ABOS Part I Orthopedic Review: Shoulder, Knee, Foot, Ankle & Ligament Surgery | Part 22222

Key Takeaway
This ABOS Part I Review module offers 40 advanced orthopedic multiple-choice questions mirroring the ABOS Part I and AAOS OITE exams. It covers high-yield topics including shoulder imaging, rotator cuff arthropathy, knee meniscus and ligament injuries (ACL, PCL), and rheumatoid foot and ankle pathology, providing detailed explanations for comprehensive board preparation.
ABOS Part I Orthopedic Review: Shoulder, Knee, Foot, Ankle & Ligament Surgery | Part 22222
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
An 84-year-old female presents after a fall onto her outstretched hand. You are asked to describe her shoulder X-ray. Which of the following views is most critical for definitively diagnosing a posterior glenohumeral dislocation when an AP view shows a 'lightbulb' sign?
Explanation
Correct Answer: C
The axillary view is the gold standard for assessing glenohumeral joint congruity and confirming the direction of dislocation (anterior or posterior). While the 'lightbulb' sign on an AP view is suggestive of posterior dislocation, it is not definitive. The Scapular Y view can indicate posterior dislocation if the humeral head is posterior to the glenoid, but it's a sagittal view. The West Point and Stryker notch views are specific for glenoid rim defects or Hill-Sachs lesions, respectively, not primary dislocation diagnosis.
Question 2
An 84-year-old woman presents with long-standing shoulder pain and weakness, with active elevation limited to 60 degrees. Her X-ray shows superior migration of the humeral head, acromial erosion, and significant glenohumeral joint space narrowing. Which of the following is the most likely diagnosis?
Explanation
Correct Answer: C
Rotator cuff arthropathy (RCA) is characterized by chronic, massive rotator cuff tears leading to superior migration of the humeral head, resulting in direct articulation between the humeral head and the acromion. This pathological contact causes secondary degenerative changes, including acromial erosion, glenohumeral joint space narrowing (typically superiorly), and often extensive osteophyte formation. Primary glenohumeral osteoarthritis usually shows concentric or inferior joint space narrowing without significant superior migration. CPPD can cause degenerative changes but not typically with this degree of superior migration. Adhesive capsulitis shows no significant radiographic findings. Seronegative spondyloarthropathies would show erosive changes, often with sacroiliitis, but not the specific pattern of RCA.
Question 3
An 84-year-old osteoporotic lady sustains a proximal humerus fracture after a low-energy fall. Her X-ray shows a fracture involving the surgical neck, greater tuberosity, and lesser tuberosity, with articular displacement. According to the Neer classification, how would you classify this fracture?
Explanation
Correct Answer: C
The Neer classification divides the proximal humerus into four anatomical parts: the humeral head (articular segment), greater tuberosity, lesser tuberosity, and humeral shaft. A fracture involving all three tuberosities and the surgical neck (which separates the head from the shaft) constitutes four distinct displaced segments, thus classifying it as a 4-part fracture. Each displaced segment (>1cm displacement or >45 degrees angulation) counts as a 'part.' A 2-part involves one displaced segment, a 3-part involves two displaced segments (e.g., head + greater tuberosity + shaft). Articular displacement is a characteristic of 4-part fractures but not a primary classification part itself. Valgus-impacted is a specific stable variant, usually 2- or 3-part.
Question 4
When reviewing the shoulder X-ray of an 84-year-old female, which radiographic finding is most indicative of severe osteoporosis, beyond just fracture presence?
Explanation
Correct Answer: C
Trabecular thinning and cortical attenuation (thinning of the outer bone layer) are direct radiographic signs of reduced bone mineral density characteristic of osteoporosis. While osteoporosis predisposes to fractures, the other options are signs of degenerative joint disease (subchondral cysts, joint space narrowing, osteophyte formation) or rotator cuff arthropathy (acromial erosion), not direct indicators of systemic bone density loss.
Question 5
An X-ray of an 84-year-old lady's shoulder shows significant inferomedial glenohumeral joint space narrowing, subchondral sclerosis, and large inferior osteophytes. There is no evidence of superior migration of the humeral head. Which diagnosis is most consistent with these findings?
Explanation
Correct Answer: C
Primary glenohumeral osteoarthritis (GHOA) typically presents with inferomedial joint space narrowing, subchondral sclerosis, and significant osteophyte formation, particularly inferiorly (humeral head and glenoid). Crucially, there is no superior migration of the humeral head, differentiating it from rotator cuff tear arthropathy. CPPD can mimic OA but often shows chondrocalcinosis. Septic arthritis would show rapid joint destruction, effusion, and possibly periarticular osteopenia, less typically prominent osteophytes. Avascular necrosis would show subchondral collapse, crescent sign, and eventual secondary OA.
Question 6
An 84-year-old lady presents with recurrent anterior glenohumeral instability. Which specialized radiographic view is most effective for visualizing a bony Bankart lesion or an anterior glenoid rim fracture?
Explanation
Correct Answer: B
The West Point axillary view is specifically designed to profile the anterior-inferior glenoid rim, making it superior for detecting bony Bankart lesions or anterior glenoid rim fractures, which are common sequelae of anterior glenohumeral dislocation. The Stryker Notch view is for Hill-Sachs lesions (posterolateral humeral head compression fracture). The Scapular Y view assesses dislocation direction. The Grashey view is a true AP. The Apical Oblique view can also show glenoid rim pathology but less specifically than West Point.
Question 7
When describing the shoulder X-ray of an elderly patient, you note an apparent non-union of the acromion. Which specific view would be most crucial to confirm an os acromiale and differentiate it from an acute fracture?
Explanation
Correct Answer: C
The outlet view (or supraspinatus outlet view) is optimal for evaluating the acromial morphology, including the presence of an os acromiale, by projecting the acromion en face. An os acromiale is a developmental failure of fusion of the acromial apophyses. While other views might incidentally show it, the outlet view provides the best profile. The Zanca view is specific for the AC joint. Axillary view is for glenohumeral congruity. Transthoracic is for humeral shaft.
Question 8
A 'Grashey view' is requested for an 84-year-old female's shoulder. What is the primary purpose of this specific projection?
