Master ABOS Orthopedic Board Review: Paget's, Gout, Hyperparathyroidism | Part 5

Key Takeaway
This ABOS Orthopedic Board Review provides multiple-choice questions covering key musculoskeletal pathologies. Topics include Paget's Disease, Gout, Hyperparathyroidism, and Newborn's Septic Arthritis of the Hip, focusing on diagnosis, pathophysiology, and clinical management crucial for board exam preparation.
Master ABOS Orthopedic Board Review: Paget's, Gout, Hyperparathyroidism | Part 5
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 68-year-old man with active Paget's disease requires a total hip arthroplasty for severe secondary osteoarthritis. To minimize the significant risk of intraoperative hemorrhage, which of the following should be administered prior to surgery?
Explanation
Question 2
A 55-year-old woman presents with generalized bone pain, nephrolithiasis, and abdominal discomfort. Hand radiographs are obtained. Which specific radiographic location of subperiosteal bone resorption is considered pathognomonic for her condition?
Explanation
Question 3
A 45-year-old man presents with acute, severe pain, erythema, and swelling in his first metatarsophalangeal joint. Joint aspiration yields fluid that is analyzed under polarizing light microscopy. Which of the following findings confirms the diagnosis of gout?
Explanation
Question 4
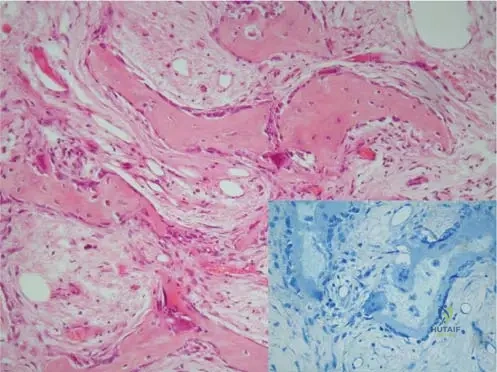
A bone biopsy from a patient with an isolated, markedly elevated serum alkaline phosphatase and an enlarged skull reveals a mosaic pattern of lamellar bone with prominent cement lines. The primary initial pathophysiologic event in this disorder most likely involves which of the following?
Explanation
Question 5
A 60-year-old man presents with chronic nodular swelling of his elbows and fingers. Radiographs show periarticular punched-out lytic lesions with overhanging edges. Which of the following is the most likely composition of these nodules?

Explanation
Question 6
A 48-year-old man with end-stage renal disease presents with a painful lytic lesion in his proximal tibia. Biopsy reveals a spindle cell stroma with numerous multinucleated giant cells and hemosiderin-laden macrophages. What is the most appropriate initial management of this bony lesion?
Explanation
Question 7
A 72-year-old man with long-standing Paget's disease presents with a new onset of severe, unremitting thigh pain and a rapidly enlarging mass. Which of the following is the most likely histologic finding upon biopsy of the mass?
Explanation
Question 8
A patient presents with diffuse bone pain and the following laboratory profile: markedly elevated Parathyroid Hormone (PTH), low-normal serum calcium, and elevated serum phosphorus. Which of the following is the most likely diagnosis?
Explanation
Question 9
A 55-year-old male renal transplant recipient on cyclosporine develops acute podagra. His serum creatinine is 2.8 mg/dL. Which of the following is the most appropriate acute treatment?
Explanation
Question 10
Which of the following neurological complications is most frequently associated with the progressive skull changes seen in Paget's disease?

Explanation
Question 11
A patient with recurrent gout flares and multiple tophi is started on allopurinol for long-term management. What is the primary mechanism of action of this medication?
Explanation
Question 12
Radiographs of the spine in a patient with end-stage renal disease reveal alternating radiolucent and radiodense bands parallel to the vertebral endplates. This "Rugger-Jersey" appearance is primarily due to which of the following?
