ABOS Orthopedic Board Review: Psoriatic Arthritis, Lipoma Arborescens, Down Syndrome, Scoliosis | Part 30

Key Takeaway
This ABOS Orthopedic Board Review provides challenging multiple-choice questions on key topics. Master your knowledge of psoriatic arthritis, lipoma arborescens, Down syndrome orthopedic abnormalities, and various scoliosis types. Enhance your exam preparation with detailed rationales and explanations for comprehensive understanding.
Question 1
A 60-year-old male with long-standing psoriatic arthritis presents with severe pain and deformity in his right hand. Radiographs of the hand reveal significant erosive changes, particularly in the interphalangeal joints, with a characteristic "pencil-in-cup" appearance in the right 4th DIP joint. This radiographic finding is pathognomonic for:
View Answer & Explanation
Correct Answer: D
Rationale: The "pencil-in-cup" deformity, characterized by resorption of the distal phalanx creating a pointed, "pencil" appearance that fits into an eroded, "cup-shaped" proximal phalanx, is a classic and highly specific radiographic finding for psoriatic arthritis, particularly in the DIP joints. It represents severe erosive changes. Main Distractor Rationale: Rheumatoid arthritis (A) causes erosions but typically spares DIP joints and does not produce this specific deformity. Osteoarthritis (B) is characterized by joint space narrowing, osteophytes, and subchondral sclerosis, not erosions or "pencil-in-cup." Gout (C) can cause erosions with overhanging edges but not the "pencil-in-cup" appearance. Ankylosing spondylitis (E) primarily affects the axial skeleton and entheses, not typically causing this type of peripheral joint destruction.
Question 2
A 48-year-old female presents with symmetric polyarthritis affecting her MCP and PIP joints, morning stiffness lasting over an hour, and fatigue. She has a positive rheumatoid factor (RF) and anti-CCP antibody. However, she also has a history of psoriasis. Which of the following features would most strongly suggest psoriatic arthritis over rheumatoid arthritis in this patient, despite the overlapping symptoms?
View Answer & Explanation
Correct Answer: C
Rationale: While psoriatic arthritis can mimic rheumatoid arthritis with symmetric polyarthritis, morning stiffness, and elevated inflammatory markers, and even rarely positive RF/anti-CCP, the presence of dactylitis (sausage digits) is a highly characteristic and specific feature of psoriatic arthritis that is not typically seen in rheumatoid arthritis. This would be a strong indicator to differentiate between the two conditions in a patient with psoriasis. Main Distractor Rationale: Symmetric joint involvement (A), elevated ESR and CRP (B), and morning stiffness > 60 minutes (D) are common features of both rheumatoid arthritis and polyarticular psoriatic arthritis, making them less useful for differentiation. Positive RF and anti-CCP antibodies (E) are hallmarks of rheumatoid arthritis, and while they can be positive in a small percentage of PsA patients, their presence generally points towards RA. Therefore, dactylitis is the most distinguishing feature among the options provided.
Question 3
A 55-year-old male with psoriatic arthritis reports recent onset of eye redness, pain, and photophobia. Ophthalmic examination reveals anterior uveitis. This extra-articular manifestation is most commonly associated with which subtype of psoriatic arthritis?
Correct Answer: E
Question 4
A 40-year-old male is diagnosed with psoriatic arthritis affecting his right knee and left ankle, with mild skin involvement. He has failed a trial of NSAIDs. His rheumatologist recommends initiating a disease-modifying anti-rheumatic drug (DMARD). Which of the following is generally considered the first-line conventional synthetic DMARD for peripheral psoriatic arthritis?
View Answer & Explanation
Correct Answer: B
Rationale: Methotrexate is widely considered the first-line conventional synthetic DMARD for patients with active peripheral psoriatic arthritis who have failed NSAIDs, especially when there is also significant skin involvement. It is effective for both joint and skin manifestations. Main Distractor Rationale: Adalimumab (A) is a biologic (TNF inhibitor) and is typically used after failure of conventional DMARDs or in severe cases. Prednisone (C) is a corticosteroid used for acute flares but not as a long-term DMARD due to side effects. Hydroxychloroquine (D) is less effective for psoriatic arthritis and can sometimes exacerbate psoriasis. Cyclosporine (E) is a potent immunosuppressant, effective for severe psoriasis and PsA, but typically reserved for cases refractory to methotrexate due to its toxicity profile.
Question 5
A 50-year-old male with psoriatic arthritis primarily presents with inflammatory back pain, morning stiffness, and limited spinal mobility. Radiographs show sacroiliitis and syndesmophytes in the lumbar spine. He has failed NSAID therapy. Which class of medication is generally considered the most effective first-line biologic therapy for axial psoriatic arthritis?
View Answer & Explanation
Correct Answer: C
Rationale: TNF-alpha inhibitors (e.g., etanercept, infliximab, adalimumab, golimumab, certolizumab pegol) are considered the first-line biologic therapy for axial psoriatic arthritis (spondylitis and sacroiliitis) that has not responded to NSAIDs. They have demonstrated significant efficacy in reducing inflammation, pain, and improving spinal mobility. Main Distractor Rationale: IL-17 inhibitors (B) and IL-12/23 inhibitors (D) are also effective for psoriatic arthritis, including axial disease, but TNF-alpha inhibitors have a longer track record and are often considered first-line for axial involvement. JAK inhibitors (A) are oral targeted synthetic DMARDs that are also effective but typically used after failure of biologics or in specific circumstances. T-cell costimulation blockers (E), like abatacept, are generally not indicated for axial spondyloarthritis.
Question 6
A 42-year-old female with severe psoriatic arthritis and extensive skin psoriasis is being considered for biologic therapy. Her rheumatologist suggests an agent that targets a key pro-inflammatory cytokine involved in both joint inflammation and skin pathology. Which of the following cytokines is a primary target for drugs like etanercept, infliximab, and adalimumab?
View Answer & Explanation
Correct Answer: C
Rationale: Etanercept, infliximab, and adalimumab are all Tumor Necrosis Factor-alpha (TNF-alpha) inhibitors. TNF-alpha is a crucial pro-inflammatory cytokine that plays a central role in the pathogenesis of both psoriasis and psoriatic arthritis, driving inflammation in the skin and joints. Main Distractor Rationale: Interleukin-17 (D) and Interleukin-23 (E) are also important cytokines in psoriatic disease and are targeted by other classes of biologics (e.g., secukinumab, ustekinumab), but not by the specific drugs listed in the question. Interleukin-1 (A) and Interleukin-6 (B) are pro-inflammatory cytokines, but their inhibitors are primarily used in other rheumatic conditions like rheumatoid arthritis (e.g., tocilizumab for IL-6) and are not the primary targets for the listed drugs in psoriatic arthritis.
Question 7
A 35-year-old male with active psoriatic arthritis and moderate-to-severe plaque psoriasis has not responded adequately to methotrexate and a TNF-alpha inhibitor. His physician is considering a different class of biologic. Which of the following biologics specifically targets the IL-17 pathway?
View Answer & Explanation
Correct Answer: C
Rationale: Secukinumab is an interleukin-17A (IL-17A) inhibitor. IL-17 is a key cytokine in the inflammatory cascade of psoriasis and psoriatic arthritis, and its inhibition has proven effective in patients who fail other therapies, including TNF-alpha inhibitors. Main Distractor Rationale: Rituximab (A) targets CD20 on B cells and is used in rheumatoid arthritis and vasculitis. Abatacept (B) is a T-cell costimulation blocker used in rheumatoid arthritis. Tocilizumab (D) is an IL-6 receptor blocker used in rheumatoid arthritis. Ustekinumab (E) targets the p40 subunit common to IL-12 and IL-23, not IL-17 directly.
Question 8
A 55-year-old male presents with a 10-year history of intermittent right knee swelling and occasional pain flares. He reports feeling a "squishy" sensation in the knee. Physical examination reveals a moderate knee effusion and mild tenderness along the joint line. Radiographs are unremarkable except for a mild effusion. An MRI is ordered.
View Answer & Explanation
Correct Answer: C
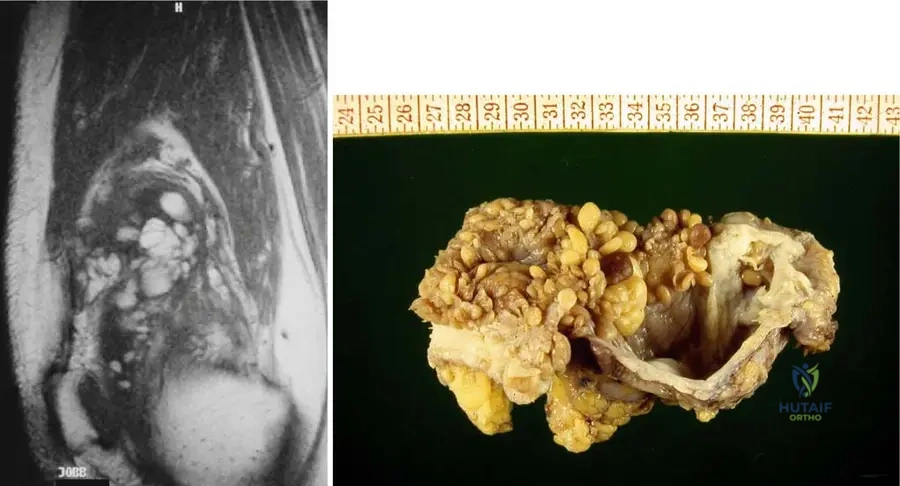
Rationale: Lipoma arborescens is characterized on MRI by nodular masses within the joint that have signal intensity isointense with fat on all pulse sequences, typically associated with a large joint effusion. This is the pathognomonic imaging finding. Option A describes pigmented villonodular synovitis (PVNS). Option B describes synovial chondromatosis. Option D describes inflammatory synovitis. Option E describes a giant cell tumor of the tendon sheath, which is usually extra-articular or localized within the joint, but not typically diffuse fatty infiltration.
