Limb Lengthening Masterclass: Ilizarov and Monoplanar Fixator Techniques
Key Takeaway
Welcome, fellows, to an immersive masterclass in limb lengthening. We'll meticulously cover Ilizarov and monoplanar fixator techniques, from comprehensive surgical anatomy and precise preoperative planning to granular, real-time intraoperative execution. Learn critical pearls, avoid common pitfalls, and master postoperative complication management for optimal patient outcomes in limb length discrepancy correction.
Comprehensive Introduction and Patho-Epidemiology
Limb lengthening and complex deformity correction represent a pinnacle of reconstructive orthopedic surgery, demanding an exhaustive understanding of bone biology, soft tissue dynamics, and intricate biomechanics. At the core of this discipline is the biological phenomenon of distraction osteogenesis (DO), a concept revolutionized by Gavriil A. Ilizarov in Kurgan, Russia, during the mid-20th century. Ilizarov elucidated the "law of tension-stress," demonstrating that gradual, controlled traction applied to living tissues creates a state of metabolic activation. This mechanical stimulus drives the proliferation and differentiation of pluripotential stem cells, resulting in the genesis of new bone, skin, muscle, nerves, and blood vessels. The biological cascade initiated by DO is essentially a highly orchestrated recapitulation of embryonic intramembranous ossification, bypassing the cartilaginous intermediate phase characteristic of endochondral fracture healing, provided that the mechanical environment remains optimally stable.
The pathogenesis of limb length discrepancy (LLD) and associated angular deformities is broadly categorized into congenital, developmental, and acquired etiologies. Congenital deficiencies, such as proximal focal femoral deficiency (PFFD), fibular hemimelia, and tibial hemimelia, present formidable reconstructive challenges. These conditions are rarely isolated linear discrepancies; they are typically accompanied by severe soft tissue contractures, joint instability, and multiplanar osseous deformities. Developmental etiologies include skeletal dysplasias (e.g., achondroplasia, pseudoachondroplasia) and metabolic bone diseases, which often result in bilateral, symmetric shortening but may develop asymmetric bowing requiring complex spatial correction. Acquired LLD frequently stems from pediatric physeal trauma, where partial or complete premature growth arrest leads to progressive shortening and angular deviation as the patient matures.
Furthermore, the epidemiology of acquired limb deformities encompasses a significant volume of post-traumatic malunions, nonunions, and chronic osteomyelitis in the adult population. High-energy trauma, particularly open tibial fractures, often results in segmental bone loss. Traditional management with massive autogenous bone grafting or vascularized fibular transfers carries significant donor site morbidity and variable success rates. The Ilizarov method, utilizing bone transport via DO, offers a paradigm-shifting alternative. By resecting the infected or necrotic bone segment and performing a remote metaphyseal corticotomy, surgeons can transport a healthy segment of bone intercalary to bridge the defect, simultaneously eradicating infection and restoring limb length.
The physiological demand of limb lengthening on the patient cannot be overstated. The regenerate bone forms in a highly vascularized, longitudinally oriented fibrovascular bridge. The success of this bridge maturing into robust cortical bone is entirely dependent on the preservation of the periosteal and endosteal blood supply during the initial corticotomy, followed by a strict adherence to the latency period (typically 5 to 10 days) before distraction commences. Disruption of this delicate biological sequence—whether through thermal necrosis during osteotomy, an excessively rapid distraction rate, or inadequate fixator stability—inevitably leads to catastrophic complications such as fibrous nonunion or premature consolidation.
Biological Phases of Distraction Osteogenesis
The process of DO is rigidly divided into three distinct clinical and biological phases: latency, distraction, and consolidation. The latency phase represents the period immediately following the corticotomy, during which a standard fracture hematoma forms, and the initial inflammatory cascade recruits mesenchymal stem cells. This period is critical for the establishment of a preliminary fibrovascular network. Skipping the latency phase severely compromises the osteogenic potential of the regenerate, often leading to atrophic nonunion. Conversely, an excessively prolonged latency phase, particularly in pediatric patients with robust healing potential, risks premature consolidation of the corticotomy site, necessitating a secondary surgical intervention.