Explanation
Question 13
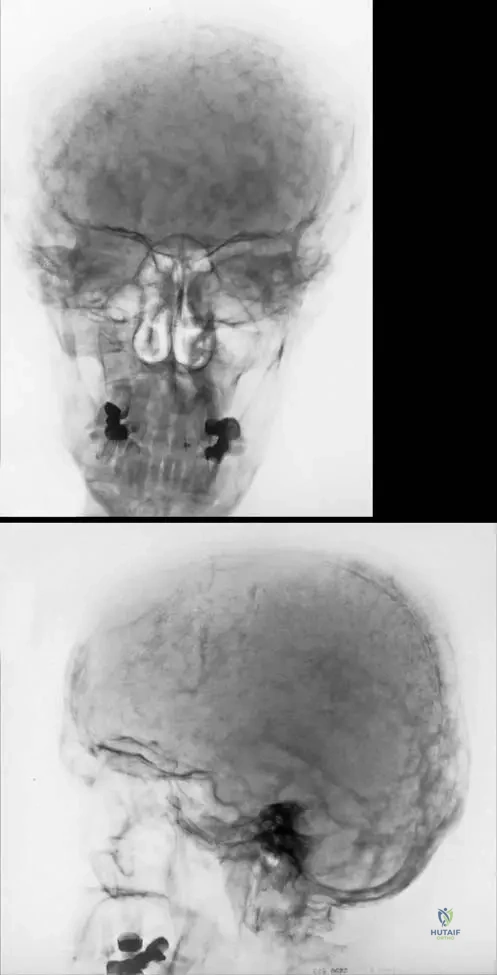
A 65-year-old male presents with increasing hat size and bilateral hearing loss. Radiographs show cortical thickening and a 'cotton-wool' appearance of the skull. Which of the following best describes the primary cellular defect in this condition?
Explanation
Question 14
A 55-year-old male presents with chronic pain and swelling in his left big toe. Radiographs demonstrate a soft tissue mass and a periarticular 'punched-out' lytic lesion with an overhanging sclerotic margin.
Joint aspiration is most likely to reveal which of the following?
Explanation
Question 15
A 48-year-old female with chronic kidney disease presents with generalized bone pain. Hand radiographs show bone resorption along the radial aspect of the middle phalanges of her index and middle fingers. What is the most likely underlying biochemical profile?
Explanation
Question 16
A 72-year-old male with known Paget's disease of the femur presents with a severe, sudden increase in thigh pain over the past month. Radiographs show a new destructive, lytic lesion with cortical breakthrough and a soft tissue mass. What is the most significant prognostic factor for this patient's new condition?
Explanation
Question 17
A 60-year-old male with recurrent gout attacks is started on allopurinol for chronic maintenance therapy. Which of the following best describes the primary mechanism of action of this medication?
Explanation
Question 18
A 40-year-old female sustains a pathologic fracture of her humerus. Radiographs show a well-defined lytic lesion. Biopsy reveals numerous multinucleated giant cells, spindle cells, and extensive hemosiderin deposition.
Which laboratory test is most critical to differentiate this lesion from a primary giant cell tumor of bone?
Explanation
Question 19
A 68-year-old female with severe secondary osteoarthritis of the hip and active Paget's disease is scheduled for a total hip arthroplasty. Her serum alkaline phosphatase is significantly elevated. What is the most appropriate preoperative medical management to optimize her surgical outcome?
Explanation
Question 20
A 52-year-old male with a history of chronic gout on allopurinol 300mg daily presents with an acute, severely painful flare in his right knee. Synovial fluid shows negatively birefringent crystals. What is the most appropriate management of his allopurinol during this acute attack?
Explanation
Question 21
A 72-year-old male with a long history of Paget's disease presents with a 2-month history of rapidly worsening, severe pain in his right thigh. Radiographs demonstrate a new destructive, lytic lesion in the previously thickened cortex of the femur.
What is the most likely diagnosis?
Explanation
Question 22
A 55-year-old male presents with an acutely swollen, erythematous, and exquisitely tender first metatarsophalangeal joint. Joint aspiration is performed. What findings are expected upon polarized light microscopy of the synovial fluid?