Question 9
A 62-year-old female presents with chronic, recurrent left knee effusions over the past 15 years. She denies any specific trauma but reports occasional dull pain. Physical examination shows a palpable effusion and mild crepitus. Plain radiographs are unremarkable. Given the chronicity and nonspecific symptoms, what is the most likely underlying pathology?
View Answer & Explanation
Correct Answer: D
Rationale: Lipoma arborescens is an extremely rare articular disease characterized by fatty infiltration of the synovial lining, typically presenting with recurrent effusions and occasional pain flares over many years, often decades. Radiographs are often unremarkable. This clinical picture strongly aligns with lipoma arborescens. PVNS typically presents with hemosiderin deposition and often bloody effusions. Synovial chondromatosis involves cartilaginous loose bodies. Rheumatoid arthritis would have systemic symptoms and specific serological markers. Gout would present with acute, severe inflammatory flares.
Question 10
A 48-year-old male undergoes arthroscopic synovectomy for chronic knee pain and recurrent effusions. During the procedure, the surgeon notes a diffuse proliferation of yellowish, frond-like tissue within the joint. A biopsy is sent for histopathological examination. What is the expected microscopic finding?
View Answer & Explanation
Correct Answer: B
Rationale: Lipoma arborescens is characterized microscopically by normal synovium interspersed with mature adipocytes. The gross description of "frond-like tissue" is also characteristic. Option A describes PVNS. Option C describes synovial chondromatosis. Option D could be seen in various granulomatous conditions, but not lipoma arborescens. Option E describes features of inflammatory arthritis like rheumatoid arthritis.
Question 11
A 70-year-old male presents with a 20-year history of progressive right knee swelling and stiffness. He reports no acute injury. Physical examination reveals a large, boggy effusion and limited range of motion. Plain radiographs show mild degenerative changes but no specific intra-articular pathology. An MRI is performed to further evaluate the chronic effusion.
View Answer & Explanation
Correct Answer: C
Rationale: Given the chronic, non-traumatic presentation with recurrent effusions and unremarkable radiographs, lipoma arborescens is highly suspected. The characteristic MRI finding for lipoma arborescens is nodular masses within the joint demonstrating signal intensity isointense with fat on all pulse sequences, often with an associated large joint effusion. The provided image (Fig. 10.4a) is a T1-weighted MRI showing this characteristic fatty signal. Option A describes PVNS. Option B describes synovial chondromatosis. Option D describes advanced osteoarthritis or inflammatory arthritis. Option E describes a Baker's cyst, which can be associated but is not the primary pathology.
Question 12
Which of the following joints is most commonly affected by Lipoma Arborescens?
View Answer & Explanation
Correct Answer: D
Rationale: The teaching case explicitly states that "The knee is the most commonly involved joint" for lipoma arborescens. While other joints can be affected, the knee is overwhelmingly the most frequent site.
Question 13
A 58-year-old male presents with a 5-year history of intermittent right knee swelling and mild discomfort. He has no history of trauma or systemic illness. Physical examination reveals a moderate effusion. Initial radiographs are normal. An MRI confirms the presence of intra-articular fatty synovial proliferation. What is the typical laterality of lipoma arborescens?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case states: "Lesions are usually unilateral, but bilateral cases have been reported in the literature." This makes option C the most accurate description of the typical laterality.
Question 14
A 65-year-old female presents with chronic, insidious onset of left knee pain and swelling over several years. She reports no mechanical symptoms or locking. Physical examination reveals a large, soft effusion. Plain radiographs show only mild age-related degenerative changes. What is the primary characteristic of the synovial lining in lipoma arborescens?
View Answer & Explanation
Correct Answer: C
Rationale: Lipoma arborescens is defined as an "extremely rare articular disease where there is fatty infiltration of a joint’s synovial lining." This is the fundamental pathological characteristic. Other options describe different synovial pathologies (PVNS, synovial chondromatosis, giant cell tumor, inflammatory arthritis).
Question 15
A 50-year-old male presents with a 12-year history of recurrent right knee effusions and occasional mild pain. He has undergone multiple aspirations, which yielded clear, straw-colored fluid. Radiographs are unremarkable. An MRI is performed, showing nodular intra-articular masses with fat signal. What is the typical duration of symptoms reported by patients with lipoma arborescens?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case states: "Patients usually report joint difficulties over a number of years, often decades." This highlights the chronic nature of the disease, distinguishing it from acute or subacute conditions.
Question 16
A 60-year-old female presents with chronic left knee swelling. Physical examination reveals a large effusion. Plain radiographs are unremarkable. An MRI is performed, showing intra-articular frond-like masses with fat signal intensity. What is the most common radiographic finding in patients with lipoma arborescens?
View Answer & Explanation
Correct Answer: D
Rationale: The teaching case states: "Radiographs are often unremarkable, although swelling, effusions, and secondary degenerative changes may be present." This indicates that plain radiographs are typically not diagnostic and often appear normal, aside from signs of effusion or secondary changes. Option A describes synovial chondromatosis. Options B and C describe features of inflammatory arthritis or advanced osteoarthritis. Option E is not typical for lipoma arborescens.
Question 17
A 52-year-old male presents with a long history of intermittent right knee swelling and discomfort. An MRI reveals nodular masses within the joint with signal intensity isointense with fat on all pulse sequences, along with a large joint effusion. During subsequent arthroscopy, the surgeon observes the characteristic gross appearance of the synovial tissue. Which of the following best describes this appearance?
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case states: "Grossly, lesions have fronds of fat." The provided image (Fig. 10.4b) also depicts this frond-like appearance of fatty villi. Option A describes PVNS. Option B describes synovial chondromatosis. Option D describes general inflammatory synovitis. Option E describes a localized tumor, not the diffuse nature of lipoma arborescens.
Question 18
A 68-year-old female presents with chronic left knee pain and recurrent effusions. An MRI confirms the diagnosis of lipoma arborescens. What is the most appropriate initial management strategy for symptomatic lipoma arborescens?
View Answer & Explanation
Correct Answer: C
Rationale: While not explicitly detailed in the provided text, the standard treatment for symptomatic lipoma arborescens, especially with recurrent effusions and pain, is arthroscopic synovectomy to remove the hypertrophied fatty synovium. This is a common understanding in orthopaedic practice. Close observation with NSAIDs (E) might be considered for very mild, asymptomatic cases, but for chronic, symptomatic disease, surgical removal is typically indicated. Systemic corticosteroids (A) are not a primary treatment for this benign mechanical issue. Hyaluronic acid injections (B) are for osteoarthritis. Radiation therapy (D) is not indicated for a benign fatty lesion.
Question 19
A 59-year-old male presents with a 10-year history of intermittent right knee swelling and mild discomfort. Physical examination reveals a moderate effusion. Plain radiographs are unremarkable. An MRI is performed, showing nodular masses within the joint with signal intensity isointense with fat on all pulse sequences. Which of the following conditions is most important to differentiate from lipoma arborescens on MRI due to similar fat signal characteristics?
View Answer & Explanation
Correct Answer: D
Rationale: While lipoma arborescens involves diffuse fatty infiltration of the synovium, an intra-articular lipoma is a distinct, usually solitary, encapsulated benign fatty tumor within the joint. Both will show fat signal on MRI, but lipoma arborescens is diffuse and frond-like, whereas an intra-articular lipoma is typically a well-defined mass. PVNS (A) shows hemosiderin. Synovial hemangioma (B) shows vascular characteristics. Synovial chondromatosis (C) shows cartilaginous loose bodies. Rheumatoid arthritis (E) shows inflammatory pannus.
Question 20
A 63-year-old female presents with chronic left knee pain and swelling. An MRI is performed, revealing nodular masses within the joint demonstrating signal intensity isointense with fat on all pulse sequences, along with a large joint effusion. What is the primary reason for the recurrent effusions seen in lipoma arborescens?
View Answer & Explanation
Correct Answer: B
Rationale: The recurrent effusions in lipoma arborescens are primarily due to the mechanical irritation caused by the hypertrophied, fatty synovial fronds within the joint, leading to a reactive increase in synovial fluid. While some low-grade inflammation might be present, it's not the primary driver. Hemorrhage (C) is more characteristic of PVNS. Adipocytes (D) do not primarily produce synovial fluid. Cartilage breakdown (E) is a secondary effect, not the primary cause of effusion in LA.
