovitis, and painless pustular dermatitis. Synovial WBC counts may be lower than those seen in staphylococcal septic arthritis.
Question 56
A 6-year-old boy presents with bilateral hip pain and a waddling gait. Radiographs reveal bilateral, symmetric fragmentation and flattening of the femoral capital epiphyses, with normal acetabuli and normal spine radiographs. His father had similar early-onset arthritis. Which of the following best differentiates this condition from Legg-Calvé-Perthes disease?
Explanation
Multiple Epiphyseal Dysplasia (MED) usually presents with symmetric, bilateral epiphyseal changes and has an autosomal dominant inheritance. Legg-Calvé-Perthes disease is predominantly unilateral and lacks a strong inherited pattern.
Question 57
A 5-year-old boy presents with progressive bowing of the legs and short stature. Labs show normal serum calcium, markedly low serum phosphate, and elevated alkaline phosphatase. Genetic testing reveals a mutation in the PHEX gene. Which of the following best explains the pathophysiology of his condition?
Explanation
X-linked hypophosphatemia is caused by a PHEX gene mutation, leading to decreased degradation and overproduction of FGF23. High FGF23 levels cause decreased renal reabsorption of phosphate, leading to profound hypophosphatemia and defective bone mineralization.
Question 58
A 45-year-old female with a history of systemic sclerosis presents with severe fingertip pain and recurrent ulceration. Radiographs of the hands are most likely to demonstrate which of the following pathognomonic findings?
Explanation
Systemic sclerosis (scleroderma) frequently involves the hand, classically presenting with acro-osteolysis (resorption of the distal phalangeal tufts) and calcinosis cutis. These changes are secondary to severe microvascular ischemia and chronic Raynaud phenomenon.
Question 59
A 6-month-old infant with achondroplasia presents with hypotonia, central apnea during sleep, and hyperreflexia. What is the most appropriate next step in management?
Explanation
Infants with achondroplasia are at high risk for foramen magnum stenosis, which can cause cervicomedullary compression leading to central apnea, hypotonia, and sudden death. MRI of the craniocervical junction is the diagnostic test of choice to evaluate for critical stenosis prior to surgical decompression.
Question 60
A 65-year-old man presents with acute onset of right knee pain, swelling, and fever 3 weeks after a primary total knee arthroplasty. Aspiration yields a white blood cell count of 75,000 cells/uL with 92% neutrophils. The implant is well-fixed. What is the most appropriate surgical management?
Explanation
Debridement, antibiotics, and implant retention (DAIR) with modular polyethylene exchange is indicated for early postoperative prosthetic joint infections (typically within 4 weeks of surgery). It relies on a well-fixed prosthesis and a healthy soft tissue envelope.
Question 61
A 52-year-old man presents with diffuse bone pain and proximal muscle weakness. Laboratory studies show hypophosphatemia, normal serum calcium, normal PTH, and elevated FGF23. A small mesenchymal tumor is found in his thigh. Complete surgical excision of the tumor will most likely lead to which of the following?
Explanation
Tumor-induced (oncogenic) osteomalacia is a paraneoplastic syndrome where a phosphaturic mesenchymal tumor secretes excess FGF23, causing renal phosphate wasting. Complete surgical excision is curative, leading to rapid normalization of phosphate and vitamin D levels.
Question 62
A newborn presents with short stature, severe rigid clubfeet, 'hitchhiker' thumbs, and cystic swelling of the pinnae (cauliflower ears). Which of the following gene mutations is most likely responsible for this condition?
Explanation
Diastrophic dysplasia is an autosomal recessive disorder caused by a mutation in the SLC26A2 (DTDST) gene, which affects a sulfate transporter. It is characterized by hitchhiker thumbs, rigid equinovarus foot deformities, and auricular cysts.
Question 63
A 45-year-old strict vegan presents with generalized bone pain and a waddling gait. Radiographs show transverse radiolucent bands in the femoral neck and pubic rami. If a bone biopsy were performed following double tetracycline labeling, what would be the expected finding?
Explanation
The patient has nutritional osteomalacia characterized by Looser zones (pseudofractures). Histomorphometry with double tetracycline labeling would show a decreased distance between labels (low mineralization rate) and widened unmineralized osteoid seams.