Explanation
Correct Answer: C
The Grashey view is a 'true AP' view of the glenohumeral joint, achieved by internally rotating the patient approximately 30-45 degrees to align the glenoid parallel to the X-ray beam. This eliminates overlap of the humeral head and glenoid, allowing for accurate assessment of joint space and articulation. While rotator cuff integrity cannot be assessed directly, its sequelae (e.g., superior migration) are better appreciated.
Question 9
On an AP internal rotation view of an 84-year-old woman's shoulder, which anatomical landmark is best visualized en face?
Explanation
Correct Answer: B
The AP internal rotation view brings the lesser tuberosity into profile, facing medially. The greater tuberosity is seen medially overlapping the humeral head. Conversely, the AP external rotation view profiles the greater tuberosity laterally.
Question 10
When reviewing an AP external rotation view of an elderly patient's shoulder, which structure is typically seen in profile laterally on the humeral head?
Explanation
Correct Answer: B
The AP external rotation view rotates the humerus externally, bringing the greater tuberosity into profile on the lateral aspect of the humeral head. The lesser tuberosity is then positioned anteriorly and medially, often superimposing on the humeral head.
Question 11
Regarding the collagenous architecture of the menisci, which of the following statements most accurately describes the predominant fiber orientation in the main body of the meniscal substance, critical for its biomechanical function?
Explanation
Correct Answer: B
The menisci are primarily composed of type I collagen, with the vast majority (90-95%) of the fibers arranged circumferentially. These longitudinal fibers are crucial for converting vertical compressive loads into 'hoop stresses,' which are then resisted by the integrity of the circumferential fibers, allowing the meniscus to transmit load efficiently and protect articular cartilage. Radial fibers, though fewer, act as 'tie-ropes' to prevent extrusion of the circumferential fibers, but they are not the predominant orientation for resisting hoop stresses.
Question 12
Which meniscal structure is considered a secondary stabilizer to anterior tibial translation, particularly in the ACL-deficient knee?
Explanation
Correct Answer: A
The posterior horn of the medial meniscus plays a significant role as a secondary stabilizer to anterior tibial translation. Its posterior root attachment resists anterior displacement of the meniscus itself, and its intact structure prevents excessive anterior translation of the tibia relative to the femur, especially when the ACL is deficient. The posterior horn of the lateral meniscus also contributes but to a lesser degree than the medial. The anterior horns and the body of the meniscus have less direct influence on resisting anterior tibial translation.
Question 13
The primary blood supply to the menisci in adults is derived from which arterial network?
Explanation
Correct Answer: A
The primary blood supply to the menisci in adults originates from branches of the inferior genicular arteries (medial and lateral), which form a perimeniscal plexus. This plexus supplies the outer 10-30% of the meniscal tissue, creating the well-known 'red-red' (vascular), 'red-white' (partially vascular), and 'white-white' (avascular) zones. The superior genicular arteries contribute to the suprapatellar region but not directly to the meniscal periphery.
Question 14
In terms of meniscal innervation, which region is primarily responsible for proprioceptive feedback?
Explanation
Correct Answer: C
The menisci are innervated primarily in their vascularized periphery, particularly the anterior and posterior horns. Mechanoreceptors (Ruffini endings, Pacinian corpuscles, Golgi tendon organ-like endings) and free nerve endings are concentrated in these regions, contributing to proprioception and nociception. The inner two-thirds (white-white zone) are largely aneural and thus lack significant innervation for proprioception.
Question 15
What is the primary role of radial 'tie' fibers within the meniscal substance?
Explanation
Correct Answer: C
While the circumferential fibers bear the hoop stresses, the relatively fewer radial 'tie' fibers act like 'sutures' or 'staples,' connecting the circumferential bundles. Their critical role is to resist meniscal extrusion by preventing the outward bulging and separation of the circumferential fibers under compressive loads, thus maintaining the meniscus's integrity and function. They do not provide the main load-bearing structure or directly resist A-P translation as their primary role.
Question 16
Which meniscal root attachment is considered stronger and has a higher load-to-failure threshold?
Explanation
Correct Answer: C
The posterior horn of the medial meniscus root attachment is biomechanically the strongest, resisting high loads and contributing significantly to posterior stability. Disruption of this root attachment effectively renders the medial meniscus non-functional, leading to biomechanical consequences similar to a total meniscectomy. While other root attachments are important, the posterior medial root is consistently shown to be the most robust.
Question 17
A discoid meniscus is an anatomical variant most commonly affecting which meniscus?
Explanation
Correct Answer: B
A discoid meniscus is an abnormally shaped, usually thicker and wider, meniscus that is prone to tearing. It most commonly affects the lateral meniscus, with the 'complete' type being the most recognized. It can be asymptomatic or present with snapping, pain, or locking, particularly with activity. While incomplete types exist, the lateral complete discoid meniscus is the classic presentation.
Question 18
What is the typical water content of a healthy adult meniscus?
Explanation
Correct Answer: C
The meniscus is rich in water, which accounts for approximately 70-80% of its wet weight in healthy adults. This high water content, along with the proteoglycan matrix, contributes to its viscoelastic properties and ability to distribute loads and absorb shock. With age and degeneration, water content can decrease, affecting its biomechanical function.
Question 19
The meniscofemoral ligaments (of Humphry and Wrisberg) are associated with which meniscal horn and may provide some additional stabilization?
Explanation
Correct Answer: D
The meniscofemoral ligaments (MFLs) are typically associated with the posterior horn of the lateral meniscus. The ligament of Wrisberg passes posterior to the PCL, and the ligament of Humphry passes anterior to the PCL. While their primary function is debated, they are thought to provide some accessory stabilization to the posterior horn of the lateral meniscus and may provide stability in the setting of an absent or deficient PCL.
Question 20
Which statement best describes the healing potential of a longitudinal tear in the inner one-third (white-white zone) of the meniscus?
Explanation
Correct Answer: C
The inner one-third (white-white zone) of the meniscus is avascular. Without a direct blood supply, intrinsic healing of tears in this region is extremely poor to non-existent. Surgical repair in this zone is generally not indicated as it has a very low success rate, hence partial meniscectomy is often the treatment. While age can influence healing, the primary determinant in this zone is the lack of vascularity.
