Medial Ankle and Deltoid Ligament Reconstruction: An Intraoperative Masterclass

Key Takeaway
This masterclass details medial ankle and deltoid ligament reconstruction. We cover comprehensive surgical anatomy, meticulous preoperative planning, and granular, real-time intraoperative execution. Learn precise techniques for acute and chronic ligament tears, including anchor placement and suture management. Gain insights into critical pearls, pitfalls, and comprehensive postoperative rehabilitation protocols for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater and this advanced didactic session. Today, we are undertaking a profound exploration of a complex, yet incredibly rewarding procedure: Medial Ankle and Deltoid Ligament Reconstruction. Historically, orthopedic literature and surgical practice have disproportionately focused on the lateral ligamentous complex, often relegating the medial side to an afterthought. However, modern biomechanical understanding dictates that this is not merely about fixing a localized tear; it is about restoring dynamic, multi-planar stability to a critical load-bearing joint. The ultimate goal is preventing devastating long-term sequelae such as progressive acquired flatfoot deformity, secondary posterior tibial tendon dysfunction (PTTD), and asymmetric tibiotalar arthrosis. Pay meticulous attention, as the intraoperative nuances and biomechanical principles discussed here dictate the difference between a resilient, functional joint and catastrophic construct failure.
Medial ankle instability is a notoriously underdiagnosed pathology, typically initiated by high-energy pronation (eversion) and external rotation injuries of the ankle joint complex. Envision the kinematics of a patient running downhill, landing awkwardly on an uneven, cambered surface, or a high-performance dancer executing a pirouette where the axial load rotates opposite to the planted foot's outward rotation. These specific mechanisms generate immense torque, leading to sequential, partial, or complete disruption of the superficial and deep bundles of the deltoid ligament. Unlike the lateral ligaments, which often fail in predictable, isolated patterns, the deltoid complex frequently undergoes interstitial tearing, plastic deformation, and chronic elongation before catastrophic rupture occurs.
A crucial historical detail to elicit during your clinical intake is the exact biomechanical mechanism of the index injury. Was there an outward rotation of the foot combined with an inward rotation of the tibia under axial load? This classic pronation-external rotation trauma often points directly to medial ligamentous compromise, even in the absence of a medial malleolar fracture. Chronic medial ankle instability is an insidious, progressive condition. Over time, the incessant valgus stress on the medial structures leads to secondary posterior tibial dysfunction, manifesting as tenosynovitis, elongation, or even complete rupture of the posterior tibial tendon. Conversely, primary posterior tibial tendon dysfunction can also overload the static deltoid ligaments, causing a step-by-step disruption and eventual complete medial column insufficiency.
Furthermore, we frequently encounter complete deltoid ligament ruptures in conjunction with lateral malleolar fractures, syndesmotic disruptions, or specific bimalleolar equivalent fracture patterns (e.g., the classic Weber B or C fracture with a widened medial clear space). The surgeon must always remain vigilant for this association; stabilizing the lateral column while ignoring an incompetent medial column will inevitably lead to a non-congruent mortise, altered contact mechanics, and rapid-onset post-traumatic osteoarthritis. The paradigm has shifted towards acute repair or reconstruction of the medial side in high-demand athletes and patients with profound instability, moving away from the historical reliance on lateral-sided fixation alone.


Detailed Surgical Anatomy and Biomechanics
Before a scalpel is ever passed, the orthopedic surgeon must possess an eidetic understanding of the medial ankle's surgical anatomy. The deltoid ligament is not a single, monolithic structure; it is a robust, highly sophisticated, multibanded complex that is absolutely crucial for medial ankle and hindfoot stability. It is functionally and anatomically divided into superficial and deep components, each possessing distinct osteological origins, insertions, and biomechanical responsibilities. Understanding this dual-layer concept is the foundation of anatomic reconstruction.