Question 21
A 72-year-old male presents with a long-standing history of right knee swelling and occasional pain. He reports no specific trauma. Physical examination reveals a large, boggy effusion. Plain radiographs show mild degenerative changes. An MRI confirms the diagnosis of lipoma arborescens. What is the long-term prognosis for the joint if left untreated?
View Answer & Explanation
Correct Answer: D
Rationale: Lipoma arborescens is a benign condition with no reported malignant transformation (A). If left untreated, the mechanical irritation from the fatty synovial proliferation will likely lead to persistent recurrent effusions and can contribute to secondary degenerative changes (B is too strong, but D captures the essence). It does not spontaneously resolve (C) and is not associated with systemic inflammatory disease (E).
Question 22
A 45-year-old female presents with chronic, intermittent left knee swelling and mild pain for 8 years. She denies any trauma. Physical examination reveals a moderate effusion. Plain radiographs are unremarkable. An MRI is performed, showing nodular masses within the joint with signal intensity isointense with fat on all pulse sequences. Which of the following is NOT a typical clinical complaint or exam finding for lipoma arborescens?
View Answer & Explanation
Correct Answer: E
Rationale: The teaching case states that patients present with "nonspecific complaints and exam findings," "recurrent effusions and occasional pain flares are common," and "joint difficulties over a number of years, often decades." Acute, severe, monoarticular inflammatory arthritis (E) is characteristic of conditions like septic arthritis or gout, not the chronic, insidious nature of lipoma arborescens.
Question 23
A 60-year-old male presents with a 15-year history of right knee swelling and occasional discomfort. An MRI is performed, showing intra-articular nodular masses with fat signal. What is the most accurate description of the underlying pathology of lipoma arborescens?
View Answer & Explanation
Correct Answer: C
Rationale: Lipoma arborescens is defined as "fatty infiltration of a joint’s synovial lining." It is not considered a true neoplasm (A) but rather a reactive or degenerative process. While it causes symptoms, it's not primarily an inflammatory (B) or autoimmune (E) condition, nor is it synovial metaplasia (D) in the sense of cartilage formation.
Question 24
A 55-year-old female presents with chronic left knee swelling and a feeling of "fullness." She has no history of trauma. Physical examination reveals a large, soft effusion. Plain radiographs are unremarkable. An MRI is performed, showing nodular masses within the joint with signal intensity isointense with fat on all pulse sequences. Which of the following MRI sequences would be most helpful in confirming the fatty nature of the synovial proliferation?
View Answer & Explanation
Correct Answer: A
Rationale: While lipoma arborescens shows signal intensity isointense with fat on all pulse sequences (B, C, D), the most definitive way to confirm the fatty nature and differentiate it from other pathologies is to observe signal suppression on fat-saturated sequences (A, E). If the signal drops significantly on T2-weighted fat-suppressed or STIR sequences, it confirms the presence of fat. T2-weighted with fat suppression is a very common and effective sequence for this purpose. STIR (E) is also a fat-suppression technique, but T2-weighted fat suppression is often used in conjunction with T1-weighted to characterize lesions.
Question 25
A 67-year-old male presents with a 20-year history of intermittent right knee swelling and mild pain. He has no history of trauma. Physical examination reveals a moderate effusion. Plain radiographs show early degenerative changes. An MRI is performed, showing nodular masses within the joint with signal intensity isointense with fat on all pulse sequences. What is the primary differential diagnosis for diffuse synovial proliferation with recurrent effusions, but *without* fat signal on MRI?
View Answer & Explanation
Correct Answer: A
Rationale: Pigmented Villonodular Synovitis (PVNS) is a common differential for diffuse synovial proliferation and recurrent effusions. However, unlike lipoma arborescens, PVNS typically shows low signal intensity on T1 and T2 sequences due to hemosiderin deposition, rather than fat signal. Synovial chondromatosis (B) involves cartilaginous loose bodies. Gouty arthritis (C) and septic arthritis (D) are acute inflammatory conditions. Osteoarthritis (E) is a degenerative condition, which can cause effusions and synovial thickening, but not typically diffuse synovial proliferation of this nature without other clear degenerative findings.
Question 26
A 50-year-old male presents with a 7-year history of left knee swelling and occasional pain. He reports no specific injury. Physical examination reveals a moderate effusion. Plain radiographs are unremarkable. An MRI is performed, showing nodular masses within the joint with signal intensity isointense with fat on all pulse sequences. What is the most appropriate next step in confirming the diagnosis and providing definitive treatment?
View Answer & Explanation
Correct Answer: C
Rationale: Given the characteristic MRI findings highly suggestive of lipoma arborescens and the patient's symptomatic presentation (swelling, pain), diagnostic arthroscopy with synovectomy is the most appropriate next step. This allows for direct visualization and biopsy to confirm the diagnosis and simultaneously provides definitive treatment by removing the hypertrophied synovial tissue. Aspiration (A) would likely yield non-specific fluid. Corticosteroid injection (B) might offer temporary relief but doesn't address the underlying mechanical issue. Repeating MRI (D) delays definitive management. Physical therapy (E) is unlikely to resolve the underlying pathology.
Question 27
A 61-year-old female presents with chronic right knee pain and swelling. An MRI reveals nodular masses within the joint demonstrating signal intensity isointense with fat on all pulse sequences, associated with a large joint effusion. The patient asks about the nature of this condition. How would you best describe lipoma arborescens to the patient?
View Answer & Explanation
Correct Answer: C
Rationale: Lipoma arborescens is explicitly described as an "extremely rare articular disease where there is fatty infiltration of a joint’s synovial lining." It is benign and does not become cancerous (A). It is not primarily an inflammatory condition (B) or an infection (E). While it can lead to secondary degenerative changes, it is not primarily caused by cartilage breakdown (D). Option C accurately and concisely describes the condition's benign nature and pathology.
Question 28
A 45-year-old male presents with a 10-year history of intermittent knee pain and swelling. Physical examination reveals a large knee effusion. Radiographs are unremarkable except for the effusion. An MRI of the knee shows nodular masses within the joint that are isointense with fat on all pulse sequences, along with a large joint effusion. Which of the following is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Lipoma arborescens is characterized by fatty infiltration of the synovial lining, presenting on MRI with nodular masses within the joint that have signal intensity isointense with fat on all pulse sequences, typically with an associated large joint effusion. PVNS would show hemosiderin deposition, appearing low signal on T1 and T2. Synovial chondromatosis would show cartilaginous loose bodies. Rheumatoid arthritis and septic arthritis would have different MRI characteristics and clinical presentations.
Question 29
A 62-year-old female reports a 20-year history of recurrent knee effusions and occasional pain flares in her right knee. Radiographs show mild degenerative changes. MRI reveals frond-like fatty villi within the suprapatellar pouch, consistent with fatty infiltration of the synovium. What is the typical duration of symptoms reported by patients with this condition?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical context states that patients with lipoma arborescens usually report joint difficulties over a number of years, often decades, due to its slow-growing and benign nature. The other options represent much shorter durations not typical for this chronic condition.
Question 30
A 55-year-old male undergoes arthroscopic synovectomy for chronic knee effusions. During the procedure, the surgeon observes a characteristic appearance of the synovial lining. Which of the following gross findings is most consistent with lipoma arborescens?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that grossly, lesions of lipoma arborescens have "fronds of fat." This is a pathognomonic gross finding. Diffuse reddish-brown discoloration is seen in PVNS, and loose cartilaginous bodies are characteristic of synovial chondromatosis.
Question 31
A biopsy is taken from the knee synovium of a 48-year-old patient presenting with chronic knee swelling and MRI findings suggestive of lipoma arborescens. Microscopic examination of the specimen is performed. Which of the following histological features is expected?
View Answer & Explanation
Correct Answer: B
Rationale: Microscopically, lipoma arborescens is characterized by normal synovium interspersed with mature adipocytes, reflecting the fatty infiltration. Proliferation of synovial cells with hemosiderin is seen in PVNS. Chondrocytes in a cartilaginous matrix are characteristic of synovial chondromatosis.
Question 32
A 38-year-old male presents with chronic, recurrent effusions in his left knee. MRI confirms the presence of nodular fatty masses within the joint. Based on the typical presentation of lipoma arborescens, which joint is most commonly involved?
View Answer & Explanation
Correct Answer: E
Rationale: The text explicitly states that "The knee is the most commonly involved joint" for lipoma arborescens. While other joints can be affected, the knee is the predominant site.
Question 33
A 50-year-old patient is diagnosed with lipoma arborescens in the right knee after presenting with long-standing effusions. The patient inquires about the likelihood of developing the same condition in the contralateral knee. What is the typical laterality of lipoma arborescens?
View Answer & Explanation
Correct Answer: B
Rationale: The text states that lesions are "usually unilateral, but bilateral cases have been reported in the literature." This indicates that while it's predominantly unilateral, bilateral involvement is a known, albeit less common, possibility.
Question 34
A 42-year-old female presents with a 15-year history of intermittent right knee swelling and discomfort. Initial plain radiographs of the knee are obtained. What are the typical findings on radiographs for lipoma arborescens?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that "Radiographs are often unremarkable, although swelling, effusions, and secondary degenerative changes may be present." This highlights the non-specific nature of plain film findings for this condition.