The distraction phase is characterized by the application of gradual, relentless tension across the osteotomy site. The universally accepted optimal rate of distraction is approximately 1.0 mm per day, meticulously divided into four increments of 0.25 mm. This rhythm and rate maintain the pluripotential cells in a state of continuous proliferation, preventing terminal differentiation into mature osteoblasts until the desired length is achieved. The microscopic environment during this phase reveals a central radiolucent "fibrous interzone" flanked by highly organized, longitudinally oriented columns of primary woven bone extending from the proximal and distal host bone surfaces.
Once the target length or deformity correction is achieved, the consolidation phase begins. The external fixator is locked, transitioning the mechanical environment from dynamic tension to static stability, which allows the central fibrous interzone to ossify. The primary woven bone undergoes extensive remodeling under the influence of functional weight-bearing, eventually transforming into mature lamellar bone with a reconstituted medullary canal. This phase is notoriously prolonged, often taking twice as long as the distraction phase. The "healing index," defined as the total time in the external fixator divided by the length of regenerate gained (months/cm), is a critical metric; a typical healing index ranges from 1.0 to 2.0 months/cm, heavily influenced by patient age, etiology, and the anatomical site of lengthening.

Detailed Surgical Anatomy and Biomechanics
The application of an Ilizarov or monoplanar external fixator requires an intimate, cross-sectional mastery of regional anatomy. The surgeon is essentially driving rigid metal pins and highly tensioned wires blindly through the limb, relying entirely on anatomical landmarks and "safe corridors" to avoid catastrophic neurovascular injury. In the tibia, the cross-sectional anatomy dictates specific wire trajectories. The anterior compartment, housing the anterior tibial artery and deep peroneal nerve, is highly vulnerable during anterior half-pin placement. The lateral compartment contains the superficial peroneal nerve, which becomes increasingly anterior as it descends the leg, crossing the planned path of lateral-to-medial transfixation wires.
The proximal tibia is the most common site for corticotomy due to its expansive metaphyseal cross-section and robust vascularity. Here, the safe zone for transfixation wires is primarily transverse, avoiding the common peroneal nerve as it wraps around the fibular neck laterally, and the popliteal artery as it bifurcates posteriorly. When addressing the femur, the anatomical constraints become even more severe due to the massive muscular envelope and deep neurovascular structures. The femoral artery and vein traverse the adductor canal medially, while the sciatic nerve courses posteriorly. Consequently, femoral fixation relies heavily on lateral and anterolateral half-pins, as true transfixation wires are frequently precluded by the risk of tethering the quadriceps mechanism or impaling major vessels.
Biomechanics of Circular vs. Monoplanar Fixation
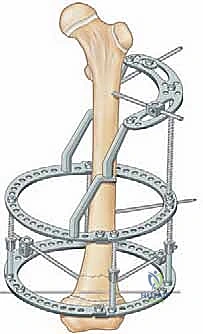
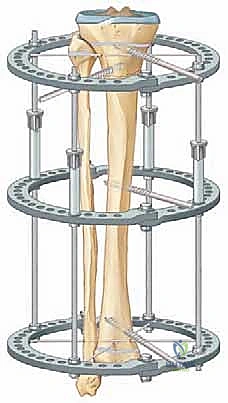
The biomechanical superiority of the Ilizarov circular fixator lies in its utilization of highly tensioned, small-diameter (1.5 mm or 1.8 mm) smooth wires. When tensioned to 100-130 kg, these wires exhibit non-linear stiffness; they provide absolute rigidity against axial torsion and bending, yet allow a microscopic degree of axial micromotion under physiological weight-bearing. This axial dynamization is the absolute catalyst for robust regenerate formation. The stability of the circular construct is governed by several critical variables: ring diameter (smaller rings closer to the skin increase stability), wire crossing angles (an ideal orthogonal 90-degree crossing maximizes multiplanar stability, though anatomical constraints often limit this to 60 degrees), and the distance between the rings (a wider span across the bone segment increases the lever arm and overall construct rigidity).