Question 21
During the initial inspection of a patient with rheumatoid arthritis presenting with foot pain, which of the following findings MOST reliably suggests active synovitis rather than fixed deformity?
Explanation
Correct Answer: C
Warmth and erythema are cardinal signs of acute inflammation, indicative of active synovitis. Fixed hallux valgus, bunionette deformity, callosities, and MTPJ subluxation/dislocation are all consequences of chronic rheumatoid disease and represent fixed deformities or secondary skin changes, not necessarily active inflammation at the time of examination.
Question 22
When performing a detailed palpation of the rheumatoid forefoot, which anatomical landmark is crucial for identifying early MTP joint synovitis, particularly in the lesser toes?
Explanation
Correct Answer: E
The plantar aspect of the MTP joint capsule is often the most sensitive area for detecting early synovitis in the lesser toes. The synovium typically expands inferiorly, and gentle palpation with two fingers, one dorsally and one plantarly, can elicit tenderness and reveal a boggy sensation indicative of inflammation. Dorsal palpation can also be useful, but the plantar side often presents earlier and more prominently.
Question 23
A patient with advanced rheumatoid arthritis presents with a severe forefoot deformity. On examination, you observe a 'telescoping' of the toes. This finding is MOST consistent with:
Explanation
Correct Answer: D
'Telescoping' of the toes, where the proximal phalanx appears to shorten into the metatarsal, is a classic sign of complete MTP joint dislocation with dorsal subluxation or dislocation of the phalanx relative to the metatarsal head. This leads to the characteristic 'cock-up' deformity and often involves the lesser toes. Plantar fat pad migration is a related but distinct consequence, and the other options describe less severe or different deformities.
Question 24
During a gait assessment of a rheumatoid patient, you observe a 'toe-off' phase that is significantly limited or absent. This finding is MOST directly attributable to:
Explanation
Correct Answer: D
The 'toe-off' phase of gait primarily relies on the push-off power generated by the MTP joints, especially the first MTP joint (hallux). Pain, stiffness, and deformity (e.g., hallux rigidus or MTP subluxation/dislocation) in these joints severely impair the ability to properly perform toe-off, leading to a propulsive gait pattern often described as an 'apathetic' or 'shuffle' gait. While other deformities can affect gait, this specific limitation points directly to forefoot pathology.
Question 25
Which of the following physical examination maneuvers is BEST for assessing the flexibility of a pes planovalgus deformity in a patient with rheumatoid arthritis?
Explanation
Correct Answer: C
Observing the arch height while standing on toes (a modification of the Jack's test or heel-rise test) is the most effective way to assess the flexibility of a pes planovalgus deformity. If the arch reconstitutes or significantly improves with a single heel-rise, the deformity is largely flexible. If the arch remains collapsed, it indicates a rigid deformity, which has significant implications for treatment planning. The 'too many toes' sign indicates hindfoot valgus but not flexibility. Tarsal Tunnel test is for nerve compression. Palpation of the posterior tibial tendon assesses tendon integrity but not overall arch flexibility.
Question 26
A 55-year-old female with long-standing rheumatoid arthritis presents with chronic forefoot pain and difficulty wearing shoes. On examination, you note diffuse callosities under the metatarsal heads and migration of the plantar fat pad anteriorly. This fat pad migration primarily contributes to her symptoms by:
Explanation
Correct Answer: C
Plantar fat pad migration is a common finding in advanced rheumatoid forefoot disease. As the MTP joints subluxate dorsally, the protective fat pad, which normally provides cushioning under the metatarsal heads, migrates distally, exposing the metatarsal heads directly to the ground during weightbearing. This loss of natural cushioning leads to significantly increased pressure, pain, and secondary callosity formation, which are major contributors to the patient's symptoms.
Question 27
When examining the midfoot of a rheumatoid patient, persistent tenderness and swelling over the talonavicular joint, even without a significant pes planovalgus deformity, should raise suspicion for:
Explanation
Correct Answer: C
The talonavicular joint is a key component of the midfoot and is frequently involved early in rheumatoid arthritis. Persistent tenderness and swelling directly over this joint are strong indicators of active synovitis or early arthritic changes. While other conditions can cause midfoot pain, localized tenderness and swelling specifically at the talonavicular joint points to its direct involvement. Achilles tendinopathy affects the hindfoot, peroneal tendon pathology is more lateral, tarsal tunnel syndrome involves nerve compression, and plantar fasciitis typically causes heel pain.
Question 28
A 'pump bump' or Haglund's deformity is a bony prominence on the posterior calcaneus. In a rheumatoid patient, a similar posterior heel prominence associated with inflammation and tenderness suggests:
Explanation
Correct Answer: B
Retrocalcaneal bursitis is a common inflammatory condition in rheumatoid arthritis, characterized by inflammation of the bursa located between the Achilles tendon and the superior aspect of the calcaneus. This can cause pain, swelling, and tenderness at the posterior heel, mimicking aspects of a 'pump bump' but due to inflammation rather than purely bony prominence. While Achilles tendinosis can coexist, the inflammation points specifically to bursitis.
Question 29
Which of the following statements regarding the assessment of the rheumatoid hindfoot is TRUE?
Explanation
Correct Answer: D
Fixed hindfoot valgus is a common and debilitating deformity in rheumatoid arthritis, often due to collapse of the medial longitudinal arch and subtalar joint involvement. It is best assessed by observing the alignment of the heel relative to the lower leg from a posterior perspective during weightbearing. Subtalar joint motion primarily allows inversion and eversion, not dorsiflexion/plantarflexion (which is ankle motion). The 'too many toes' sign indicates hindfoot valgus (and compensatory forefoot abduction). Hindfoot valgus is more common than varus. Ankle joint involvement, while less frequent than midfoot/forefoot, can occur and significantly impact gait.