Question 35
A 60-year-old male presents with chronic knee pain and swelling. MRI demonstrates nodular masses within the joint with signal intensity identical to subcutaneous fat. This finding is characteristic of what type of synovial infiltration?
View Answer & Explanation
Correct Answer: C
Rationale: Lipoma arborescens is defined as a fatty infiltration of a joint's synovial lining. The MRI description of signal intensity isointense with fat directly points to fatty infiltration. Hemosiderin is seen in PVNS, and cartilaginous metaplasia in synovial chondromatosis.
Question 36
A 58-year-old patient is diagnosed with lipoma arborescens. This condition primarily affects which specific anatomical structure within the joint?
View Answer & Explanation
Correct Answer: C
Rationale: The definition of lipoma arborescens is "an extremely rare articular disease where there is fatty infiltration of a joint’s synovial lining." Therefore, the synovial lining is the primary structure affected.
Question 37
A 47-year-old patient presents with a long history of knee effusions and occasional pain. The clinical presentation is described as "nonspecific complaints and exam findings." Given this description, which of the following best characterizes the typical clinical course of lipoma arborescens?
View Answer & Explanation
Correct Answer: C
Rationale: The text describes the clinical presentation as "nonspecific complaints and exam findings. Recurrent effusions and occasional pain flares are common. Patients usually report joint difficulties over a number of years, often decades." This points to a chronic, insidious course with recurrent effusions and mild pain flares.
Question 38
A 52-year-old female undergoes an MRI for chronic knee swelling. The report notes nodular masses within the joint that demonstrate signal intensity identical to subcutaneous fat on T1-weighted, T2-weighted, and fat-suppressed sequences. This specific MRI characteristic is crucial for diagnosing lipoma arborescens. What is the key signal intensity finding on all pulse sequences?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that MRI demonstrates characteristic imaging features with "nodular masses within the joint that have signal intensity isointense with fat on all pulse sequences." This is the defining MRI characteristic for lipoma arborescens.
Question 39
A 65-year-old male presents with a long history of knee discomfort and swelling. MRI findings are highly suggestive of lipoma arborescens. In addition to the characteristic synovial changes, what other finding is typically associated with this condition on MRI?
View Answer & Explanation
Correct Answer: D
Rationale: The text states, "There is usually an associated large joint effusion" with the characteristic MRI findings of lipoma arborescens. While other findings might be present incidentally, a large joint effusion is a commonly associated feature.
Question 40
A gross specimen is obtained during synovectomy for a patient with lipoma arborescens. The specimen is described as having a distinctive appearance. Which term best describes the characteristic macroscopic morphology of lipoma arborescens?
View Answer & Explanation
Correct Answer: C
Rationale: The text and accompanying image description explicitly state, "Grossly, lesions have fronds of fat" and "Note the frond-like appearance of the fatty villi." This is a key descriptive feature of the gross specimen.
Question 41
A 40-year-old patient presents with chronic knee effusions. After extensive workup, including MRI and biopsy, a diagnosis of lipoma arborescens is made. Considering the prevalence of this condition, how would it be classified?
View Answer & Explanation
Correct Answer: C
Rationale: The very first sentence of the text states, "Lipoma arborescens is an extremely rare articular disease." This emphasizes its low incidence.
Question 42
A 50-year-old patient with a 10-year history of knee problems is suspected of having lipoma arborescens. Clinically, what are the most common complaints reported by patients with this condition?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Clinically, patients present with nonspecific complaints and exam findings. Recurrent effusions and occasional pain flares are common." This accurately describes the typical clinical presentation.
Question 43
A 68-year-old male is diagnosed with lipoma arborescens in his knee. Given the name "lipoma," what is the general biological nature of this lesion?
View Answer & Explanation
Correct Answer: C
Rationale: The term "lipoma" generally refers to a benign tumor composed of mature fat cells. Lipoma arborescens is a benign fatty infiltration of the synovium, not a malignant, precancerous, infectious, or autoimmune process.
Question 44
A 44-year-old patient presents with chronic knee swelling. An MRI is performed. The presence of nodular masses within the joint with signal intensity isointense with fat on all pulse sequences, including fat-suppressed images, helps differentiate lipoma arborescens from other synovial proliferative disorders. Which of the following conditions would typically show low signal intensity on T1 and T2 due to hemosiderin?
View Answer & Explanation
Correct Answer: B
Rationale: Pigmented Villonodular Synovitis (PVNS) is characterized by hemosiderin deposition, which typically appears as low signal intensity on both T1- and T2-weighted MRI sequences, often with "blooming" on gradient echo sequences. This contrasts sharply with the fat-isointense signal of lipoma arborescens.
Question 45
A 59-year-old patient presents with a long history of knee effusions. An MRI is performed, and the T1-weighted image (Fig. 10.4a) shows characteristic findings. What specific feature is highlighted in the description of the T1-weighted MRI image for lipoma arborescens?
View Answer & Explanation
Correct Answer: C
Rationale: The image caption for Fig. 10.4a explicitly states, "Note the frond-like appearance of the fatty villi corresponding to the areas of fat signal on MRI." This directly refers to the characteristic fat signal on the T1-weighted image.
Question 46
A 46-year-old patient presents with chronic, unexplained knee swelling. After a thorough evaluation, including advanced imaging, a diagnosis of lipoma arborescens is made. This condition is best described as a:
View Answer & Explanation
Correct Answer: C
Rationale: Lipoma arborescens is characterized by fatty infiltration of the synovial lining, which is a form of synovial proliferation. It is not primarily a bone tumor, cartilage disorder, ligamentous issue, or inflammatory arthropathy in the typical sense.
Question 47
A 3-year-old male presents for a routine orthopedic check-up. He was diagnosed with Down syndrome at birth. His parents are concerned about his overall development and potential associated medical conditions. What is the most frequent chromosomal anomaly associated with Down syndrome?
View Answer & Explanation
Correct Answer: C
Rationale: Down syndrome is explicitly stated as the most frequent chromosomal anomaly, trisomy 21. Trisomy 18 (Edwards syndrome) and Monosomy X (Turner syndrome) are other chromosomal anomalies but not the cause of Down syndrome. Klinefelter syndrome is XXY.
Question 48
A 6-month-old infant with a known diagnosis of Down syndrome is referred to orthopedics for evaluation of generalized hypotonia. The orthopedic surgeon is aware that while orthopedic issues are common, another medical condition historically represented the primary cause of morbidity and mortality in these patients. What is the most common cause of morbidity in individuals with Down syndrome?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "Although congenital heart disease (most commonly atrioventricular canal defect) is the main cause of morbidity in mongolism..." While atlanto-axial instability and recurrent hip luxations are significant orthopedic problems, they are not the primary cause of morbidity. Leukemia and gastrointestinal malformations are not mentioned as the main cause of morbidity in the provided text.
Question 49
A 4-year-old boy with Down syndrome presents with a history of recurrent patellar dislocations. On physical examination, he demonstrates excessive joint mobility in multiple joints. The underlying etiology for the majority of orthopedic problems observed in patients with Down syndrome is most likely:
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "The most probable origin of these problems is generalized ligamentous laxity which occurs in almost every Down syndrome patient." While some patients might have other contributing factors, generalized ligamentous laxity is identified as the primary underlying cause for the listed orthopedic issues.
Question 50
A 7-year-old girl with Down syndrome is brought to the clinic due to a noticeable limp and difficulty walking. Her parents report a history of recurrent hip dislocations since she started walking. Physical examination reveals a significant leg length discrepancy. Radiographs confirm a fixed hip dislocation. This presentation is consistent with a common orthopedic complication in Down syndrome patients.
View Answer & Explanation
Correct Answer: C
Rationale: The text and image caption (Fig. 1.108) directly state, "Recurrent hip luxations may result fixed dislocation in untreated cases, like this patient with the prominent leg length discrepancy." This perfectly matches the vignette. While developmental dysplasia of the hip can occur, the specific progression from recurrent luxations to fixed dislocation with leg length discrepancy is highlighted as a characteristic outcome in Down syndrome.
Question 51
A 5-year-old boy with Down syndrome presents with a history of his kneecap "popping out" frequently, especially during sports activities. On examination, the patella is easily dislocated laterally with minimal provocation. This condition is a common orthopedic problem in patients with Down syndrome, primarily due to generalized ligamentous laxity.
View Answer & Explanation
Correct Answer: C
Rationale: The text lists "habitual luxation of the patella" as one of the significant orthopedic problems associated with Down syndrome, stemming from generalized ligamentous laxity. Osgood-Schlatter disease, patellofemoral pain syndrome, tibial tubercle avulsion, and osteochondritis dissecans are other knee conditions but do not describe the recurrent dislocation seen in this patient with Down syndrome.
Question 52
A 9-year-old girl with Down syndrome is undergoing a pre-operative evaluation for an unrelated surgical procedure. As part of her routine orthopedic screening, the surgeon is particularly vigilant for a specific spinal instability that is common in this population and can have serious neurological consequences. Which of the following spinal conditions is frequently associated with Down syndrome?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly lists "atlanto-axial instability" as one of the significant orthopedic abnormalities associated with Down syndrome. The other options are spinal conditions but are not specifically highlighted as common in Down syndrome in the provided text.