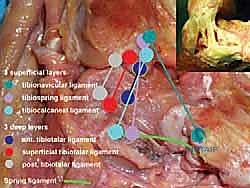
Superficial Components of the Deltoid Ligament
The superficial components of the deltoid ligament are unique in that they span two distinct articulations: the tibiotalar (ankle) and the talocalcaneonavicular (subtalar/transverse tarsal) joints. This bi-articular nature allows them to provide broad, sweeping stability to the medial column and the longitudinal arch. The complex is primarily composed of three distinct bands. First, the tibionavicular ligament originates from the anterior aspect of the anterior colliculus of the medial malleolus and inserts broadly onto the dorsal and medial aspect of the navicular bone. This band is a primary restraint to plantarflexion and external rotation.
Second, the tibiospring ligament is arguably the most critical of the superficial components for arch maintenance. It originates from the anterior colliculus and descends to blend intimately with the superomedial portion of the spring ligament complex (plantar calcaneonavicular ligament). This continuous fascial connection highlights its vital, synergistic role in supporting the talar head and maintaining the medial longitudinal arch; failure here is a hallmark of progressive flatfoot deformity. Third, the tibiocalcaneal ligament originates from the medial malleolus and descends almost vertically to insert onto the sustentaculum tali of the calcaneus, acting as a primary restraint to true hindfoot valgus.




Deep Components of the Deltoid Ligament
Beneath the sweeping superficial layer lie the deep components. These are shorter, vastly thicker, and significantly stronger bands that are strictly intra-articular (or capsular) and primarily stabilize the tibiotalar joint. The deep deltoid is the primary restraint to lateral translation and external rotation of the talus within the mortise. The anterior tibiotalar ligament originates from the anterior colliculus and inserts onto the medial talar body, just posterior to the articular surface of the talar head.
The posterior tibiotalar ligament is the most robust portion of the entire complex. It originates from the posterior colliculus of the medial malleolus and inserts broadly onto the medial tubercle of the posterior process of the talus. It is tensioned in dorsiflexion and is the ultimate backstop against anterior translation and internal rotation of the tibia on the talus. An intermediate tibiotalar ligament is frequently identified in cadaveric studies, acting as a transitional zone between the anterior and posterior deep fibers. Surgical reconstruction must account for these deep fibers; reconstructing only the superficial layer will leave the patient with persistent rotational instability of the talus.
Neurovascular and Musculotendinous Considerations
Approaching the medial ankle requires strict adherence to safe surgical intervals to avoid iatrogenic morbidity. Anteriorly, the Great Saphenous Vein and the Saphenous Nerve course directly over the anteromedial aspect of the joint. The saphenous nerve provides critical sensation to the medial aspect of the foot and ankle. Iatrogenic transection or entrapment in scar tissue can lead to debilitating, intractable neuropathic pain or painful neuromas that overshadow a successful ligament reconstruction. Our incisions must be meticulously planned and superficial dissection performed bluntly to mobilize and protect these structures.
Posteriorly, the Posterior Tibial Neurovascular Bundle resides within the tarsal tunnel, deep to the flexor retinaculum. While our primary incision is typically centered over the medial malleolus, aggressive posterior retraction or blind deep dissection must be rigorously avoided to protect the posterior tibial artery, the tibial nerve, and its accompanying venae comitantes. Furthermore, the Posterior Tibial Tendon (PTT) lies immediately posterior to the medial malleolus in the retromalleolar groove. As a key dynamic stabilizer of the medial arch, its integrity must be assessed during surgery. The PTT sheath is frequently thickened in chronic instability and can easily be mistaken for native deltoid ligamentous tissue by the unwary surgeon.



Exhaustive Indications and Contraindications
Patient selection is the cornerstone of successful medial ankle reconstruction. The diagnosis of medial ankle instability remains primarily clinical, built upon a foundation of thorough history-taking, detailed physical examination, and the judicious application of advanced imaging modalities. The ideal candidate is a patient with symptomatic, chronic medial ankle instability who has failed a comprehensive, supervised non-operative regimen (including medial posting orthotics, aggressive physical therapy focusing on invertor strengthening, and proprioceptive training) for a minimum of 3 to 6 months.