Question 30
When evaluating a patient with severe rheumatoid forefoot deformity prior to surgical correction, the presence of a 'positive paper test' (unable to slide a thin piece of paper under the metatarsal heads) indicates:
Explanation
Correct Answer: C
A 'positive paper test' indicates that the metatarsal heads are pressing firmly against the ground due to fixed MTP joint dorsiflexion, subluxation, or dislocation. This means the metatarsal heads are prominent plantarly and bear excessive weight, often leading to pain and callosities. It signifies a fixed deformity that is unlikely to correct with conservative measures and often requires surgical intervention.
Question 31
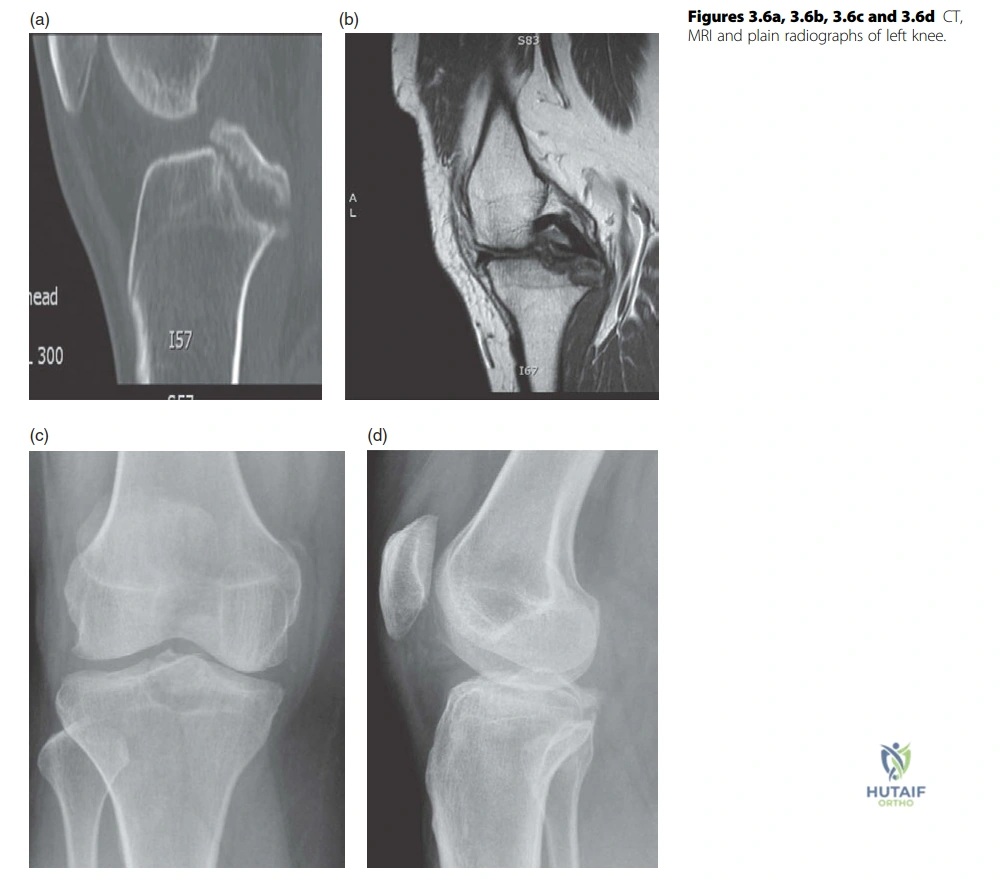
A 26-year-old rugby player presents after an awkward fall onto his left knee during a tackle. Clinical examination reveals a posterior sag and a positive posterior drawer test. Radiographs and MRI are obtained, as shown in the image below. Based on the findings, what is the most appropriate initial management for this patient's primary knee injury?
Explanation
Correct Answer: C
The case describes a 26-year-old rugby player with a PCL injury, and the images show a cortical disruption at the PCL insertion with a displaced avulsed fragment. The candidate in the viva correctly identifies this as a large, displaced avulsion fragment. For a displaced PCL avulsion fracture, especially in a young, active athlete, open reattachment of the fragment is the preferred treatment to restore PCL integrity and knee stability. The candidate in the case specifically states, 'I would offer this patient reattachment of the PCL avulsion through open procedure.'
- Option A (Non-operative management with bracing and physical therapy): While non-operative management can be considered for isolated, non-displaced PCL tears or mid-substance tears in less active individuals, it is generally not appropriate for a significantly displaced bony avulsion in an active athlete, as it would likely lead to persistent instability and poor functional outcomes.
- Option B (Arthroscopic PCL reconstruction with allograft): PCL reconstruction (arthroscopic or open) is typically reserved for mid-substance PCL tears or chronic PCL instability. In this case, there is a bony avulsion, which is amenable to direct reattachment, offering superior bone-to-bone healing and often better outcomes than a reconstruction with an allograft for this specific injury pattern.
- Option D (Posterior capsular repair with augmentation): A posterior capsular repair might be part of a broader reconstruction or repair strategy if there's significant capsular injury, but it does not address the primary issue of the displaced bony PCL avulsion.
- Option E (Acute arthroscopic debridement and observation): Debridement alone would not stabilize the displaced fragment and would lead to persistent instability. Observation is not appropriate for a displaced bony avulsion in an active individual.
Question 32
During the viva, the candidate describes the posterior approach to the knee. Which of the following is NOT a commonly accepted indication for utilizing a posterior approach to the knee?
Explanation
Correct Answer: D
The candidate explicitly lists the indications for a posterior approach to the knee: 'The indications include removal of popliteal cysts and neoplasms, posterior synovectomy, open reduction and internal fixation of posterior tibial plateau shear fractures, fixation of bone avulsions associated with a posterior cruciate ligament (PCL) injury, repair of posterior vascular injuries, and more recently, posterior inlay PCL reconstructions.'
- Option A (Open reduction and internal fixation of posterior tibial plateau shear fractures): This is a direct indication mentioned in the text.
- Option B (Fixation of bone avulsions associated with a posterior cruciate ligament (PCL) injury): This is the specific injury discussed in the case and is a direct indication mentioned.
- Option C (Repair of posterior vascular injuries): This is a direct indication mentioned in the text.
- Option E (Removal of popliteal cysts and neoplasms): This is a direct indication mentioned in the text.