Question 53
A 2-year-old boy with Down syndrome is noted by his parents to have very flexible feet and a lack of a normal arch when standing. On examination, his feet appear pronated and flattened. This common foot deformity in Down syndrome is attributed to generalized ligamentous laxity.
View Answer & Explanation
Correct Answer: D
Rationale: The text lists "flatfoot" as one of the orthopedic abnormalities associated with Down syndrome. Clubfoot, metatarsus adductus, pes cavus, and vertical talus are other foot deformities, but flatfoot is specifically mentioned in the context of Down syndrome.
Question 54
A 6-year-old girl with Down syndrome presents with a noticeable "knock-knee" appearance. On physical examination, she has bilateral genu valgum. This angular deformity is a recognized orthopedic problem in patients with Down syndrome, often exacerbated by their generalized ligamentous laxity.
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly lists "genu valgum" as one of the orthopedic abnormalities associated with Down syndrome. Genu varum (bowlegs) is the opposite deformity, and genu recurvatum, tibial torsion, and femoral anteversion are different lower extremity conditions.
Question 55
A 10-year-old boy with Down syndrome is being evaluated for generalized joint hypermobility. The orthopedic resident performs several tests to assess for generalized ligamentous laxity according to the Carter and Wilkinson criteria. To establish a diagnosis of generalized joint laxity using these criteria, how many of the specified tests must be positive?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "According to Carter and Wilkinson the diagnosis of generalized joint laxity can be set if more than two of the following tests are positive." This directly answers the question.
Question 56
A 12-year-old girl with Down syndrome is being assessed for generalized ligamentous laxity. As part of the Carter and Wilkinson criteria, the orthopedic surgeon attempts to passively appose her thumb to the flexor aspect of her forearm. This test is positive if she can achieve this maneuver.
View Answer & Explanation
Correct Answer: B
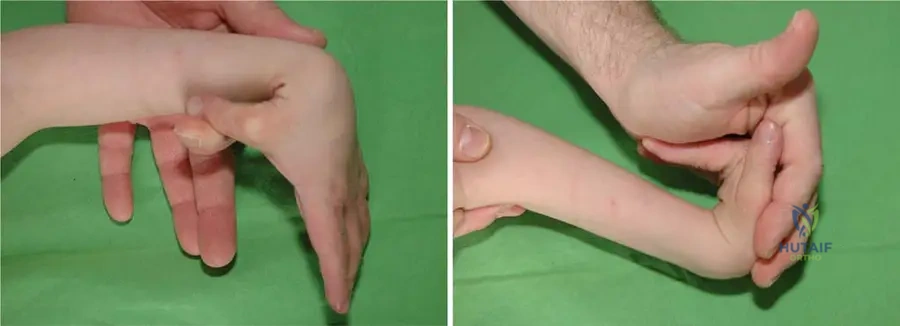
Rationale: The vignette describes one of the specific Carter and Wilkinson tests. Option B directly matches the description: "(1) passive apposition of the thumb to the flexor aspect of the forearm." The image (Fig. 1.105 a, b) illustrates generalized ligamentous laxity, which includes this test.
Question 57
A 3-year-old boy with Down syndrome is evaluated for hypermobility. During the physical examination, the orthopedic surgeon assesses for generalized ligamentous laxity using the Carter and Wilkinson criteria. One of the criteria involves assessing the elbow joint. Which of the following describes a positive finding for elbow laxity?
View Answer & Explanation
Correct Answer: B
Rationale: The text lists "(3) ability to hyperextend the elbow more than 10°" as one of the Carter and Wilkinson tests for generalized joint laxity. The other options describe different elbow findings not related to the specific laxity criteria.
Question 58
A 14-year-old adolescent with Down syndrome is being screened for joint hypermobility. When assessing the knee joint as part of the Carter and Wilkinson criteria, what specific finding indicates a positive test for generalized ligamentous laxity?
View Answer & Explanation
Correct Answer: C
Rationale: The text lists "(4) ability to hyperextend the knee more than 10°" as one of the Carter and Wilkinson tests for generalized joint laxity. The other options describe different knee findings not related to the specific laxity criteria.
Question 59
A 5-year-old child with Down syndrome is undergoing an orthopedic evaluation. The physician performs a test for generalized ligamentous laxity by passively hyperextending the child's fingers. What specific finding, according to Carter and Wilkinson, indicates a positive test for finger laxity?
View Answer & Explanation
Correct Answer: B
Rationale: The text lists "(2) passive hyperextension of the fingers so that they lay parallel with the extensor aspect of the forearm" as one of the Carter and Wilkinson tests for generalized joint laxity. The image (Fig. 1.105 a, b) illustrates generalized ligamentous laxity, which includes this test.
Question 60
A 8-year-old boy with Down syndrome is being assessed for generalized ligamentous laxity. The orthopedic surgeon examines his ankle and foot. According to the Carter and Wilkinson criteria, which of the following findings in the ankle and foot would be considered a positive test for laxity?
View Answer & Explanation
Correct Answer: B
Rationale: The text lists "excessive range of passive dorsiflexion of the ankle and eversion of the foot" as one of the Carter and Wilkinson tests for generalized joint laxity. The other options describe different ankle/foot findings not related to the specific laxity criteria.
Question 61
A 1-year-old infant with Down syndrome is referred to orthopedics. The parents express gratitude for the successful cardiac surgery their child recently underwent for an atrioventricular canal defect. The orthopedic surgeon explains that due to advancements in medical care for Down syndrome patients, the focus on certain aspects of their health has shifted. What is the primary reason for the increased importance of orthopedic problems in Down syndrome patients today?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "effective cardiac surgical techniques decreased the mortality of Down syndrome children and doing so increased the importance of their orthopedic problems." This directly explains the shift in focus.
Question 62
A 7-year-old boy with Down syndrome presents with a combination of orthopedic issues including a noticeable limp, flat feet, and a "knock-knee" appearance. His parents also report that his kneecaps sometimes "pop out." These multiple musculoskeletal findings are all commonly observed in Down syndrome and share a common underlying etiology.
View Answer & Explanation
Correct Answer: C
Rationale: The vignette describes several orthopedic problems (limp from hip/patella, flat feet, genu valgum, patellar luxation) all explicitly listed in the text as associated with Down syndrome. The text attributes the origin of these problems to "generalized ligamentous laxity."
Question 63
A 15-year-old male with Down syndrome is noted to have a progressive spinal curvature. Radiographic evaluation confirms scoliosis. This condition, along with other orthopedic issues like hip dislocation and patellar luxation, is a recognized abnormality in Down syndrome. What is the most common congenital heart defect associated with Down syndrome, as mentioned in the provided text?
View Answer & Explanation
Correct Answer: E
Rationale: The text explicitly states that congenital heart disease is the main cause of morbidity, and specifically mentions "(most commonly atrioventricular canal defect)."
Question 64
A 9-year-old boy with Down syndrome presents with a long-standing history of hip instability. His parents recall multiple instances where his hip seemed to "pop out" and then reduce spontaneously. Over the past year, he has developed a persistent limp and leg length discrepancy. Radiographs confirm a fixed dislocation of the hip. This progression from recurrent luxations to a fixed dislocation is a known complication in Down syndrome.
View Answer & Explanation
Correct Answer: C
Rationale: The text and image caption (Fig. 1.108) state, "Recurrent hip luxations may result fixed dislocation in untreated cases, like this patient with the prominent leg length discrepancy." This directly supports that untreated recurrent luxations lead to fixed dislocation.
Question 65
A 1-year-old infant with Down syndrome is brought for an orthopedic consultation. The parents are educated about the common orthopedic issues their child may face. These issues are largely attributed to a pervasive underlying condition. Which of the following is NOT listed as an orthopedic abnormality associated with Down syndrome in the provided text?
View Answer & Explanation
Correct Answer: C
Rationale: The text lists dislocation of the hip, habitual luxation of the patella, genu valgum, flatfoot, atlanto-axial instability, and scoliosis as orthopedic abnormalities. Clubfoot (talipes equinovarus) is not mentioned in the provided list.
Question 66
A 10-year-old girl with Down syndrome presents with a history of multiple orthopedic complaints, including a waddling gait, frequent knee instability, and a noticeable spinal curve. Her physical examination confirms generalized joint hypermobility. The overall orthopedic presentation in Down syndrome is primarily characterized by a spectrum of conditions stemming from a single common underlying factor.
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "The most probable origin of these problems is generalized ligamentous laxity which occurs in almost every Down syndrome patient." While muscle hypotonia is also present in Down syndrome, the text specifically attributes the *orthopedic problems* listed (dislocation of the hip, habitual luxation of the patella, genu valgum, flatfoot, atlanto-axial instability, scoliosis) to generalized ligamentous laxity.
Question 67
A 3-month-old infant with Down Syndrome is undergoing a cardiac evaluation. The pediatric cardiologist notes a significant murmur and identifies a common congenital heart defect associated with this chromosomal anomaly. Which of the following is the most frequently observed cardiac defect in patients with Down Syndrome?
View Answer & Explanation
Correct Answer: C
Rationale: The provided text explicitly states that congenital heart disease, most commonly an atrioventricular canal defect, is the main cause of morbidity in Down Syndrome. Main Distractor Rationale: While ventricular septal defects (VSDs) and patent ductus arteriosus (PDA) can occur in Down Syndrome, the atrioventricular canal defect is specifically highlighted as the most common and significant cardiac anomaly.