Surgical intervention is explicitly indicated in patients complaining of a persistent, debilitating sensation of "giving way," particularly localized to the medial aspect of the joint during activities involving uneven terrain, descending stairs, or pivoting. Furthermore, acute reconstruction is increasingly indicated in high-demand athletes presenting with a massive, acute deltoid rupture, particularly when associated with a syndesmotic injury or a rotational ankle fracture where the medial clear space cannot be anatomically reduced and maintained by lateral and syndesmotic fixation alone. Concomitant bony malalignment, such as a severe valgus hindfoot, is an absolute indication for combined procedures; performing a soft-tissue deltoid reconstruction in the presence of an uncorrected bony valgus thrust guarantees premature graft stretch-out and clinical failure.
Contraindications must be strictly respected to avoid catastrophic outcomes. Absolute contraindications include active, localized, or systemic infection, severe peripheral vascular disease precluding wound healing, and active Charcot neuropathic arthropathy. In a neuropathic joint, soft tissue reconstructions will inevitably fail due to the lack of protective proprioception; these patients require rigid osseous stabilization (arthrodesis). Relative contraindications include advanced patient age with low functional demands, morbid obesity (which places exponential stress on the reconstruction), uncontrolled diabetes mellitus, and severe, end-stage tibiotalar osteoarthritis. In the presence of advanced arthritis, a ligament reconstruction will not alleviate the primary source of pain, and an ankle arthrodesis or total ankle arthroplasty should be considered instead.
| Category | Specific Conditions | Rationale / Management Impact |
|---|---|---|
| Absolute Indications | Chronic symptomatic medial instability failing >6 months conservative care | Soft tissue integrity lost; requires anatomic reconstruction to restore kinematics. |
| Absolute Indications | Acute deltoid rupture with un-reducible medial clear space in fracture | Interposed ligament or massive instability preventing mortise congruence. |
| Relative Indications | Concomitant Stage II Adult Acquired Flatfoot Deformity (AAFD) | Deltoid repair must be combined with PTT debridement, FDL transfer, and calcaneal osteotomy. |
| Absolute Contraindications | Active Charcot Neuropathic Arthropathy | Lack of proprioception guarantees soft-tissue construct failure; requires fusion. |
| Absolute Contraindications | Active deep space infection or severe Peripheral Vascular Disease | Unacceptable risk of wound necrosis, deep infection, or amputation. |
| Relative Contraindications | End-stage Tibiotalar Osteoarthritis (Kellgren-Lawrence Grade IV) | Restoring stability will not cure arthritic pain; arthrodesis or arthroplasty indicated. |




Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is non-negotiable. The clinical examination should have already quantified the degree of instability. The Anterior Drawer Test, performed with the foot in slight plantarflexion, assesses the anterior deep deltoid and anterior talofibular ligament. The Eversion Stress Test, stabilizing the distal tibia and applying valgus stress to the hindfoot, is pathognomonic for deltoid incompetence when excessive medial gapping is palpated compared to the contralateral limb. Furthermore, the single-leg heel rise test must be evaluated to ensure the posterior tibial tendon is functional and capable of locking the transverse tarsal joint.
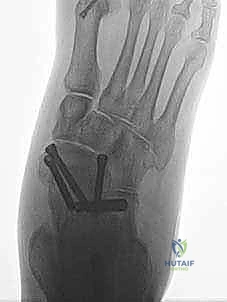
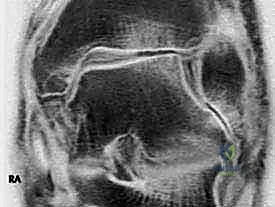
Imaging is a crucial adjunct to clinical assessment. Standard weight-bearing plain radiographs (AP, lateral, and mortise views) are mandatory. The surgeon must meticulously evaluate for medial clear space widening (>4mm is highly suspicious for deep deltoid incompetence), talar tilt, and secondary foot deformities such as valgus heel malalignment or talonavicular joint unroofing. Magnetic Resonance Imaging (MRI) is the gold standard for soft tissue evaluation. T2-weighted fat-suppressed sequences are excellent for identifying acute edema, partial tears, or interstitial stripping of the deltoid complex from the medial malleolus. T1-weighted images are critical for assessing the chronicity of the injury, visualizing scar tissue, and evaluating the structural integrity of the posterior tibial tendon and spring ligament complex.