Explanation
Question 23
A 48-year-old female with chronic kidney disease presents with a lytic bone lesion in her distal femur. Laboratory studies reveal elevated parathyroid hormone (PTH) and hypercalcemia.
What is the most likely diagnosis of this lesion?
Explanation
Question 24
Which of the following cellular mechanisms is considered the primary initiating event in the pathophysiology of Paget's disease of bone?
Explanation
Question 25
A 60-year-old male with chronic gout currently taking allopurinol 300 mg daily presents to the clinic with an acute gout flare in his left knee. What is the most appropriate modification to his allopurinol regimen during this acute flare?
Explanation
Question 26
A 50-year-old female on hemodialysis complains of diffuse bone pain. Hand radiographs are obtained.
Which of the following radiographic findings is considered pathognomonic for her underlying metabolic bone disease?
Explanation
Question 27
A 68-year-old male with Paget's disease of the tibia presents with worsening bone pain and an elevated serum alkaline phosphatase level. What is the first-line pharmacological treatment for this symptomatic patient?
Explanation
Question 28
A 65-year-old male with long-standing untreated joint pain presents with a swollen, nodular foot. Radiographs display punched-out lytic lesions with overhanging sclerotic margins.
What is the eponymous term for this specific radiographic finding?
Explanation
Question 29
A 45-year-old female with no history of renal disease presents with recurrent nephrolithiasis, diffuse bone pain, and fatigue. Laboratory tests show elevated serum calcium, decreased serum phosphorus, and elevated intact PTH. What is the most likely diagnosis?
Explanation
Question 30
A 74-year-old male with Paget's disease involving the skull complains of gradually worsening hearing loss. What is the most common pathophysiologic mechanism for this specific deficit?
Explanation
Question 31
A 4-year-old boy presents with severe, early-onset gout, developmental delay, and self-mutilating behaviors (lip and finger biting). A deficiency in which of the following enzymes is responsible for this condition?
Explanation
Question 32
A lateral radiograph of the lumbar spine in a patient with end-stage renal disease demonstrates alternating radiolucent and radiopaque bands parallel to the vertebral endplates.
This "rugger jersey" appearance is most characteristic of which condition?
Explanation
Question 33
A 70-year-old male with widespread Paget's disease is scheduled for a total hip arthroplasty due to severe secondary osteoarthritis. Which of the following is a major intraoperative and perioperative anesthetic concern specific to his underlying bone disease?
Explanation
Question 34
A 52-year-old male is prescribed a medication for an acute gout attack. The drug's mechanism of action involves binding to tubulin and inhibiting microtubule polymerization. Which medication was prescribed?
Explanation
Question 35
A 55-year-old female is diagnosed with primary hyperparathyroidism and is found to have a mechanically stable, asymptomatic Brown tumor in her proximal humerus. What is the most appropriate initial management for the bone lesion?
Explanation
Question 36
When performing a total knee arthroplasty in a patient with advanced Paget's disease of the tibia, which of the following statements regarding the expected surgical outcome and technical considerations is most accurate?

Explanation
Question 37
A 62-year-old male is being treated for hypertension and subsequently develops his first acute gout attack. Which of the following antihypertensive medications is most likely responsible for precipitating this attack by decreasing renal urate excretion?
Explanation
Question 38
A biopsy is taken from a lytic bone lesion in a patient with severe untreated secondary hyperparathyroidism. What is the classic histologic appearance of this lesion?
Explanation
Question 39
Which of the following laboratory profiles is most characteristic of isolated, uncomplicated Paget's disease of bone?
Explanation
Question 40
A 60-year-old male with chronic tophaceous gout presents with a large, draining mass over his olecranon.
Which of the following is an absolute indication for surgical excision of a gouty tophus?

Explanation
Question 41
A 65-year-old male presents with increasing hat size, hearing loss, and anterior bowing of his tibias. What is the primary cellular defect that initiates the pathogenesis of this condition?
Explanation
Question 42
A 50-year-old male presents with severe acute pain in his first metatarsophalangeal joint. Joint aspiration is performed.