Question 68
A 7-year-old boy with Down Syndrome presents with new-onset gait disturbance, neck pain, and hyperreflexia in his lower extremities. His parents report a recent fall from a low height. Given his underlying condition, which orthopedic problem is most likely responsible for these symptoms?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical vignette describes neurological symptoms (gait disturbance, hyperreflexia) along with neck pain following trauma in a patient with Down Syndrome. The text lists atlanto-axial instability as a significant orthopedic problem in these patients, and such instability can lead to spinal cord compression, manifesting with these symptoms. Main Distractor Rationale: While recurrent patellar luxation, genu valgum, scoliosis, and hip dislocation are common orthopedic issues in Down Syndrome, they do not typically present with acute neurological symptoms related to spinal cord compression in the cervical region.
Question 69
A 10-year-old girl with Down Syndrome is evaluated for increasing difficulty with ambulation and frequent falls. Physical examination reveals a waddling gait and limited hip abduction. Radiographs show bilateral hip subluxation. The underlying generalized condition contributing to this presentation is:
View Answer & Explanation
Correct Answer: CRationale: The text explicitly states that generalized ligamentous laxity occurs in almost every Down Syndrome patient and is the "most probable origin" of orthopedic problems such as dislocation of the hip. This laxity directly contributes to joint instability and subluxation. Main Distractor Rationale: While muscular hypotonia is also characteristic of Down Syndrome and contributes to joint instability, the text specifically identifies generalized ligamentous laxity as the primary orthopedic origin for hip dislocations and other joint problems.
Question 70
A 14-year-old male with Down Syndrome presents with a history of his knee "giving out" and occasional locking. On examination, his patella is easily displaced laterally with minimal effort. This condition is directly attributable to the generalized underlying musculoskeletal characteristic of Down Syndrome. Which of the following is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: The vignette describes symptoms and findings consistent with patellar instability (knee "giving out," lateral patellar displacement). The text lists "habitual luxation of the patella" as a common orthopedic abnormality in Down Syndrome, stemming from generalized ligamentous laxity. Main Distractor Rationale: While other knee pathologies can occur, habitual luxation of the patella is a specific and common problem in Down Syndrome patients due to their inherent ligamentous laxity, making it the most likely diagnosis given the clinical picture.
Question 71
A 5-year-old child with Down Syndrome is brought for evaluation of foot pain and an altered gait pattern. On examination, the child exhibits a pronated foot posture with a collapsed medial longitudinal arch. This common foot deformity in Down Syndrome is known as:
View Answer & Explanation
Correct Answer: C
Rationale: The text lists "flatfoot" as one of the common orthopedic problems associated with Down Syndrome. The description of a pronated foot with a collapsed medial longitudinal arch is characteristic of flatfoot deformity. Main Distractor Rationale: While other foot deformities exist, flatfoot is specifically mentioned in the text as a common issue in Down Syndrome patients, often exacerbated by generalized ligamentous laxity.
Question 72
A 2-year-old with Down Syndrome is being followed by an orthopedic surgeon. The parents inquire about the increasing focus on orthopedic issues in children with Down Syndrome compared to previous generations. What is the primary reason for this shift in clinical importance?
View Answer & Explanation
Correct Answer: D
Rationale: The text states, "effective cardiac surgical techniques decreased the mortality of Down syndrome children and doing so increased the importance of their orthopedic problems." This directly explains the shift in focus. Main Distractor Rationale: While improved diagnostics and awareness are beneficial, the fundamental reason for the increased *importance* of orthopedic problems is the increased lifespan of these children, allowing them to live long enough for these issues to become clinically significant.
Question 73
A 6-year-old boy with Down Syndrome is evaluated for generalized joint hypermobility. To assess for generalized joint laxity according to Carter and Wilkinson criteria, which of the following tests would be considered positive if the elbow extends beyond 10 degrees?
View Answer & Explanation
Correct Answer: C
Rationale: The question specifically asks which test is positive if the elbow extends beyond 10 degrees. The text lists "ability to hyperextend the elbow more than 10°" as one of the Carter and Wilkinson criteria for generalized joint laxity. Main Distractor Rationale: All options A, B, D, and E are also Carter and Wilkinson criteria, but option C is the only one that directly corresponds to the specific finding mentioned in the vignette (elbow hyperextension > 10 degrees).
Question 74
A 12-year-old girl with Down Syndrome presents with a noticeable limp and a discrepancy in leg length. Her medical history includes untreated recurrent hip luxations since early childhood. Which of the following is the most likely long-term consequence of these untreated recurrent hip luxations, as depicted in the clinical context?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "Recurrent hip luxations may result fixed dislocation in untreated cases, like this patient with the prominent leg length discrepancy." The image caption also reinforces this. Main Distractor Rationale: While avascular necrosis and early osteoarthritis can be complications of hip pathology, the text specifically highlights fixed dislocation and leg length discrepancy as the direct result of untreated recurrent luxations in Down Syndrome patients.
Question 75
A 4-year-old boy with Down Syndrome is noted to have a positive Galeazzi sign on the right side during a routine orthopedic check-up. This finding suggests a potential issue with hip stability. The primary underlying factor contributing to hip instability in children with Down Syndrome is:
View Answer & Explanation
Correct Answer: C
Rationale: The text clearly states that "generalized ligamentous laxity which occurs in almost every Down syndrome patient" is the "most probable origin" of orthopedic problems such as dislocation of the hip. Main Distractor Rationale: While muscular weakness (hypotonia) is also present in Down Syndrome and contributes to instability, the text specifically identifies generalized ligamentous laxity as the primary underlying orthopedic cause for hip dislocations.
Question 76
A 9-year-old girl with Down Syndrome is being assessed for generalized joint hypermobility. As part of the Carter and Wilkinson criteria, the examiner attempts to passively appose the patient's thumb to the flexor aspect of the forearm. A positive result for this test indicates:
View Answer & Explanation
Correct Answer: C
Rationale: The text lists "passive apposition of the thumb to the flexor aspect of the forearm" as one of the specific tests used to diagnose generalized joint laxity according to Carter and Wilkinson. A positive result indicates laxity. Main Distractor Rationale: Normal joint flexibility would not typically allow for this extreme range of motion. Ligamentous contracture, muscular spasticity, or bone deformity would generally *limit* joint motion, not increase it.
Question 77
A 15-year-old patient with Down Syndrome undergoes an assessment for generalized joint laxity using the Carter and Wilkinson criteria. The patient demonstrates passive apposition of the thumb to the forearm, hyperextension of the elbows greater than 10 degrees, and excessive ankle dorsiflexion. Based on these findings, how many positive tests are required to establish a diagnosis of generalized joint laxity?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "According to Carter and Wilkinson the diagnosis of generalized joint laxity can be set if more than two of the following tests are positive." Main Distractor Rationale: While the patient in the vignette has three positive tests, the critical threshold for diagnosis is "more than two," not exactly two or all five.
Question 78
A newborn is diagnosed with Down Syndrome based on characteristic clinical features and genetic testing. The most frequent chromosomal anomaly responsible for this condition is:
View Answer & Explanation
Correct Answer: D
Rationale: The text begins by stating, "The most frequent chromosomal anomaly, trisomy 21 is associated with numerous orthopedic abnormalities." This directly identifies the genetic basis of Down Syndrome. Main Distractor Rationale: Trisomy 18 (Edwards syndrome) and Trisomy 13 (Patau syndrome) are other chromosomal anomalies, but Trisomy 21 is specifically associated with Down Syndrome and is the most frequent chromosomal anomaly mentioned in the context of this condition.
Question 79
A 3-year-old child with Down Syndrome is seen for a routine orthopedic follow-up. The parents express gratitude for the advancements in medical care that have significantly improved their child's life expectancy. This improvement in survival is primarily due to successful management of which of the following?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Although congenital heart disease (most commonly atrioventricular canal defect) is the main cause of morbidity in mongolism, effective cardiac surgical techniques decreased the mortality of Down syndrome children..." This directly links improved survival to cardiac management. Main Distractor Rationale: While other medical issues can affect Down Syndrome patients, the text specifically identifies congenital heart disease as the primary cause of morbidity and the target of interventions that have decreased mortality.
Question 80
A 10-year-old boy with Down Syndrome presents with a history of his right hip "popping out" and then reducing spontaneously multiple times over the past year. This pattern of hip instability is described as:
View Answer & Explanation
Correct Answer: D
Rationale: The vignette describes a hip that repeatedly dislocates and reduces, which is characteristic of recurrent luxation. The text specifically mentions "recurrent hip luxations" as a problem in Down Syndrome that can lead to fixed dislocation if untreated. Main Distractor Rationale: While congenital hip dysplasia is a predisposing factor, the *pattern* of "popping out and reducing spontaneously multiple times" is best described as recurrent luxation. Septic arthritis, transient synovitis, and SCFE have different clinical presentations.
Question 81
A 13-year-old girl with Down Syndrome is diagnosed with scoliosis. The development of scoliosis in patients with Down Syndrome is primarily attributed to which of the following underlying factors?