- Option D (Arthroscopic meniscal repair of a posterior horn tear): While posterior horn meniscal tears are common, their repair is almost universally performed arthroscopically through standard anterior portals, sometimes with an accessory posteromedial or posterolateral portal, but not via a formal open posterior approach as described. The posterior approach is for deeper, more extensive posterior pathology or direct access to the PCL and vessels.
Question 33
When performing a posterior approach to the knee for a PCL avulsion, the surgeon makes a lazy S-shaped incision and identifies the neurovascular structures. Which of the following statements accurately describes the anatomical relationship of the major neurovascular structures in the popliteal fossa, as relevant to this approach?
Explanation
Correct Answer: C
The candidate's description of the posterior approach states: 'The small saphenous nerve is identified with accompanying sural nerve that must be preserved. The sural nerve is traced proximally where it pierces deep fascia from the tibial nerve trunk. At the apex of the fossa, the common peroneal nerve separates from tibial nerve. The tibial nerve lies posterior to the popliteal vein which in turn is superficial to popliteal artery.'
- Option A (The common peroneal nerve separates from the tibial nerve at the apex of the fossa and lies medial to the popliteal artery): The common peroneal nerve does separate at the apex, but it lies posterolaterally, not medial to the popliteal artery.
- Option B (The tibial nerve lies superficial to the popliteal vein, which is superficial to the popliteal artery): The text states, 'The tibial nerve lies posterior to the popliteal vein which in turn is superficial to popliteal artery.' This means the tibial nerve is most superficial (posterior), then the vein, then the artery (deepest/anterior). So, the tibial nerve is superficial to the vein, but the vein is superficial to the artery, making the overall statement incorrect in its sequence.
- Option C (The small saphenous nerve is identified with the accompanying sural nerve, which must be preserved): This is directly stated in the text: 'The small saphenous nerve is identified with accompanying sural nerve that must be preserved.'
- Option D (The popliteal artery is the most superficial structure, lying posterior to the popliteal vein and tibial nerve): This is incorrect. The popliteal artery is the deepest of the three main neurovascular structures (nerve, vein, artery) in the popliteal fossa. The tibial nerve is the most superficial.
- Option E (The common peroneal nerve is typically found posteromedially, while the tibial nerve is posterolaterally): This is incorrect. The common peroneal nerve is posterolateral, and the tibial nerve is posteromedial (and more central as it descends).
Question 34
A 30-year-old professional soccer player undergoes single-bundle ACL reconstruction for a right knee injury. To achieve optimal anatomical and isometric tunnel placement, where should the femoral tunnel ideally be positioned?
Explanation
Correct Answer: C
The candidate states: 'For the femoral tunnel the isometric point lies at about 10 to 10.30 o’clock for right knee and 1.30 to 2 for left knee. The anteromedial bundle is thought to be the most isometric but most surgeons feel that it’s important to replace the posterolateral bundle.' The question specifies a right knee and single-bundle reconstruction aiming for anatomical and isometric placement.
- Option A (At 12 o'clock, anterior to the resident's ridge): Placing the tunnel too anterior (e.g., 12 o'clock or anterior to the resident's ridge) is described as a common mistake that restricts knee flexion and may result in graft elongation.
- Option B (At 3 o'clock, in the intercondylar notch): This position is not described as optimal for a right knee ACL femoral tunnel.
- Option C (At 10 to 10:30 o'clock, targeting the posterolateral bundle footprint): This is the exact optimal position described for a right knee, with the aim of replacing the posterolateral bundle.
- Option D (At 1:30 to 2 o'clock, targeting the anteromedial bundle footprint): This position is described for a left knee, not a right knee. While the anteromedial bundle is isometric, the text states most surgeons aim to replace the posterolateral bundle.
- Option E (Posterior to the resident's ridge, at 7 o'clock): While avoiding the resident's ridge is important, placing the tunnel too posterior (e.g., 7 o'clock) results in excessive tightening of the graft when the knee is extended.
Question 35
A 28-year-old patient undergoes an arthroscopic single-bundle ACL reconstruction. Post-operatively, the patient complains of significant restriction in knee flexion, particularly beyond 90 degrees. Based on the principles discussed in the case, which of the following is the most likely technical error during the procedure?
Explanation
Correct Answer: D
The candidate explicitly states: 'The most common mistake is to place femoral tunnel too anterior or ‘resident’s ridge’. This restricts flexion of the knee and may result in elongation of graft.'
- Option A (Femoral tunnel placed too posterior): A femoral tunnel placed too posterior would result in excessive tightening of the graft when the knee is extended, not restricted flexion.
- Option B (Tibial tunnel placed too posterior): While tibial tunnel malpositioning can cause issues, the text specifically links restricted flexion to an anterior femoral tunnel. A too-posterior tibial tunnel might lead to impingement in flexion or extension, but the primary cause of restricted flexion is often an anterior femoral tunnel.
- Option C (Graft tensioned excessively in extension): While excessive tensioning can cause stiffness, the specific pattern of restricted flexion is most directly linked to an anterior femoral tunnel.
- Option E (Inadequate notchplasty leading to impingement in extension): Impingement from an inadequate notchplasty is mentioned, but the text links it to impingement on the lateral femoral condyle, and the specific complication of restricted flexion is attributed to an anterior femoral tunnel. Impingement in extension would typically be due to a too-anterior tibial tunnel or an inadequate notchplasty.
Question 36
A 35-year-old recreational athlete is considering ACL reconstruction. The surgeon discusses graft options, including bone-patella tendon-bone (BPTB) autograft. According to the case discussion, which of the following is a recognized disadvantage or donor site morbidity specifically associated with BPTB autografts?
Explanation
Correct Answer: D
The candidate discusses the disadvantages of BPTB grafts: 'However, it has donor site morbidity which includes anterior knee pain in 30–50%, patellar tendonitis 3–5%, patellar fracture and patella baja.'
- Option A (Slow healing due to tendon-to-bone incorporation): This is a disadvantage specifically associated with hamstring grafts, not BPTB grafts, which benefit from bone-to-bone healing.
- Option B (Increased risk of saphenous nerve injury): This is a potential complication associated with hamstring graft harvest, not BPTB.