Question 64
A 2-year-old child presents with a limp, low-grade fever, and refusal to bear weight on the right leg. Hip aspiration yields synovial fluid with a WBC count of 45,000 cells/uL. Standard Gram stain and routine cultures are negative at 48 hours. What is the most appropriate method to identify the most likely causative organism?
Explanation
Kingella kingae is the most common cause of septic arthritis in children under 4 years old. It is a fastidious organism that is notoriously difficult to grow on solid media; inoculation into blood culture vials or PCR significantly increases detection.
Question 65
A 50-year-old female with the CREST variant of scleroderma presents with a gangrenous tip of her index finger due to severe Raynaud phenomenon. She has failed conservative management. Before proceeding with surgical amputation, what intervention is recommended to optimize healing of the adjacent tissue?
Explanation
In patients with scleroderma and severe ischemic ulcerations failing medical therapy, digital sympathectomy and adventitial stripping can improve digital perfusion. This optimizes tissue viability and wound healing potential prior to or during surgical amputation.
Question 66
Which of the following cervical spine manifestations is most characteristic of Spondyloepiphyseal Dysplasia Congenita (SEDC) but NOT typical for Achondroplasia?
Explanation
SEDC is a type II collagenopathy characterized by severe epiphyseal dysplasia and odontoid hypoplasia, leading to marked atlantoaxial instability. In contrast, achondroplasia is classically associated with foramen magnum stenosis, not atlantoaxial instability.
Question 67
A 45-year-old female presents with tightening of the skin on her fingers, dysphagia, and cold-induced digital vasospasm. Radiographs of her hands are most likely to demonstrate which of the following classic findings?
Explanation
This patient has CREST syndrome (limited scleroderma). Classic hand radiographic findings include acro-osteolysis (resorption of the distal tufts) and calcinosis cutis.
Question 68
Achondroplasia is characterized by a disproportionate short stature. Which of the following accurately describes the primary genetic and cellular etiology of this condition?
Explanation
Achondroplasia is caused by a gain-of-function mutation in the FGFR3 gene. This overactivity abnormally inhibits chondrocyte proliferation within the proliferative zone of the physis.
Question 69
A 60-year-old female with a history of celiac disease presents with generalized bone pain and proximal muscle weakness. Her radiographs demonstrate pseudofractures.
Which of the following laboratory profiles is most consistent with her diagnosis?
Which of the following laboratory profiles is most consistent with her diagnosis?

Explanation
This patient has osteomalacia secondary to malabsorption (Vitamin D deficiency). This leads to low calcium and phosphate levels, which triggers a secondary hyperparathyroidism and elevated alkaline phosphatase.
Question 70
A 7-year-old boy with sickle cell disease presents with fever, focal tibial pain, and swelling. While Staphylococcus aureus remains the most common overall cause of osteomyelitis in this population, which of the following organisms is disproportionately more prevalent in patients with this underlying disease compared to the general pediatric population?
Explanation
Patients with sickle cell disease have functional asplenia and a uniquely high susceptibility to Salmonella osteomyelitis, although S. aureus still remains the most common cause overall.
Question 71
A newborn is evaluated for skeletal dysplasia. Examination reveals severe micromelia, "hitchhiker" thumbs, clubfeet, and cystic swelling of the pinnae (cauliflower ear). What is the underlying genetic defect?
Explanation
Diastrophic dysplasia presents with hitchhiker thumbs, severe clubfeet, and cauliflower ears. It is an autosomal recessive condition caused by a mutation in the sulfate transporter gene (SLC26A2/DTDST).
Question 72
A 45-year-old male presents with worsening lower extremity pain, muscle weakness, and multiple rib fractures. Laboratory studies reveal severe hypophosphatemia, normal calcium, elevated alkaline phosphatase, and low 1,25-dihydroxyvitamin D. PTH is normal. A PET scan reveals a small soft-tissue mass in the plantar aspect of his foot. Overproduction of which of the following substances by this tumor is responsible for his condition?
Explanation
Tumor-induced osteomalacia is a paraneoplastic syndrome caused by phosphaturic mesenchymal tumors that secrete FGF23. FGF23 promotes renal phosphate wasting and decreases calcitriol production.
Question 73
A 4-year-old boy presents with an acute onset of a limp and refuses to bear weight on his right leg. His temperature is 38.8°C (101.8°F). Laboratory tests show a WBC count of 13,500/mm³ and an ESR of 55 mm/hr. According to the Kocher criteria, what is the predictive probability that this child has septic arthritis of the hip?