View Answer & Explanation
Correct Answer: C
Rationale: The text lists scoliosis as one of the orthopedic abnormalities in Down Syndrome and states that "The most probable origin of these problems is generalized ligamentous laxity." Main Distractor Rationale: While neuromuscular imbalance can contribute to scoliosis in other conditions, the text specifically points to generalized ligamentous laxity as the overarching cause for the listed orthopedic problems in Down Syndrome, including scoliosis.
Question 82
A 6-year-old boy with Down Syndrome is scheduled for an elective surgical procedure unrelated to his spine. Given the common orthopedic issues in this population, what specific spinal condition should be screened for preoperatively due to its potential for catastrophic neurological complications?
View Answer & Explanation
Correct Answer: C
Rationale: The text lists atlanto-axial instability as a significant orthopedic problem in Down Syndrome. This condition, due to ligamentous laxity in the cervical spine, can lead to spinal cord compression, especially during intubation or positioning for surgery, making preoperative screening crucial. Main Distractor Rationale: While other spinal conditions can occur, atlanto-axial instability is uniquely critical in Down Syndrome patients due to the risk of acute neurological injury during procedures requiring neck manipulation.
Question 83
A 16-year-old patient with Down Syndrome presents with severe genu valgum, causing significant functional limitations. Surgical correction is being considered. When planning orthopedic interventions for patients with Down Syndrome, surgeons must be particularly mindful of the generalized tissue property that can affect surgical outcomes and recurrence rates. This property is:
View Answer & Explanation
Correct Answer: C
Rationale: The text repeatedly emphasizes that generalized ligamentous laxity is the "most probable origin" of numerous orthopedic abnormalities in Down Syndrome, including genu valgum. This inherent laxity can impact the stability of surgical repairs and the long-term success of corrective procedures. Main Distractor Rationale: While other factors like bone density or muscle strength might play a role, the text specifically highlights ligamentous laxity as the fundamental underlying issue for the orthopedic problems listed, making it the most critical consideration for surgical planning related to joint stability.
Question 84
A pediatrician is counseling the parents of a newborn diagnosed with Down Syndrome regarding potential future orthopedic issues. The pediatrician explains that a specific generalized musculoskeletal characteristic is highly prevalent in this population and underlies many of these problems. What is the approximate prevalence of generalized ligamentous laxity in patients with Down Syndrome?
View Answer & Explanation
Correct Answer: D
Rationale: The text states, "generalized ligamentous laxity which occurs in almost every Down syndrome patient." Main Distractor Rationale: The phrase "almost every patient" indicates a very high prevalence, far exceeding 25%, 50%, or 75%, and it is not limited to only severe cases.
Question 85
A 17-year-old male with Down Syndrome presents with a chronic limp and significant leg length discrepancy. His history includes multiple episodes of hip dislocation that were never formally treated. Which specific joint is most commonly affected by recurrent luxations that can lead to a fixed dislocation and leg length discrepancy in untreated cases, as described in the provided clinical context?
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly mentions "dislocation of the hip" as one of the orthopedic abnormalities and further elaborates that "Recurrent hip luxations may result fixed dislocation in untreated cases, like this patient with the prominent leg length discrepancy." Main Distractor Rationale: While other joints can be affected by laxity (e.g., patellar luxation in the knee), the text specifically links recurrent luxations leading to fixed dislocation and leg length discrepancy to the hip joint.
Question 86
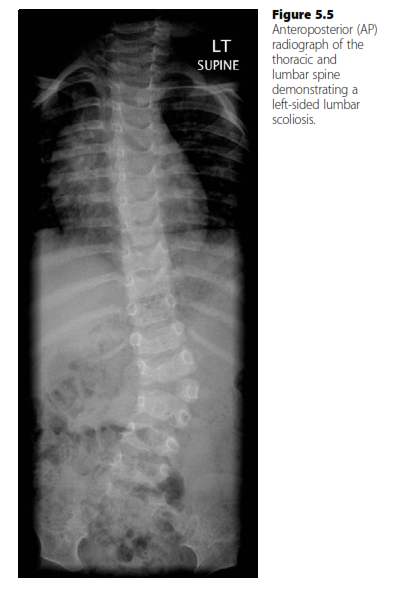
A 13-year-old female presents for evaluation of a progressive spinal deformity. Her mother noticed asymmetry of her back. On physical examination, she has a 10-degree right thoracic rib hump on Adam's forward bend test. Radiographs reveal a 32-degree right thoracic curve from T6 to T12 and a 20-degree left lumbar curve. Her Risser sign is 1.
View Answer & Explanation
Correct Answer: C
Rationale: For adolescent idiopathic scoliosis (AIS) in a skeletally immature patient (Risser 1) with a curve between 25-45 degrees, bracing with a TLSO is the standard of care to prevent curve progression. Observation is typically for curves less than 25 degrees or skeletally mature patients. Spinal fusion is generally reserved for curves greater than 45-50 degrees or those that progress despite bracing. An MRI is not routinely indicated for typical idiopathic curves unless there are atypical features (e.g., left thoracic curve, rapid progression, neurological symptoms, abnormal neurological exam, pain, or very early onset). Physical therapy alone has not been shown to prevent curve progression.
Question 87
A 15-year-old male presents with a worsening right thoracic scoliosis. He was diagnosed with AIS at age 12 and has been compliant with TLSO bracing for the past 2 years. Despite bracing, his curve has progressed from 38 degrees to 52 degrees. He is Risser 4. He denies pain or neurological symptoms.
View Answer & Explanation
Correct Answer: C
Rationale: For skeletally mature or nearly mature patients (Risser 4) with adolescent idiopathic scoliosis (AIS) and a curve greater than 45-50 degrees, especially with documented progression despite bracing, posterior spinal fusion with instrumentation is the most appropriate treatment to prevent further progression and correct the deformity. Continuing bracing is unlikely to be effective given the progression and skeletal maturity. Observation is not appropriate for a 52-degree curve that has progressed. Physical therapy does not prevent curve progression. An MRI is not indicated in the absence of atypical features or neurological symptoms in a typical AIS presentation.
Question 88
A 10-year-old female is referred for evaluation of a mild scoliosis noted during a school screening. She is asymptomatic. On examination, she has a barely perceptible right thoracic prominence on Adam's forward bend test. Standing radiographs show a 19-degree right thoracic curve (T5-T10) and a Risser sign of 0.
View Answer & Explanation
Correct Answer: D
Rationale: For skeletally immature patients (Risser 0) with adolescent idiopathic scoliosis (AIS) and curves less than 25 degrees, observation with serial radiographs is the standard of care. Bracing is typically indicated for curves between 25-45 degrees. Surgical consultation is for curves greater than 45-50 degrees or those that progress significantly. Physical therapy does not prevent curve progression. An MRI is not indicated for this typical presentation of AIS.
Question 89
A 2-year-old male presents with a congenital spinal deformity. His parents noticed a prominent rib on his left side. Radiographs reveal a hemivertebra at T8 on the left, resulting in a 35-degree congenital scoliosis. There are no neurological deficits. A renal ultrasound shows a solitary kidney.
View Answer & Explanation
Correct Answer: C
Rationale: Congenital scoliosis due to a fully segmented hemivertebra has a high risk of progression, especially in the thoracic spine. A 35-degree curve in a 2-year-old is significant and likely to progress, leading to severe deformity. Early surgical intervention, such as hemivertebra excision and fusion, is often recommended to prevent severe progression and minimize the extent of fusion required later. Observation is generally for mild, non-progressive curves or those with balanced deformities. Bracing is typically ineffective for rigid congenital curves. Physical therapy does not correct structural deformities. While genetic counseling may be relevant for associated anomalies, the primary management of the spinal deformity is surgical.
Question 90
A 10-year-old male with Duchenne muscular dystrophy presents with progressive scoliosis and worsening sitting balance. His pulmonary function tests show a forced vital capacity (FVC) of 45% of predicted. Radiographs show a 65-degree thoracolumbar curve. He is non-ambulatory.
View Answer & Explanation
Correct Answer: C
Rationale: Neuromuscular scoliosis, especially in Duchenne muscular dystrophy, is often progressive, long C-shaped, and leads to loss of sitting balance and respiratory compromise. Surgical stabilization is indicated for curves typically greater than 40-50 degrees, especially with functional decline. Due to the progressive nature and pelvic obliquity, fusion often extends to the pelvis (T2-pelvis or T3-pelvis) to maintain sitting balance. The FVC of 45% is a concern but not an absolute contraindication, and surgery can help preserve remaining pulmonary function. Bracing is generally ineffective for progressive neuromuscular curves. Anterior fusion alone is insufficient for long C-curves with pelvic obliquity. Observation is not appropriate for a 65-degree curve with functional decline.
Question 91
A 68-year-old female presents with chronic low back pain radiating into her left buttock and thigh, exacerbated by standing and walking, and relieved by sitting. She reports increasing difficulty standing upright. Physical examination reveals a positive forward stoop and mild weakness in her left L5 distribution. Radiographs show a 40-degree thoracolumbar scoliosis with degenerative changes, disc space narrowing, and facet arthropathy.