Templating and Graft Selection
Once the diagnosis is confirmed, templating and surgical strategy must be finalized. If the MRI indicates a robust but avulsed native ligament, primary repair with suture anchors (often augmented with internal bracing) is planned. However, in cases of chronic, attenuated insufficiency where the native tissue is biologically inadequate, an autograft or allograft reconstruction is required. The surgeon must decide between a free tendon graft (e.g., semitendinosus, gracilis, or plantaris) or utilizing a local tendon transfer. Preoperative templating involves estimating the required graft length and determining the optimal trajectory for bone tunnels in the medial malleolus, talus, and potentially the navicular or calcaneus, depending on the specific bundles being reconstructed.
Operating Room Setup and Positioning
The patient is brought to the operating theater and placed in the supine position on a standard radiolucent operating table. A bump (typically a rolled blanket or sandbag) is placed under the ipsilateral hip. This is a critical step; it internally rotates the leg, bringing the naturally externally rotated lower extremity into a neutral position, thereby allowing simultaneous access to both the medial and lateral aspects of the ankle if a combined procedure (e.g., lateral ligament repair or syndesmotic stabilization) is required. A well-padded pneumatic tourniquet is applied to the proximal thigh. The entire lower extremity is prepped and draped in a standard sterile fashion, ensuring the knee is free to allow for assessment of rotational alignment. Intraoperative fluoroscopy (C-arm) must be positioned to enter from the contralateral side, ensuring unencumbered orthogonal views of the ankle mortise throughout the procedure.





Step-by-Step Surgical Approach and Fixation Technique
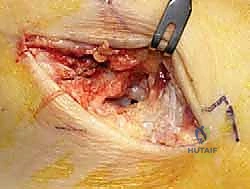
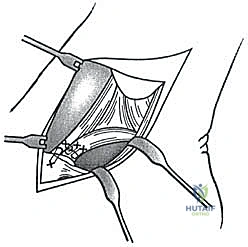
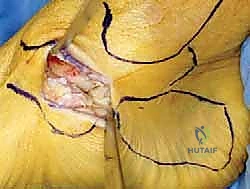
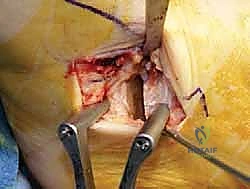
The surgical execution demands precision, respect for soft tissue envelopes, and rigid adherence to biomechanical principles. Following exsanguination and tourniquet inflation, a curvilinear incision is made over the medial aspect of the ankle. The incision typically begins 2-3 centimeters proximal to the tip of the medial malleolus, curving distally and slightly anteriorly toward the navicular tuberosity. This approach provides excellent exposure of both the medial malleolus and the talonavicular joint.
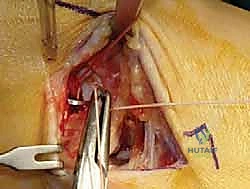
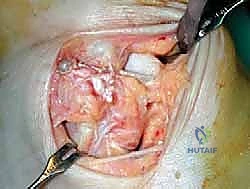
Superficial Dissection and Joint Preparation
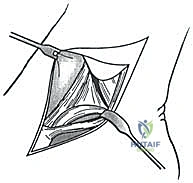
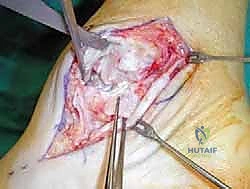
Subcutaneous dissection must be performed with meticulous care using blunt retractors and careful hemostasis. The great saphenous vein and the saphenous nerve are identified in the anterior flap, mobilized together, and gently retracted anteriorly to prevent traction neurapraxia. The deep crural fascia is then incised in line with the skin incision. The surgeon must now identify the remnants of the deltoid ligament. In chronic cases, this is often a thickened, disorganized mass of scar tissue. The posterior tibial tendon sheath is identified at the posterior margin of the wound and left intact unless concomitant PTT pathology dictates exploration.