Explanation
The patient has all four Kocher criteria (non-weight-bearing, fever >38.5°C, WBC >12,000, ESR >40). The presence of all 4 criteria yields a 99% probability of septic arthritis.
Question 74
A patient with diffuse systemic sclerosis (scleroderma) requires a reconstructive hand procedure. This patient is known to be at high risk for progressive interstitial lung disease. Which of the following autoantibodies is most highly associated with the diffuse form of this disease and pulmonary fibrosis?
Explanation
Anti-Scl-70 (anti-topoisomerase I) is associated with diffuse systemic sclerosis and a higher risk of interstitial lung disease. Anti-centromere antibodies are primarily linked to limited cutaneous disease (CREST).
Question 75
A 6-year-old child presents with disproportionate short stature, normal craniofacial features, significant ligamentous laxity, and early-onset osteoarthritis of the hips. Radiographs show delayed epiphyseal ossification and platyspondyly with anterior beaking. A defect in which of the following genes is the most likely cause?
Explanation
Pseudoachondroplasia is caused by mutations in the Cartilage Oligomeric Matrix Protein (COMP) gene. It classically presents with normal facies (unlike achondroplasia), severe early osteoarthritis, and ligamentous laxity.
Question 76
A 48-year-old woman presents with generalized bone pain and muscle weakness. Radiographs reveal bilateral radiolucent bands perpendicular to the cortex in her femoral necks.
Histological analysis of these bands would most likely demonstrate an accumulation of which of the following?
Histological analysis of these bands would most likely demonstrate an accumulation of which of the following?
Explanation
The patient has osteomalacia with Looser zones (pseudofractures). Histologically, these zones represent areas of thick, unmineralized osteoid seams due to a defect in bone mineralization.
Question 77
Which of the following describes the underlying pathophysiology of achondroplasia at the level of the physis?
Explanation
Achondroplasia is caused by a gain-of-function mutation in FGFR3, which leads to the constitutional inhibition of chondrocyte proliferation in the proliferative zone of the physis.
Question 78
A 45-year-old female with systemic sclerosis (scleroderma) suffers from severe, medically refractory Raynaud's phenomenon. She is scheduled for a digital sympathectomy. Which of the following is the primary anatomic target during this procedure?
Explanation
Digital sympathectomy for refractory Raynaud's phenomenon involves microsurgical stripping of the adventitia of the common and proper digital arteries, which houses the overactive sympathetic nerve fibers.
Question 79
An 18-month-old child presents with an acute monoarticular effusion of the knee, fever, and refusal to bear weight. Gram stain of the synovial aspirate is negative. Which of the following is the most sensitive method to isolate Kingella kingae from this patient's synovial fluid?
Explanation
Kingella kingae is a fastidious organism responsible for many pediatric joint infections. Its isolation is significantly improved by inoculating synovial fluid directly into aerobic blood culture vials (BACTEC).
Question 80
A 50-year-old male presents with profound muscle weakness and multiple pseudofractures. Laboratory studies show hypophosphatemia, normocalcemia, normal PTH, and inappropriately low 1,25-dihydroxyvitamin D. Which of the following is the most likely etiology?
Explanation
This profile is classic for tumor-induced osteomalacia. A phosphaturic mesenchymal tumor secretes FGF23, which causes renal phosphate wasting and inhibits 1-alpha-hydroxylase, reducing active vitamin D.
Question 81
A newborn presents with rhizomelic short stature, bilateral clubfeet, "hitchhiker" thumbs, and cystic swelling of the pinnae. Mutations in the SLC26A2 gene are suspected. Which of the following spinal deformities is most characteristic of this condition?
Explanation
The patient has diastrophic dysplasia (SLC26A2 mutation). A hallmark and potentially life-threatening complication of this condition is progressive cervical kyphosis, which can cause neurologic compromise.
Question 82
A 70-year-old man underwent a total hip arthroplasty 3 years ago. He had a dental extraction 4 weeks ago and now presents with 3 days of severe hip pain, erythema, and a temperature of 38.8°C. Aspiration yields 85,000 WBC/uL (95% neutrophils). What is the most appropriate initial surgical management?
Explanation
This is an acute hematogenous periprosthetic joint infection (symptoms < 3 weeks, well-fixed implants). The standard of care is DAIR (Debridement, Antibiotics, Implant Retention) with exchange of modular components.