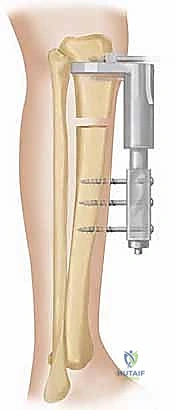
Monoplanar fixators, conversely, rely on the cantilever bending stiffness of large-diameter (4.5 mm to 6.0 mm) half-pins anchored into the near and far cortices of the bone, connected to a rigid external rail. While technically less demanding to apply and often better tolerated by patients due to reduced bulk, monoplanar devices are biomechanically inferior for complex multiplanar deformities. They are inherently asymmetric, meaning the mechanical axis of the fixator is offset from the mechanical axis of the bone. This offset creates bending moments during distraction, which predictably pull the bone into varus or valgus depending on the pin placement. Therefore, monoplanar fixators are strictly indicated for simple, single-plane lengthening (e.g., pure LLD without angular deformity) or in specific anatomical regions like the femur where a full circular frame is poorly tolerated.
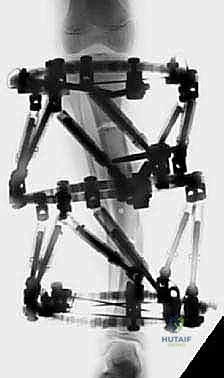
To mitigate the inherent biomechanical limitations of external fixation, modern techniques frequently employ hybrid constructs. These combine the rigid half-pin fixation of monoplanar systems in the diaphyseal regions with the tensioned-wire multiplanar control of circular rings in the metaphyseal regions. Furthermore, the advent of hexapod circular fixators (e.g., Taylor Spatial Frame) has revolutionized the biomechanical application of Ilizarov principles. Hexapod frames utilize a Stewart platform configuration, allowing simultaneous correction of six degrees of freedom (angulation and translation in all three planes) via a computerized algorithm, drastically reducing the need for complex, mid-treatment frame modifications.
Exhaustive Indications and Contraindications
The decision to embark on a limb lengthening or complex deformity correction utilizing distraction osteogenesis is one of the most consequential in orthopedic surgery. The indications are broad but must be carefully weighed against the immense psychological and physiological toll the procedure exacts on the patient. Primary indications include significant congenital limb length discrepancies (typically those projected to exceed 3-4 cm at skeletal maturity), where non-operative management via shoe lifts becomes functionally prohibitive and cosmetically unacceptable. In the pediatric population, conditions such as hemihypertrophy, Ollier's disease, and multiple hereditary exostoses frequently necessitate multi-staged lengthening procedures throughout the child's growth.
In adult reconstructive orthopedics, the indications shift heavily toward post-traumatic salvage. Infected nonunions with segmental bone loss represent a classic indication for the Ilizarov bone transport technique. Traditional grafting techniques fail dismally in the presence of active osteomyelitis; however, DO allows for the radical debridement of infected, avascular bone followed by the transport of a pristine, highly vascularized osseous segment to obliterate the defect. Additional adult indications include the correction of severe malunions that alter joint mechanics and precipitate early-onset osteoarthritis, as well as the treatment of complex foot and ankle deformities (e.g., severe equinocavovarus) where acute correction would result in devastating neurovascular compromise or skin necrosis.

Contraindications, while relatively few, are absolute when present. Severe psychiatric illness, non-compliance, or lack of a robust psychosocial support system are absolute contraindications. The patient must be capable of adhering to a rigorous daily protocol of pin-site care, precise fixator adjustments, and aggressive physical therapy; failure in any of these areas guarantees a catastrophic outcome. Furthermore, severe vascular insufficiency represents a biological absolute contraindication. Distraction osteogenesis is a highly metabolic process requiring immense local blood flow; attempting to lengthen an ischemic limb will inevitably result in soft tissue necrosis, nonunion, and potentially amputation.