- Option C (Higher incidence of hamstring weakness): This is a potential complication associated with hamstring graft harvest, not BPTB.
- Option E (Radiographic femoral tunnel widening): The text mentions 'increased knee laxity with radiographic femoral tunnel wide in hamstring graft,' indicating this is more associated with hamstring grafts.
Question 37
A 22-year-old patient undergoes ACL reconstruction using a four-strand hamstring autograft. Post-operatively, the patient reports numbness and altered sensation along the medial aspect of the leg, distal to the knee. Which nerve is most likely to have been injured during graft harvest?
Explanation
Correct Answer: D
The candidate states that a disadvantage of hamstring grafts is that 'It can also result in hamstring weakness and saphenous nerve injury.' The saphenous nerve provides sensory innervation to the medial aspect of the leg distal to the knee, making its injury consistent with the described symptoms.
- Option A (Common peroneal nerve): Injury to the common peroneal nerve would typically result in foot drop (weakness in dorsiflexion and eversion) and sensory loss over the dorsum of the foot and lateral leg, not the medial aspect of the leg.
- Option B (Tibial nerve): Injury to the tibial nerve would affect plantarflexion and toe flexion, with sensory loss over the sole of the foot.
- Option C (Sural nerve): The sural nerve provides sensation to the posterolateral aspect of the leg and lateral foot.
- Option E (Posterior femoral cutaneous nerve): This nerve provides sensation to the posterior thigh and upper calf, not the medial aspect of the distal leg.
Question 38
During an arthroscopic ACL reconstruction, after drilling the femoral tunnel in the anatomically correct position (10-10:30 o'clock for a right knee), the surgeon observes that the graft impinges against the anterior portion of the lateral femoral condyle when the knee is flexed. What is the most appropriate next step to address this issue?
Explanation
Correct Answer: B
The candidate discusses this exact scenario: 'Careful assessment of notch should be done prior to graft insertion using a pin to ensure no impingement on lateral femoral condyle. The presence of impingement with correct placement of tunnels necessitates notchplasty of the anterior portion of lateral femoral condyle.'
- Option A (Redrill the femoral tunnel in a more posterior position): The text explicitly states that the tunnel is already in the 'correct placement.' Redrilling it more posteriorly would lead to excessive tightening of the graft in extension, as mentioned in the case.
- Option C (Tension the graft less aggressively to avoid impingement): Graft tensioning is crucial for stability. Reducing tension to avoid impingement would compromise the stability of the reconstruction. The issue is mechanical impingement, not tension.
- Option D (Redrill the tibial tunnel in a more anterior position): This would likely exacerbate impingement or lead to other issues, as the problem is identified at the femoral side with the lateral femoral condyle.
- Option E (Proceed with graft fixation, as minor impingement is expected): Impingement, even if minor, can lead to graft wear, failure, and restricted range of motion. It should be addressed.
Question 39
A 20-year-old collegiate basketball player requires ACL reconstruction. The surgeon is comparing the use of a bone-patella tendon-bone (BPTB) autograft versus a four-strand hamstring autograft. According to the provided case discussion, which statement accurately reflects a key difference or outcome between these two graft types?
Explanation
Correct Answer: C
The candidate summarizes the comparison: 'Most studies show arthroscopic reconstruction with either graft results in similar functional outcome but increased morbidity in BPTB in form of early OA and increased knee laxity with radiographic femoral tunnel wide in hamstring graft.'
- Option A (BPTB grafts have slower integration due to tendon-to-bone healing compared to hamstring grafts): This is incorrect. BPTB grafts have faster integration due to bone-to-bone healing, while hamstring grafts have slower tendon-to-bone incorporation.
- Option B (Hamstring grafts are associated with a higher incidence of anterior knee pain compared to BPTB grafts): This is incorrect. Anterior knee pain (30-50%) is a significant donor site morbidity associated with BPTB grafts, not hamstring grafts.
- Option C (Most studies show BPTB grafts result in similar functional outcomes but increased donor site morbidity compared to hamstring grafts): This accurately reflects the summary provided by the candidate, noting similar functional outcomes but increased morbidity (e.g., anterior knee pain, patellar tendonitis) with BPTB.
- Option D (Hamstring grafts provide more rigid fixation and faster integration due to bone-to-bone healing): This is incorrect. BPTB grafts provide rigid fixation and faster integration due to bone-to-bone healing.
- Option E (BPTB grafts are associated with a higher risk of saphenous nerve injury during harvest): This is incorrect. Saphenous nerve injury is a risk associated with hamstring graft harvest.
Question 40
The case describes a 26-year-old rugby player with a displaced PCL avulsion fracture. The candidate proposes open reattachment. Considering the patient's age and activity level, what is the primary biomechanical advantage of open reattachment of a displaced bony PCL avulsion compared to a mid-substance PCL reconstruction?
Explanation
Correct Answer: C
While not explicitly stated as a direct comparison in the text, the underlying principle for choosing reattachment for an avulsion is the ability to restore the native anatomy and leverage bone-to-bone healing. The text implies this by stating the candidate would offer 'reattachment of the PCL avulsion through open procedure,' which is the standard of care for displaced bony avulsions in active patients. Bone-to-bone healing is generally more robust and faster than tendon-to-bone healing required for mid-substance reconstructions.
- Option A (Reduced risk of infection due to smaller incision): An open reattachment typically involves a larger incision than an arthroscopic reconstruction, so this is incorrect.
- Option B (Faster return to sport due to less invasive procedure): Open reattachment is generally more invasive than arthroscopic reconstruction, and recovery times can be similar or longer depending on the specific reconstruction technique.
- Option C (Superior bone-to-bone healing potential, restoring the native PCL footprint): This is the key advantage. Reattaching a bony fragment allows for bone-to-bone healing, which is biologically more favorable and provides a stronger initial fixation and faster healing compared to the tendon-to-bone healing required for a graft in a mid-substance reconstruction. It also directly restores the original PCL insertion site.
- Option D (Lower incidence of post-operative knee stiffness): Post-operative stiffness can occur with any knee surgery, and there's no inherent guarantee that reattachment leads to less stiffness than reconstruction.