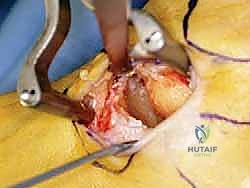
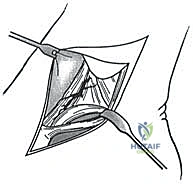
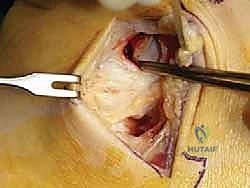
An anteromedial arthrotomy is performed to inspect the tibiotalar joint. This is a critical step to address any intra-articular pathology. The medial gutter is thoroughly debrided of hypertrophic synovitis, scar tissue, and any loose osteochondral fragments that may have resulted from chronic talar impingement. The medial articular surface of the talus and the tibial plafond are inspected for osteochondral lesions. Once the joint is cleared, the anatomical footprints of the superficial and deep deltoid ligaments on the medial malleolus and the medial aspect of the talus are identified and decorticated with a curette or a motorized burr to expose bleeding subchondral bone, optimizing the biological environment for ligament-to-bone healing.
Graft Preparation and Tunnel Placement
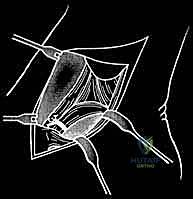
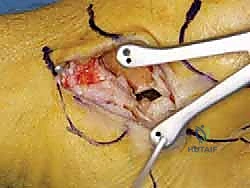
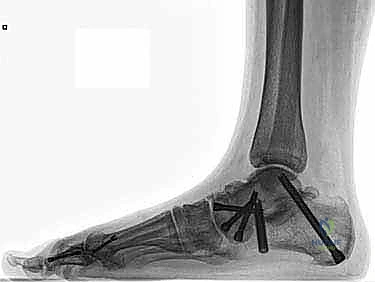
If an anatomic reconstruction utilizing a tendon graft is planned, the graft (e.g., a semitendinosus allograft) is prepared on the back table. The ends are whipstitched with high-strength non-absorbable suture. Attention is then turned to bone tunnel creation. For a comprehensive reconstruction addressing both deep and superficial layers, a tunnel is drilled into the medial body of the talus, corresponding to the insertion of the deep anterior tibiotalar ligament. A second tunnel or anchor point is established on the navicular tuberosity or sustentaculum tali, depending on the specific superficial bands being recreated.
The medial malleolar tunnel is the keystone of the construct. A guide pin is placed starting at the anatomic origin of the deltoid complex (between the anterior and posterior colliculi) and directed proximally and laterally to exit the lateral tibial cortex. A cannulated drill is used to create a socket of appropriate depth and diameter to accommodate the graft. It is imperative that the osseous tunnels are placed precisely at the isometric points of the native ligaments; non-isometric placement will result in either graft laxity in certain ranges of motion or restricted joint mobility and premature graft failure.
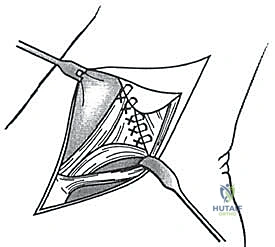
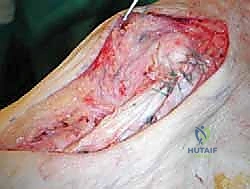
Construct Tensioning and Fixation
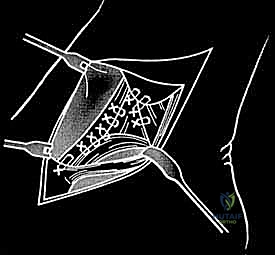
The graft is first secured within the talar tunnel using a bio-tenodesis screw or a solid cortical anchor. The superficial limb of the graft is similarly secured to the navicular or calcaneus. The free ends of the graft are then passed into the medial malleolar socket. Tensioning the construct is the most technically demanding aspect of the procedure. The ankle is held in neutral dorsiflexion and slight inversion. This position reduces the talus anatomically within the mortise and closes the medial clear space.