| Category | Specific Conditions / Factors | Rationale for Indication or Contraindication |
|---|---|---|
| Absolute Indications | Infected Nonunions with Bone Loss | DO allows radical debridement and intercalary transport, simultaneously curing infection and restoring length. |
| Severe Congenital LLD (>4 cm) | Corrects disabling pelvic obliquity and gait pathology that orthotics cannot adequately address. | |
| Multiplanar Malunions | Hexapod/Ilizarov frames allow simultaneous correction of angulation, rotation, and translation. | |
| Relative Indications | Aesthetic Stature Lengthening | Highly controversial; carries immense risk for purely cosmetic gain, though increasingly performed in specialized centers. |
| Moderate LLD (2-4 cm) | May be treated with epiphysiodesis in growing children or shoe lifts; lengthening is an option but risks must be weighed. | |
| Absolute Contraindications | Severe Peripheral Vascular Disease | Ischemic tissues cannot support the massive metabolic demand of regenerate bone formation. |
| Untreated Systemic Sepsis | Active systemic infection must be controlled prior to elective frame application. | |
| Severe Psychiatric Non-Compliance | Inability to perform pin care, adjust struts, or attend PT leads to guaranteed failure and severe morbidity. |

Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning is the absolute bedrock of successful deformity correction. The surgeon must transition from a qualitative assessment to a highly precise, quantitative geometric analysis of the deformity. This begins with the acquisition of pristine, full-length, weight-bearing, hip-to-ankle radiographs. The patient must be positioned with the patellae facing strictly forward to eliminate rotational artifact, and a leveling block must be placed under the short limb to level the pelvis. From these radiographs, the Mechanical Axis Deviation (MAD) is calculated. The mechanical axis of the lower extremity normally passes from the center of the femoral head, through the center of the knee joint, to the center of the ankle mortise. Any deviation of this line from the center of the knee indicates a structural deformity requiring correction.
The core of modern pre-operative templating relies on the Center of Rotation of Angulation (CORA) methodology, popularized by Dror Paley. By drawing the anatomical or mechanical axes of the proximal and distal bone segments, the intersection point defines the CORA. The surgeon must then apply the three osteotomy rules. Rule 1: If the osteotomy and the mechanical hinge of the fixator are both placed exactly at the CORA, the deformity will correct without translation. Rule 2: If the osteotomy is placed away from the CORA, but the hinge remains at the CORA, the deformity will correct, but the bone ends will translate (often a desirable effect to maintain bone contact in complex deformities). Rule 3: If the hinge and osteotomy are placed away from the CORA, a secondary translation deformity will be inadvertently created.

Advanced imaging, particularly CT scanograms, is mandatory when severe joint contractures preclude true standing radiographs. CT allows for the highly accurate measurement of torsional deformities (e.g., femoral anteversion, tibial torsion) by superimposing axial cuts of the proximal and distal articular surfaces. In the era of computerized hexapod frames, pre-operative planning also involves software templating. The surgeon inputs specific radiographic parameters (mounting parameters, deformity parameters, and frame parameters) into the software, which then generates a precise daily strut adjustment schedule for the patient.
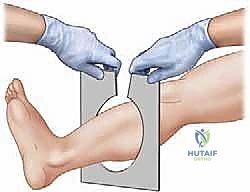
Patient positioning in the operating room must facilitate unhindered fluoroscopic access from the hip to the ankle in both orthogonal planes. A completely radiolucent Jackson table or a standard table with a radiolucent extension is required. For lower extremity procedures, a bump is placed under the ipsilateral hip to internally rotate the leg to a neutral position. The entire limb is prepped and draped free, allowing the surgeon to manipulate the joints and visually assess alignment throughout the procedure. The C-arm must be positioned to allow rapid transition between AP and lateral views without compromising the sterile field or striking the bulky external fixator.

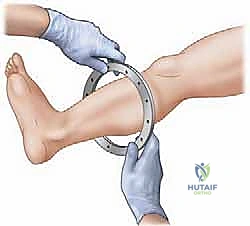
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of an Ilizarov application demands meticulous attention to detail; minor technical errors in pin placement or corticotomy execution compound into major clinical failures. The procedure begins with the pre-assembly of the external fixator frame based on the pre-operative templating. While some surgeons prefer to build the frame intra-operatively "on the leg," pre-assembly significantly reduces tourniquet time and ensures optimal ring sizing and alignment. The frame is slid onto the limb, and the reference wire—typically a transverse wire placed parallel to the joint line in the metaphyseal block—is inserted. This first wire dictates the alignment of the entire construct and must be perfectly parallel to the mechanical axis of the joint in the coronal plane.