- Option E (Elimination of donor site morbidity): While reattachment avoids the donor site morbidity associated with autografts used in reconstruction, it is not the primary biomechanical advantage. Furthermore, if an allograft is used for reconstruction, donor site morbidity is also avoided.
Question 41
A 22-year-old rugby player presents with a history of recurrent anterior shoulder instability. CT scan evaluation of the glenoid demonstrates a 25% anterior glenoid bone defect. Which of the following is the most appropriate definitive surgical management?
Explanation
Question 42
During a medial patellofemoral ligament (MPFL) reconstruction for recurrent patellar dislocation, identifying the correct femoral attachment site is critical to prevent abnormal joint kinematics. According to Schöttle's point, where is the anatomic femoral origin of the MPFL located?
Explanation
Question 43
A 35-year-old construction worker sustains a purely ligamentous Lisfranc injury after his foot gets trapped under a heavy object. Which of the following surgical treatments is associated with the best long-term functional outcomes and lowest reoperation rates for this specific injury pattern?
Explanation
Question 44
A 45-year-old cyclist falls directly onto his shoulder. Clinical examination reveals a prominent clavicle, and radiographs show an acromioclavicular (AC) joint dislocation with 150% superior displacement of the clavicle relative to the acromion. Which of the following describes the injured structures in a Type III AC separation?
Explanation
Question 45
A 50-year-old patient undergoes knee arthroscopy for a suspected medial meniscus injury. Intraoperatively, a complete radial tear at the posterior root of the medial meniscus is identified. Biomechanically, this injury is most equivalent to which of the following?
Explanation
Question 46
A 21-year-old elite collegiate basketball player sustains a fracture of the fifth metatarsal. Radiographs demonstrate a transverse fracture at the metaphyseal-diaphyseal junction. Which of the following is the most appropriate management for this specific patient?
Explanation
Question 47
A 68-year-old male presents with profound weakness in shoulder elevation and external rotation. MRI reveals a massive, retracted, and fatty-infiltrated tear of the supraspinatus and infraspinatus with an intact subscapularis and normal articular cartilage. He has active forward flexion to only 45 degrees but a negative hornblower's sign. Which of the following is the most appropriate surgical option?
Explanation
Question 48
A 9-year-old female soccer player sustains a mid-substance complete ACL rupture. She has wide-open physes with significant growth remaining. Which of the following surgical techniques is most appropriate to minimize the risk of growth arrest?
Explanation
Question 49
A 55-year-old diabetic patient presents with an erythematous, profoundly swollen, and warm right foot without open ulcerations. Radiographs demonstrate periarticular osteopenia and early fragmentation of the tarsal navicular. Systemic inflammatory markers are normal. What is the most appropriate initial management?
Explanation
Question 50
A 34-year-old male falls from his bicycle and sustains a completely displaced midshaft clavicle fracture. Which of the following radiographic findings is a universally accepted relative indication for open reduction and internal fixation?
Explanation
Question 51
A 28-year-old male sustains a high-energy knee dislocation (Schenck KD III). In the emergency department, his foot is pulseless. After prompt closed reduction of the knee, his dorsalis pedis pulse returns, but his Ankle-Brachial Index (ABI) is 0.8. What is the most critical next step in management?
Explanation
Question 52
When comparing operative versus nonoperative management of acute Achilles tendon ruptures, modern literature indicates which of the following regarding functional rehabilitation protocols?
Explanation
Question 53
A 30-year-old male weightlifter feels a pop in his anterior chest while performing a bench press. Examination reveals an asymmetric axillary fold and weakness with resisted adduction and internal rotation. Where does the pectoralis major most commonly tear in this mechanism?
Explanation
Question 54
A patient presents with lateral knee pain and a sensation of giving way following a hyperextension injury. Physical examination reveals a positive dial test with 15 degrees of increased external rotation at 30 degrees of knee flexion compared to the contralateral side. At 90 degrees of knee flexion, the external rotation is equal bilaterally. What is the most likely diagnosis?
Explanation
Question 55
A 45-year-old female presents with a painful bunion. Weight-bearing radiographs reveal a hallux valgus angle (HVA) of 45 degrees and an intermetatarsal angle (IMA) of 18 degrees. Clinical examination demonstrates significant hypermobility of the first tarsometatarsal (TMT) joint. Which surgical procedure is most appropriate?
Explanation
Question 56
A 65-year-old woman sustains a 3-part proximal humerus fracture.
Knowledge of the blood supply to the humeral head is critical for predicting the risk of avascular necrosis (AVN). Which vessel provides the primary blood supply to the articular segment of the humeral head?
Explanation
Question 57
During a posterior cruciate ligament (PCL) reconstruction, the surgeon must address the distinct functional bundles of the native PCL. Which of the following statements accurately describes the biomechanics of the PCL bundles?
Explanation
Question 58
A 25-year-old male is 4 months postoperative from open reduction and internal fixation of a Weber C ankle fracture with placement of two cortical syndesmotic screws. The patient is asymptomatic but inquires if the screws must be removed. Based on current orthopedic evidence, what is the best advice regarding routine syndesmotic screw removal?
Explanation
Question 59
A patient demonstrates a positive "lift-off" test and a positive "belly-press" test after a traumatic shoulder injury. These tests isolate the subscapularis muscle. Which of the following nerves supplies the isolated muscle?
Explanation
Question 60
A 22-year-old male presents with persistent knee pain 1 year after an injury. MRI and subsequent arthroscopy reveal a 3 cm x 3 cm isolated, full-thickness chondral defect (Outerbridge Grade IV) on the weight-bearing portion of the medial femoral condyle. The surrounding cartilage and menisci are normal. What is the most appropriate surgical treatment for a defect of this size?
Explanation
Question 61
A 22-year-old female soccer player sustains a non-contact twisting injury to her knee, feeling a "pop" and developing a rapid effusion. MRI confirms an acute anterior cruciate ligament (ACL) rupture. Which concomitant intra-articular injury is most commonly associated with this acute presentation?
Explanation
Question 62
A 30-year-old male is evaluated for knee instability following a motor vehicle accident. On physical examination, the dial test reveals 15 degrees of increased external rotation of the tibia at 30 degrees of knee flexion compared to the contralateral side. At 90 degrees of flexion, the external rotation is equal bilaterally. What is the most likely diagnosis?