Question 83
Acro-osteolysis of the distal phalanges is frequently observed in patients with systemic sclerosis. Which of the following best describes the primary pathogenesis of this finding?
Explanation
Acro-osteolysis (resorption of the terminal phalangeal tufts) in systemic sclerosis is primarily driven by chronic tissue ischemia resulting from severe microvascular disease and Raynaud's phenomenon.
Question 84
An 8-month-old male with achondroplasia presents for routine follow-up. Radiographs demonstrate a 30-degree thoracolumbar kyphosis. Neurologic exam is normal. What is the most appropriate management of the spinal deformity?
Explanation
Thoracolumbar kyphosis is common in infants with achondroplasia due to hypotonia. It typically resolves spontaneously once the child begins to walk independently, so observation is the initial standard of care.
Question 85
A 35-year-old patient on long-term phenytoin therapy develops osteomalacia. Which of the following best explains the mechanism of antiepileptic-induced bone disease?
Explanation
Phenytoin and phenobarbital induce hepatic cytochrome P450 enzymes. This accelerates the catabolism of vitamin D into inactive metabolites, leading to decreased calcium absorption and subsequent osteomalacia.
Question 86
A 5-year-old boy presents with short-trunk dwarfism, a waddling gait, myopia, and a history of cleft palate. Radiographs show delayed ossification of the femoral heads and severe coxa vara. He is diagnosed with spondyloepiphyseal dysplasia (SED) congenita. This disorder is caused by a mutation affecting which of the following proteins?
Explanation
SED congenita is an autosomal dominant skeletal dysplasia caused by a mutation in the COL2A1 gene, resulting in defective Type II collagen. It affects articular cartilage and the nucleus pulposus.
Question 87
A 60-year-old diabetic patient presents with acute, severe leg pain out of proportion to exam findings, swelling, and bullae. In the operating room, an incision reveals "dishwater pus" and non-bleeding fascia. Which of the following is the most critical intervention for patient survival?
Explanation
The clinical picture describes necrotizing fasciitis. While antibiotics are necessary, immediate and aggressive surgical debridement of all necrotic tissue is the most critical step to prevent mortality.
Question 88
To confirm a suspected diagnosis of osteomalacia and assess bone turnover dynamics, an undecalcified bone biopsy is obtained.
Which of the following labeling agents is administered prior to the biopsy to evaluate the mineralization apposition rate?
Which of the following labeling agents is administered prior to the biopsy to evaluate the mineralization apposition rate?
Explanation
Double tetracycline labeling involves giving tetracycline courses spaced out over time. It binds to newly mineralized bone, allowing measurement of the mineralization apposition rate on an undecalcified biopsy under fluorescent light.
Question 89
In a patient with CREST syndrome, which of the following represents the most widely accepted orthopedic indication for surgical excision of calcinosis cutis lesions?
Explanation
Calcinosis cutis in CREST syndrome is generally managed nonoperatively. Surgery is indicated primarily when lesions become painful, exophytic, and cause skin breakdown leading to recurrent infections.
Question 90
An adult male with achondroplasia presents with progressive neurogenic claudication and lower extremity weakness. Which of the following distinct anatomic features of the achondroplastic spine most directly causes this pathology?
Explanation
Achondroplasia features a progressive narrowing of the interpedicular distance from the upper to the lower lumbar spine, combined with short pedicles, leading to severe congenital spinal stenosis.
Question 91
Which of the following organisms is most heavily reliant on the production of a polysaccharide glycocalyx (slime layer) to adhere to orthopedic implants and evade host immune responses in chronic periprosthetic joint infections?
Explanation
Staphylococcus epidermidis is notorious for forming a thick glycocalyx biofilm on foreign bodies, which facilitates adherence and protects the bacteria from both systemic antibiotics and host phagocytosis.
Question 92
A 3-year-old child presents with short stature, ligamentous laxity, and a waddling gait. He had a normal appearance at birth and has a normal facial appearance. Radiographs show fragmented epiphyses. A mutation in the COMP gene is confirmed. What is the diagnosis?
Explanation
Pseudoachondroplasia is caused by a mutation in the COMP gene. Unlike achondroplasia, children are normal at birth, lack facial involvement, and exhibit marked joint laxity.