While holding this precise reduction, maximum manual tension is applied to the graft limbs, and a bio-interference screw is advanced into the medial malleolar tunnel, achieving rigid aperture fixation. If a primary repair with internal bracing is utilized instead of a graft, high-strength suture tape is passed from talar and navicular anchors up to a swivel-lock anchor in the medial malleolus, tensioned in the exact same biomechanical position. Following fixation, the ankle is put through a full range of motion. The surgeon must visually and fluoroscopically confirm that the medial clear space remains symmetric throughout the arc of motion, without restricting physiological dorsiflexion or plantarflexion. The arthrotomy and retinacular layers are meticulously closed, followed by standard layered skin closure.



Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following medial ankle reconstruction can and do occur. The surgeon must be prepared to identify and manage these effectively. The most common intraoperative error is non-anatomic tunnel placement or inappropriate tensioning. Over-tightening the construct, particularly in excessive inversion or plantarflexion, will result in a severely restricted range of motion, chronic medial ankle pain, and altered gait mechanics. Conversely, under-tightening or failing to address the deep deltoid components will lead to recurrent valgus instability, persistent talar tilt, and eventual failure of the superficial reconstruction.
Neurologic complications are a significant source of postoperative morbidity. The saphenous nerve is highly vulnerable during the superficial dissection. Traction neurapraxia usually resolves with conservative management and time, but direct transection or entrapment in the surgical scar can lead to a painful neuroma or Complex Regional Pain Syndrome (CRPS). Incidence rates for transient saphenous neuritis range from 5% to 15% in the literature. Management of a confirmed neuroma may require surgical excision and burying the proximal nerve stump deep into muscle belly to prevent recurrent surface irritation.
Hardware-related complications include anchor pullout, particularly in osteoporotic bone, or prominent hardware causing soft tissue irritation. Biological failures, such as graft stretching, rupture, or ongoing progression of an undiagnosed posterior tibial tendon dysfunction, can lead to recurrent instability. Infection, while rare (<2%), is a devastating complication in any intra-articular procedure and requires aggressive irrigation, debridement, and appropriate intravenous antibiotic therapy.
Salvage Procedures
When a primary medial ankle reconstruction fails, salvage options become increasingly complex. If the failure is due to isolated graft stretch-out but the joint remains completely congruent without arthritic changes, a revision reconstruction using a more robust allograft and augmented fixation techniques (e.g., adding an internal brace or utilizing suspensory cortical buttons) may be attempted. However, if recurrent instability is accompanied by significant uncorrected bony deformity (e.g., severe pes planovalgus), revision soft-tissue surgery must be combined with corrective osteotomies (e.g., medializing calcaneal osteotomy, Cotton osteotomy). In end-stage scenarios where chronic instability has led to severe, irreversible tibiotalar or subtalar osteoarthritis, soft-tissue reconstruction is no longer viable. The definitive salvage procedure in these cases is an ankle arthrodesis or a triple arthrodesis to provide a stable, plantigrade, and pain-free foot.
| Complication Type | Estimated Incidence | Prevention & Salvage Management |
|---|---|---|
| Saphenous Nerve Injury | 5% - 15% | Prevention: Careful blunt dissection, avoid aggressive anterior retraction. Salvage: Gabapentinoids, nerve blocks; surgical neuroma excision and deep burial if intractable. |
| Recurrent Instability / Graft Failure | 5% - 10% | Prevention: Anatomic tunnel placement, correct tensioning in neutral, address bony valgus. Salvage: Revision reconstruction with allograft/internal bracing; consider corrective osteotomies. |
| Joint Stiffness / Over-constriction | 10% - 20% | Prevention: Tension graft strictly in neutral dorsiflexion, avoid excessive inversion. Salvage: Aggressive physical therapy; rarely requires arthroscopic or open release of the construct. |
| Deep Infection | < 2% | Prevention: Strict sterile technique, prophylactic antibiotics, optimize host factors. Salvage: Immediate operative I&D, hardware removal if loose, targeted IV antibiotics. |