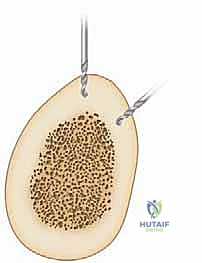
Wire insertion technique is critical to prevent thermal necrosis of the bone and subsequent ring sequestrum or pin-site infection. Wires must never be drilled continuously through the bone. The surgeon should push the wire through the near soft tissues to the bone cortex, drill through the near cortex, gently tap the wire across the medullary canal to preserve endosteal vessels, drill through the far cortex, and finally tap the wire out through the far soft tissues. Once the wire exits the skin, it is secured to the ring and tensioned to 100-130 kg using a dedicated dynamometer. Olive wires—wires with a small metal bead—are strategically utilized to compress bone fragments or prevent translation of the bone along the wire during complex deformity correction.

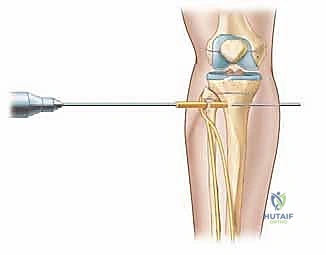
The Atraumatic Corticotomy
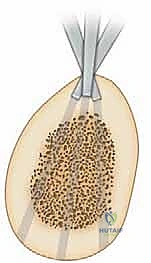
The corticotomy is the most critical biological step of the operation. It must not be confused with a standard osteotomy; the goal is to divide the rigid cortical bone while maximally preserving the periosteal sleeve and, if possible, the medullary blood supply. The approach is typically made through a minimal 1-2 cm incision over the subcutaneous border of the bone (e.g., the anterior medial face of the tibia). The periosteum is meticulously incised and elevated circumferentially. A multiple drill-hole technique is highly recommended. A 4.8 mm or 3.2 mm drill bit is used to create a series of contiguous holes across the near, medial, and lateral cortices, taking extreme care not to plunge into the posterior neurovascular structures.
Following the drilling, a sharp, thin osteotome is introduced into the drill holes. The osteotome is not driven straight through the bone; rather, it is gently twisted to crack the remaining cortical bridges—a technique known as osteotome clasis. The posterior cortex is often the most difficult to safely divide. Once the cortices are cracked, the surgeon manually rotates the bone fragments to ensure a complete circumferential break. An audible "crack" and the sudden ability to freely rotate the proximal and distal segments confirm completion. The bone fragments are then immediately apposed to their anatomic position to tamponade bleeding and initiate the latency phase hematoma.

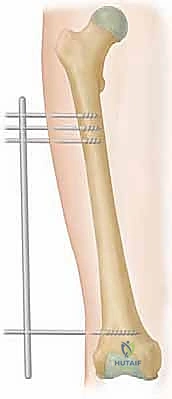
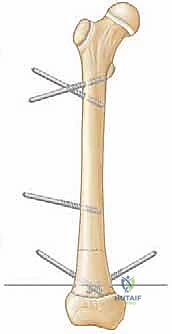
For monoplanar fixator application, the principles remain similar, but the execution relies on half-pins. Hydroxyapatite (HA)-coated half-pins are strongly recommended for diaphyseal fixation, as they significantly increase the bone-pin interface extraction torque and drastically reduce the incidence of aseptic loosening and pin-site infections. The pins must be placed strictly in the mid-sagittal or mid-coronal planes to minimize asymmetric bending forces during distraction. Pre-drilling with a sharp bit and utilizing a tissue protection sleeve are absolute mandates to prevent soft tissue necrosis around the pin shank.

Complications, Incidence Rates, and Salvage Management
Limb lengthening is fraught with complications; it is universally acknowledged that every patient undergoing massive lengthening will experience at least one complication during their treatment course. Dror Paley famously categorized these into "problems" (requiring non-operative intervention, e.g., minor pin tract infection), "obstacles" (requiring operative intervention but not affecting the final outcome, e.g., premature consolidation requiring re-corticotomy), and "true complications" (permanent sequelae affecting the final outcome, e.g., permanent nerve injury or nonunion). The incidence of pin-site infections approaches 100% in lengthy treatments, though the vast majority are superficial and rapidly resolve with oral antibiotics and aggressive local pin care.