View Answer & Explanation
Correct Answer: C
Rationale: This patient presents with symptoms consistent with adult degenerative scoliosis with associated spinal stenosis (neurogenic claudication). Initial management for symptomatic adult degenerative scoliosis typically involves conservative measures such as physical therapy, anti-inflammatory medications, and epidural steroid injections. These treatments aim to alleviate pain and improve function without surgery. Surgical intervention (decompression and fusion) is considered when conservative measures fail, or if there is progressive neurological deficit, severe deformity, or intractable pain. Bracing is generally not effective for long-term management of adult degenerative scoliosis. Anterior column reconstruction alone is insufficient for a complex degenerative deformity with instability and neurological symptoms.
Question 92
A 4-year-old male is diagnosed with a 45-degree right thoracic scoliosis. He has no neurological deficits, and an MRI of the spine is unremarkable. His Risser sign is 0. The curve is progressive.
View Answer & Explanation
Correct Answer: C
Rationale: For early-onset scoliosis (EOS) in young children (typically under 10 years old) with progressive curves, non-fusion techniques are preferred to allow for continued spinal and thoracic growth. Serial casting (e.g., Mehta casts) is a common initial treatment for progressive curves in this age group, aiming for curve correction and prevention of progression without surgery. Bracing can be used but is often less effective than casting for very young children or larger curves. Immediate fusion is generally avoided due to the severe impact on lung development and trunk height. Observation is not appropriate for a progressive 45-degree curve. VBT is a growth modulation technique typically used in older, skeletally immature patients with specific curve patterns, not usually in a 4-year-old.
Question 93
A 12-year-old female presents with a 38-degree left thoracic scoliosis. She reports mild, intermittent back pain but no neurological symptoms. On examination, she has a mild left thoracic rib hump. Her neurological exam is normal. Radiographs show a typical scoliotic curve. Her Risser sign is 2.
View Answer & Explanation
Correct Answer: B
Rationale: A left thoracic curve in an otherwise typical adolescent idiopathic scoliosis presentation is considered an atypical curve pattern. Left thoracic curves are more commonly associated with intraspinal pathology (e.g., Chiari malformation, syringomyelia, spinal cord tumors) than right thoracic curves. Therefore, an MRI of the entire spine is indicated to rule out such underlying conditions before proceeding with treatment for idiopathic scoliosis. While bracing might be considered for a 38-degree curve with Risser 2, it should only be initiated after ruling out intraspinal pathology. Observation is for smaller curves, and surgical consultation is for larger, progressive curves. Physical therapy does not address the underlying etiology or progression.
Question 94
A 14-year-old female with adolescent idiopathic scoliosis has a 42-degree right thoracic curve. Her Risser sign is 4. She is concerned about further progression. Her menarche was at age 12.
View Answer & Explanation
Correct Answer: C
Rationale: A Risser sign of 4 indicates that the patient is nearing skeletal maturity, with only minimal growth remaining. The risk of significant curve progression in adolescent idiopathic scoliosis decreases substantially once a Risser sign of 4 or 5 is reached. While some progression can occur, it is typically much slower and less severe than in skeletally immature patients. Bracing is less effective at this stage, and surgical intervention is usually reserved for curves >45-50 degrees that are still progressing or causing significant symptoms. Therefore, the risk of significant progression is low.
Question 95
A 16-year-old male presents with a known history of adolescent idiopathic scoliosis. To assess his curve, standing posteroanterior and lateral radiographs of the entire spine are obtained. Which of the following best describes the method for measuring the Cobb angle?
View Answer & Explanation
Correct Answer: B
Rationale: The Cobb angle is measured by identifying the most tilted superior and inferior end-vertebrae of the curve. A line is drawn along the superior endplate of the most tilted superior vertebra, and another line is drawn along the inferior endplate of the most tilted inferior vertebra. Perpendicular lines are then drawn from these two lines, and the angle formed by the intersection of these perpendiculars is the Cobb angle. Alternatively, the angle formed by the intersection of the endplate lines themselves can be measured after extending them. Option A describes the endplates of a single vertebra, not a curve. Options C, D, and E describe incorrect methods or anatomical landmarks for Cobb angle measurement.
Question 96
A 16-year-old male presents with a rapidly progressive 70-degree thoracolumbar scoliosis. On physical examination, he is tall and thin, has arachnodactyly, and a positive wrist and thumb sign. Cardiac evaluation reveals aortic root dilation. His family history is positive for similar features and sudden cardiac death.
View Answer & Explanation
Correct Answer: C
Rationale: The constellation of features described – tall stature, thin habitus, arachnodactyly (positive wrist and thumb signs), rapidly progressive scoliosis, and aortic root dilation with a family history of sudden cardiac death – is classic for Marfan Syndrome. Scoliosis in Marfan syndrome is often severe and rapidly progressive, requiring early surgical intervention. Neurofibromatosis Type 1 can cause scoliosis but is associated with café-au-lait spots, neurofibromas, and optic gliomas, not the skeletal and cardiac features described. Cerebral palsy and Duchenne muscular dystrophy cause neuromuscular scoliosis but have distinct presentations. Prader-Willi syndrome is associated with hypotonia, obesity, and developmental delay.
Question 97
A 9-year-old female presents with a 40-degree dystrophic scoliosis. On examination, she has multiple café-au-lait spots, axillary freckling, and cutaneous neurofibromas. An MRI of the spine shows dural ectasia and vertebral scalloping. She has no neurological deficits.
View Answer & Explanation
Correct Answer: D
Rationale: The presence of multiple café-au-lait spots, axillary freckling (Crowe's sign), cutaneous neurofibromas, and dystrophic scoliosis (often short-segment, sharp angulation, and associated with vertebral scalloping and dural ectasia) are pathognomonic for Neurofibromatosis Type 1 (NF1). Scoliosis in NF1 can be either dystrophic (more severe, rapidly progressive, often requiring surgery) or non-dystrophic (similar to idiopathic). Marfan syndrome has different skeletal and cardiac features. Ehlers-Danlos syndrome involves joint hypermobility and skin hyperextensibility. Osteogenesis imperfecta is characterized by brittle bones and blue sclera. Spinal muscular atrophy causes neuromuscular weakness and scoliosis but lacks the cutaneous findings.
Question 98
A 14-year-old female undergoes posterior spinal fusion for a 60-degree right thoracic adolescent idiopathic scoliosis. Intraoperative neuromonitoring (SSEP and MEP) is used. During rod placement, there is a sudden, sustained loss of MEP signals in the lower extremities, while SSEP signals remain stable. The patient is hypotensive.
View Answer & Explanation
Correct Answer: B
Rationale: A sudden, sustained loss of MEP signals (motor evoked potentials) during spinal deformity correction, especially with stable SSEP (somatosensory evoked potentials), is highly concerning for spinal cord ischemia or injury, particularly affecting the anterior spinal cord (which MEPs primarily monitor). The immediate management involves reversing the surgical maneuver (e.g., removing instrumentation, releasing distraction), administering high-dose steroids (e.g., methylprednisolone), and awakening the patient for a neurological examination to confirm the deficit. While hypotension can affect neuromonitoring, a selective loss of MEPs with stable SSEPs points more strongly to a spinal cord issue rather than systemic hypotension alone. Checking electrodes is a first step for any signal change, but given the sustained loss during a critical phase, more aggressive intervention is warranted. Naloxone is for opioid overdose, and increasing anesthesia depth could worsen the situation or mask a neurological deficit.
Question 99
A 16-year-old female undergoes posterior spinal fusion from T4 to L1 for a 65-degree right thoracic scoliosis. One year post-operatively, she develops new onset low back pain and a noticeable increase in her lumbar lordosis. Radiographs show a loss of sagittal balance and a kyphotic deformity developing immediately caudal to her fusion construct, at L2-L3.
View Answer & Explanation
Correct Answer: D
Rationale: The patient's symptoms and radiographic findings describe Distal Junctional Kyphosis (DJK). This is a kyphotic deformity that develops immediately caudal (distal) to a long posterior spinal fusion construct. It is often caused by increased stress on the unfused segments below the fusion, leading to disc degeneration, vertebral collapse, or fracture. Proximal junctional kyphosis (PJK) occurs immediately cranial (proximal) to the fusion. Pseudarthrosis refers to a failure of fusion. Instrumentation failure at the proximal end would typically cause PJK or loss of correction at the top of the construct. Infection would present with different symptoms like fever, redness, and drainage.
Question 100
A 15-year-old female presents with a 55-degree right thoracic scoliosis and a 40-degree compensatory left lumbar curve. She is Risser 3. Her primary goal is maximal cosmetic correction with minimal fusion levels. She has good spinal flexibility on bending films.
View Answer & Explanation
Correct Answer: B
Rationale: Anterior vertebral body tethering (VBT) is a growth modulation technique that can be considered for skeletally immature patients (Risser 0-3) with flexible thoracic or thoracolumbar curves (typically 35-55 degrees) who desire a non-fusion option. It aims to correct the curve while preserving motion and allowing for continued growth. Posterior spinal fusion is a definitive fusion procedure, which the patient wants to minimize. Anterior spinal fusion for a thoracic curve is less common now due to VBT and posterior techniques. Bracing is generally for curves <45 degrees, and observation is for curves <25 degrees or skeletally mature patients. Given the patient's age, curve magnitude, flexibility, and desire for minimal fusion, VBT is a viable option.
You Might Also Like