Question 93
A 5-year-old girl is diagnosed with X-linked hypophosphatemic rickets (PHEX mutation). Which of the following is the gold standard medical therapy to prevent progression of skeletal deformity?
Explanation
Treatment for X-linked hypophosphatemia requires oral phosphate supplementation. Calcitriol must also be added to prevent secondary hyperparathyroidism, which would otherwise be triggered by the phosphate load.
Question 94
During surgical debridement of chronic osteomyelitis, the surgeon removes a piece of dense, isolated bone. By definition, a sequestrum represents which of the following?
Explanation
In chronic osteomyelitis, a sequestrum is a piece of dead, necrotic bone that has become separated from the surrounding living bone. An involucrum is the shell of new reactive bone forming around it.
Question 95
A 60-year-old female presents with severe hand deformities. Radiographs reveal prominent resorption of the terminal phalangeal tufts, preservation of the joint spaces, and diffuse subcutaneous calcifications. Marginal erosions are absent. This radiographic pattern is most pathognomonic for which of the following diseases?
Explanation
Acro-osteolysis (resorption of the terminal tufts) combined with soft tissue calcification (calcinosis cutis) and preservation of joint spaces is a hallmark radiographic presentation of systemic sclerosis (scleroderma).
Question 96
A 48-year-old female with a history of Roux-en-Y gastric bypass presents with diffuse bone pain, muscle weakness, and a waddling gait. Radiographs demonstrate the findings shown in the provided image.
Which of the following best describes the primary underlying histologic pathogenesis of this condition?
Which of the following best describes the primary underlying histologic pathogenesis of this condition?
Explanation
Osteomalacia is characterized by impaired mineralization of the bone matrix, leading to wide, unmineralized osteoid seams. The radiographic presence of pseudofractures (Looser zones) is a pathognomonic finding in advanced cases.
Question 97
A 12-month-old male with achondroplasia is brought to the clinic by his parents due to a noticeable "hump" in his lower back. Physical examination reveals a flexible thoracolumbar kyphosis that corrects when the child is suspended prone. Neurological examination is unremarkable. What is the most appropriate initial management?
Explanation
Thoracolumbar kyphosis is common in infants with achondroplasia and typically resolves spontaneously as the child develops truncal muscle tone and begins to walk. Bracing or surgery is strictly reserved for progressive, rigid deformities or those associated with neurological compromise.
Question 98
A 5-year-old child presents with disproportionate short stature, a waddling gait, and profound joint laxity. Unlike classic achondroplasia, the child has completely normal facial features and intelligence. Radiographs show delayed epiphyseal ossification and irregular, fragmented metaphyses. A mutation in which of the following genes is most likely responsible?
Explanation
Pseudoachondroplasia is an autosomal dominant skeletal dysplasia caused by mutations in the Cartilage Oligomeric Matrix Protein (COMP) gene. It is clinically distinguished from achondroplasia by the presence of normal craniofacial features and the absence of clinical manifestations at birth.
Question 99
A 54-year-old female with long-standing diffuse systemic sclerosis (scleroderma) presents with progressive, painful flexion contractures of her proximal and distal interphalangeal joints bilaterally. Radiographs show acro-osteolysis but no periarticular erosions. Which of the following is the most likely primary cause of her joint contractures?
Explanation
Joint contractures in systemic sclerosis are primarily caused by progressive fibrosis, induration, and tightening of the skin and periarticular soft tissues. Primary erosive arthropathy is rare in scleroderma unless there is an overlapping rheumatoid syndrome.
Question 100
A 2-year-old child presents with a low-grade fever, limp, and refusal to bear weight on the right leg. Inflammatory markers are only mildly elevated. A knee aspirate yields purulent synovial fluid, but standard Gram stain is negative. Which of the following fastidious pathogens is highly suspected and best identified using nucleic acid amplification testing (PCR)?
Explanation
Kingella kingae is a leading cause of osteoarticular infections in children aged 6 months to 4 years. It is a fastidious organism that is notoriously difficult to culture on standard solid media, making PCR or inoculation into liquid blood culture vials the diagnostic methods of choice.
None
Previous ChapterOrthopedic & Rheumatology Board Review: JIA, Bone Tumors, S…
Next Chapter ABOS Orthopedic Board Review: Psoriatic Arthritis, Lipoma A…

Medically Verified Content by
Prof. Dr. Mohammed Hutaif Clinic
Consultant Orthopedic & Spine Surgeon