Under compensated polarized light microscopy, what are the expected characteristics of the causative crystals?
Explanation
Question 43
A 45-year-old female with end-stage renal disease presents with diffuse bone pain. A radiograph of her hand is obtained.
What is the pathognomonic radiographic finding of her bone disease at this anatomical site?
Explanation
Question 44
A 70-year-old female with a long-standing history of polyostotic Paget's disease presents with new-onset, severe, and unrelenting pain in her right thigh. Radiographs demonstrate a new destructive, lytic lesion in previously pagetoid bone. What is the most likely diagnosis?
Explanation
Question 45
A 60-year-old male with recurrent gout attacks requires long-term urate-lowering therapy. He has a history of multiple radiolucent kidney stones. Which of the following medications is strictly contraindicated for this patient?
Explanation
Question 46
A 55-year-old male presents with generalized weakness and nephrolithiasis. Radiographs reveal a lytic bone lesion. Biopsy shows abundant giant cells, hemosiderin-laden macrophages, and a background of spindle cells.
What is the most likely serum laboratory profile for this patient?
Explanation
Question 47
An asymptomatic 68-year-old male undergoes a routine pelvic radiograph which demonstrates cortical thickening and sclerosis of the right iliopectineal line (Brim sign).
What is the classic serum laboratory profile associated with this condition?
Explanation
Question 48
A 55-year-old male with chronic untreated joint pain presents with palpable nodular masses around his joints. Radiographs of his feet are obtained.
Which radiographic description best characterizes the classic bony erosions seen in this condition?
Explanation
Question 49
In a patient with end-stage renal disease who develops secondary hyperparathyroidism, what is the primary pathophysiological trigger for the parathyroid gland hyperplasia?
Explanation
Question 50
A 72-year-old male with symptomatic Paget's disease involving the right hemipelvis and proximal femur is scheduled for a total hip arthroplasty. What perioperative medical management is highly recommended to minimize surgical complications?
Explanation
Question 51
A 40-year-old male develops his first acute gout flare in the great toe two weeks after his primary care physician started him on a new antihypertensive medication. Which of the following medications most likely precipitated this event by decreasing renal uric acid excretion?
Explanation
Question 52
An 80-year-old male complains of progressive bilateral hearing loss. A lateral skull radiograph demonstrates mixed radiolucent and radiopaque areas with marked thickening of the calvarium.
What is the classic descriptive term for this radiographic appearance?
Explanation
Question 53
A 48-year-old female with long-standing secondary hyperparathyroidism undergoes spine radiography for chronic back pain. Which of the following radiographic signs is classically associated with her condition?
Explanation
Question 54
A 58-year-old male hospitalized for severe COPD exacerbation develops acute, intense swelling and erythema in his left knee. Synovial fluid analysis confirms acute gout. He has Stage 4 chronic kidney disease (eGFR 20 mL/min). What is the safest acute treatment option?
Explanation
Question 55
A patient with symptomatic Paget's disease is started on zoledronic acid. What is the specific cellular mechanism of action of this medication?
Explanation
Question 56
A 50-year-old female is incidentally diagnosed with asymptomatic primary hyperparathyroidism during routine labs. Which of the following is considered an accepted criterion for recommending parathyroidectomy in this asymptomatic patient?
Explanation
Question 57
Aspiration of an acutely inflamed metatarsophalangeal joint in a 45-year-old male yields fluid with 25,000 WBCs/mcL, predominantly consisting of a specific inflammatory cell. The inflammation is heavily driven by the NLRP3 inflammasome. Which cell type and cytokine are primarily driving this acute gouty inflammation?
Explanation
Question 58
A bone biopsy is obtained from a thickened, clinically warm tibia in a 70-year-old male to rule out malignancy.
If this lesion represents the classic underlying metabolic disease, what is the histological hallmark expected on biopsy?
Explanation
Question 59
A 65-year-old man with a known history of Paget's disease presents with a new onset of severe, unrelenting thigh pain and swelling over the past two months. Radiographs reveal a new, destructive lytic lesion in the femur with cortical breakthrough. What is the most likely diagnosis?