Explanation
Question 63
A 35-year-old manual laborer presents with chronic, severe shoulder pain and weakness in external rotation. Imaging reveals a massive, retracted, and irreparable tear of the supraspinatus and infraspinatus with advanced fatty infiltration, but an intact subscapularis and teres minor. He has no significant glenohumeral arthritis. What is the most appropriate surgical intervention?
Explanation
Question 64
A 20-year-old collegiate rugby player presents with recurrent anterior shoulder instability. A pre-operative 3D CT scan demonstrates 27% anterior glenoid bone loss. Which of the following is the most appropriate definitive management?
Explanation
Question 65
A 24-year-old female presents with vague midfoot pain and swelling after forcefully plantarflexing her foot when stumbling on a stair. Non-weight-bearing radiographs appear entirely normal. If a subtle Lisfranc injury is suspected, what is the best next diagnostic step?
Explanation
Question 66
A 40-year-old male sustains an acute, closed midsubstance Achilles tendon rupture. When discussing operative repair versus functional non-operative management, the patient should be counseled that operative management is classically associated with:
Explanation
Question 67
A 16-year-old female presents with recurrent lateral patellar dislocations. You decide to surgically reconstruct the primary restraint to lateral patellar translation. Where is the normal anatomic femoral origin of this ligament located?
Explanation
Question 68
A 28-year-old recreational skier catches an edge and forcefully abducts his tibia. Clinical exam and MRI confirm an isolated, complete (Grade III) midsubstance tear of the medial collateral ligament (MCL). What is the standard of care for this injury?
Explanation
Question 69
A 55-year-old diabetic male with peripheral neuropathy presents with a deformed, painless, swollen foot. Radiographs display absorption of fine intra-articular debris, early fusion of large fracture fragments, and significant subchondral sclerosis. These findings correspond to which stage of the Eichenholtz classification for Charcot arthropathy?
Explanation
Question 70
A 33-year-old professional overhead laborer falls directly onto his acromion, sustaining an acromioclavicular (AC) joint injury. Radiographs show superior displacement of the clavicle by 150% compared to the acromion, with an increased coracoclavicular distance. What is the most appropriate management for this Type V AC joint injury?
Explanation
Question 71
During a Weber C ankle fracture, the distal tibiofibular syndesmosis is disrupted. Which of the following ligaments provides the greatest percentage of resistance against lateral displacement of the fibula?
Explanation
Question 72
A 10-year-old boy presents with a painful, snapping knee. MRI demonstrates a discoid lateral meniscus. In the Wrisberg variant of a discoid meniscus, which of the following normal anatomic attachments is absent?
Explanation
Question 73
A 24-year-old minor league baseball pitcher presents with vague, deep shoulder pain and clicking. MRI arthrogram shows a Type II Superior Labrum Anterior and Posterior (SLAP) tear. The "peel-back" mechanism precipitating this injury occurs maximally in which arm position during throwing?
Explanation
Question 74
A 45-year-old male with isolated medial compartment knee osteoarthritis and a varus mechanical axis is undergoing a medial opening-wedge high tibial osteotomy (HTO). To achieve optimal unloading, where should the weight-bearing line be transposed in the coronal plane?
Explanation
Question 75
A 40-year-old female presents with a painful bunion. Radiographs demonstrate a hallux valgus angle (HVA) of 26 degrees and an intermetatarsal angle (IMA) of 11 degrees. The first tarsometatarsal joint is stable without hypermobility. Which of the following is the most appropriate surgical option?
Explanation
Question 76
A 28-year-old male is brought to the trauma bay after a severe motorcycle accident. He has a clinically obvious knee dislocation that is quickly reduced. Post-reduction, his foot is warm with palpable pulses, but his Ankle-Brachial Index (ABI) is 0.85. What is the most appropriate next step in management?
Explanation
Question 77
A 68-year-old female presents with primary glenohumeral osteoarthritis. A CT scan of the shoulder reveals significant posterior glenoid wear, causing biconcavity and retroversion of the glenoid face. Based on the Walch classification, what type of glenoid morphology does she have?
Explanation
Question 78
A 30-year-old male sustains a severe hyperdorsiflexion injury to his foot during a fall from a height. Radiographs reveal a Hawkins Type III talar neck fracture. Which of the following accurately describes the associated displacement and the risk of avascular necrosis (AVN)?
Explanation
Question 79
What is the optimal knee flexion angle for tensioning a posterior cruciate ligament (PCL) graft during a single-bundle reconstruction?
Explanation
Question 80
A 72-year-old male undergoes a reverse total shoulder arthroplasty. At his 2-year follow-up, radiographs demonstrate inferior scapular notching. Which of the following surgical technique modifications during the index procedure would have most effectively reduced the risk of this complication?
Explanation
Question 81
When comparing functional rehabilitation following operative versus nonoperative treatment of acute Achilles tendon ruptures, nonoperative management combined with an early functional rehabilitation protocol has been shown to result in:
Explanation
Question 82
A 10-year-old male with wide-open physes sustains a complete mid-substance ACL tear. Which of the following surgical techniques has the lowest risk of iatrogenic growth disturbance?
Explanation
Question 83
A 24-year-old athlete sustains a midfoot injury. Weight-bearing radiographs show widening of the interval between the first and second metatarsal bases. The Lisfranc ligament connects which two structures?
Explanation
Question 84
A 22-year-old collegiate baseball pitcher presents with posterior shoulder pain during the late cocking phase of throwing. MRI arthrography reveals a Type II SLAP lesion. The pathogenesis of this specific injury is most commonly associated with:
Explanation
Question 85
A 32-year-old male sustains a Hawkins type III talar neck fracture following a motor vehicle collision. Which of the following indicates a positive Hawkins sign on a 6-week follow-up radiograph, and what does it signify?
Explanation
Question 86
A 55-year-old female presents with acute medial knee pain after a deep squat. MRI reveals a posterior root tear of the medial meniscus. If left untreated, this injury alters knee biomechanics most similarly to:
Explanation
None