Explanation
Question 60
A 45-year-old male presents with an acutely painful, swollen, and erythematous first metatarsophalangeal joint.
Synovial fluid aspiration is performed. Under compensated polarized light microscopy, what crystal characteristics confirm the suspected diagnosis?
Explanation
Question 61
A 48-year-old female with chronic kidney disease presents with diffuse bone pain.
Hand radiographs demonstrate subperiosteal bone resorption. Where is this radiographic finding most classically located?
Explanation
Question 62
A 70-year-old female with active polyostotic Paget's disease requires an elective total hip arthroplasty for severe secondary osteoarthritis. To minimize intraoperative blood loss, which of the following is the most appropriate preoperative medical intervention?
Explanation
Question 63
A patient with secondary hyperparathyroidism presents with a well-demarcated lytic bone lesion in the distal radius. A biopsy is performed. Which histological description best characterizes a Brown tumor?
Explanation
Question 64
Which of the following radiographic features is considered pathognomonic for chronic tophaceous gout?
Explanation
Question 65
Paget's disease of bone progresses through three distinct pathophysiological phases. Which cellular mechanism initiates the primary lytic phase of the disease?
Explanation
Question 66
A 55-year-old female presents with lethargy, abdominal pain, and bone pain. Laboratory evaluation reveals elevated serum parathyroid hormone (PTH). Which set of additional laboratory findings confirms the diagnosis of primary hyperparathyroidism?
Explanation
Question 67
A 52-year-old man with recurrent gout attacks is prescribed a medication for long-term management to prevent future flares. The prescribed medication works by inhibiting xanthine oxidase. What is this medication?
Explanation
Question 68
In a patient suspected of having Paget's disease, what is the most sensitive imaging modality for identifying the extent of polyostotic skeletal involvement?
Explanation
Question 69
A patient with long-standing end-stage renal disease presents with back pain. Lateral radiographs of the lumbar spine demonstrate prominent radiodense bands at the superior and inferior endplates of the vertebral bodies. This classic 'rugger jersey spine' is indicative of which condition?
Explanation
Question 70
A 60-year-old male with an acute gout flare in his knee has a medical history significant for stage 4 chronic kidney disease and a recent bleeding gastric ulcer. Which is the safest and most appropriate acute treatment option for his knee?
Explanation
Question 71
A 72-year-old man with a long history of Paget's disease presents with a 2-month history of worsening, unrelenting right thigh pain and a newly palpable mass. Radiographs reveal a destructive lytic lesion with cortical breakthrough in the mid-diaphysis of his thickened, bowed right femur. Which of the following is the most likely diagnosis?
Explanation
Question 72
A 60-year-old man presents with chronic pain and swelling in his left big toe. Radiographs show a well-defined periarticular erosion with an 'overhanging margin' and preserved joint space.
What is the primary composition of the crystalline deposit responsible for this lesion?
Explanation
Question 73
A 55-year-old woman is evaluated for generalized bone pain and recurrent nephrolithiasis. Dual-energy x-ray absorptiometry reveals severe cortical bone loss. Her laboratory profile will most likely show which of the following?
Explanation
Question 74
A bone biopsy is obtained from the pelvis of an asymptomatic 65-year-old man who was noted to have an incidental sclerotic lesion on a radiograph. Histological examination reveals a disordered, 'mosaic' pattern of lamellar bone with prominent, irregular cement lines. The primary initial defect in this patient's disease process involves which of the following cell types?
Explanation
Question 75
A 48-year-old man with end-stage renal disease presents with severe diffuse bone pain. Radiographs demonstrate a 'rugger-jersey' spine and diffuse osteopenia. His condition is primarily driven by the failure of the kidneys to synthesize which of the following?
Explanation
Question 76
A 52-year-old man with a history of recurrent gouty attacks is started on allopurinol for long-term management. Through which of the following mechanisms does this medication exert its therapeutic effect?
Explanation
Question 77
A 70-year-old woman with Paget's disease presents with increasing right thigh pain and bowing of the femur. She is prescribed an intravenous nitrogen-containing bisphosphonate (zoledronic acid). This class of medication functions primarily by inhibiting which of the following enzymes?
Explanation
Question 78
A 40-year-old woman presents with a pathologic fracture of her left humerus. A radiograph reveals a lytic, expansile lesion. Biopsy shows clusters of multinucleated giant cells within a highly vascular, hemorrhagic stroma containing hemosiderin-laden macrophages.
Which of the following tests is most critical to confirm the underlying etiology?
Explanation
Question 79
A 66-year-old man with polyostotic Paget's disease presents with progressively worsening lower extremity weakness, numbness, and difficulty walking. Radiographs of the lumbar spine reveal an enlarged 'ivory vertebra' at L3. What is the most likely etiology of his neurological symptoms?
Explanation
Question 80
A 55-year-old man undergoes excision of a large, chalky white mass overlying his olecranon. The surgeon suspects a gouty tophus. To accurately preserve the diagnostic crystals for histopathological examination, the specimen should be fixed in which of the following solutions?
Explanation
Question 81
A 72-year-old man presents with progressive bowing of his right tibia and a deep, aching bone pain. Radiographs show cortical thickening and trabecular coarsening. A bone biopsy reveals woven bone with a mosaic pattern of prominent cement lines. Which of the following describes the primary cellular abnormality responsible for this condition?
Explanation
Question 82
A 45-year-old woman with end-stage renal disease presents with a painful lytic lesion in her proximal tibia. Laboratory tests reveal significantly elevated parathyroid hormone (PTH) and low serum calcium. A biopsy of the lesion is performed. What is the characteristic histological finding expected in this lesion?
Explanation
Question 83
A 52-year-old man presents with chronic foot pain and nodular swellings around his toes. Radiographs of the foot show periarticular erosions with sclerotic margins and overhanging edges (so-called 'rat bite' erosions).
What is the composition of the crystals associated with this radiographic appearance?
Explanation
Question 84
A 76-year-old man with a long-standing history of Paget's disease involving his pelvis presents with severe, progressive, and unremitting left hip pain over the past 2 months. Recent radiographs demonstrate a new destructive, permeative lytic lesion with cortical breakthrough. What is the most likely diagnosis for this new lesion?
Explanation
Question 85
A 60-year-old woman is diagnosed with primary hyperparathyroidism due to a parathyroid adenoma. Dual-energy X-ray absorptiometry (DEXA) demonstrates generalized osteopenia. Parathyroid hormone (PTH) stimulates bone resorption primarily by binding directly to receptors on which of the following cell types?
Explanation
Question 86
A 55-year-old man with recurrent gouty arthropathy is started on daily allopurinol for long-term medical management. Which of the following describes the primary mechanism of action of this medication?
Explanation
Question 87
A 68-year-old man presents with bilateral leg pain and neurogenic claudication. Radiographs of the lumbar spine demonstrate an enlarged, dense L4 vertebral body with thickened cortices ('picture frame' vertebra).
What is the most likely pathophysiological mechanism for this patient's neurologic symptoms?
Explanation
Question 88
A 42-year-old man presents with an acutely swollen and erythematous right knee. Joint aspiration yields synovial fluid with a white blood cell count of 35,000/uL. Under polarized light microscopy with a red compensator, the crystals appear yellow when aligned parallel to the axis of the compensator. Which of the following is the most likely diagnosis?
Explanation
Question 89
A 58-year-old man with end-stage renal disease (ESRD) presents with diffuse bone pain. He is diagnosed with renal osteodystrophy and secondary hyperparathyroidism. Which of the following laboratory profiles is most consistent with this patient's condition?
Explanation
Question 90
A 70-year-old woman is diagnosed with active Paget's disease due to severe long bone pain and markedly elevated alkaline phosphatase. She is prescribed intravenous zoledronic acid. What is the primary intracellular target of this class of medication?
Explanation
None