Joint contractures represent the most insidious and common obstacle during limb lengthening. As the bone is distracted, the surrounding musculotendinous units resist elongation, creating massive tension across adjacent joints. In tibial lengthening, the gastrocnemius-soleus complex inevitably tightens, leading to a progressive equinus contracture of the ankle. If left unchecked, this forces the foot into a rigid plantarflexed position, making weight-bearing impossible and potentially leading to anterior subluxation of the talus. Salvage management requires immediate cessation of distraction, aggressive physical therapy, dynamic splinting, and frequently, operative intervention such as a percutaneous Achilles tendon lengthening (TAL) or the extension of the Ilizarov frame across the ankle joint to mechanically force dorsiflexion.

Axial deviation of the regenerate is another frequent complication, occurring in up to 30% of cases, particularly with monoplanar fixators. The soft tissue tension invariably pulls the bone fragments toward the strongest muscle groups—resulting in varus and procurvatum in the femur, and valgus and procurvatum in the tibia. If utilizing a circular frame, this deviation can be dynamically corrected by adjusting the hinges and struts. However, in monoplanar systems, significant axial deviation often requires a return to the operating room to revise the pin placement or exchange the frame entirely.
| Complication Type | Estimated Incidence | Pathophysiology & Presentation | Salvage / Management Strategy |
|---|---|---|---|
| Pin-Site Infection | 80% - 100% | Bacterial colonization (Staph aureus) at skin-metal interface. Erythema, drainage, pain. | Grade 1-2: Oral antibiotics, aggressive cleaning. Grade 3-4: Pin removal/exchange, IV antibiotics, debridement. |
| Joint Contracture (Equinus) | 40% - 60% | Failure of muscle to elongate at the rate of bone distraction. Rigid plantarflexion. | Stop distraction. Aggressive PT, Botox injections, Percutaneous Achilles Lengthening, frame extension to foot. |
| Premature Consolidation | 5% - 15% | Latency too long or distraction too slow. Regenerate ossifies before target length is reached. | Return to OR for closed osteoclasis or open re-corticotomy. Increase distraction rate post-op. |
| Delayed / Non-Union | 5% - 10% | Traumatic corticotomy, unstable frame, or poor host biology. Radiolucent gap persists. | "Accordion maneuver" (alternating compression/distraction), bone grafting, exchange to internal fixation (LON). |
| Nerve Injury / Palsy | 3% - 8% | Direct pin injury or stretch neuropraxia (e.g., Peroneal nerve). Paresthesia, foot drop. | Immediate cessation of lengthening. If stretch injury: shorten limb slightly and wait. If direct injury: immediate pin removal/exploration. |
Phased Post-Operative Rehabilitation Protocols
The surgical application of the external fixator represents merely the first 10% of the overall treatment effort; the remaining 90% is dictated by an exhaustive, daily post-operative rehabilitation and management protocol. During the latency phase (Days 0-7), the primary goals are pain control, edema management, and the initiation of protected range of motion (ROM) of the adjacent joints. The limb must be elevated strictly to prevent massive swelling, which can compromise skin viability around the pin sites. Weight-bearing is generally restricted to toe-touch or partial weight-bearing to protect the fresh corticotomy hematoma.
Upon initiation of the distraction phase, the rehabilitation paradigm shifts dramatically. The patient must engage in aggressive, daily physical therapy to combat the rapidly developing soft tissue contractures. Active and active-assisted ROM exercises are mandatory. For tibial lengthenings, the patient must sleep in a rigid ankle-foot orthosis (AFO) or a dynamic splint attached to the frame to maintain the ankle in neutral dorsiflexion. Weight-bearing is progressively increased; the axial loading provided by ambulation is a critical mechanical signal that stimulates the orientation and mineralization of the regenerate bone columns. Nutritional optimization is paramount during this highly metabolic phase; patients require high-protein diets and aggressive supplementation with Vitamin D3, Calcium, and Vitamin C to support immense osteoblastic activity.
The consolidation phase begins when the target length is achieved. The frame is locked, and the focus shifts entirely to maximizing weight-bearing and functional use of the limb to drive corticalization of the regenerate. Radiographic monitoring transitions from weekly to monthly. The surgeon evaluates the regenerate for the appearance of three distinct cortices on orthogonal radiographs before considering frame removal. Premature frame removal is a catastrophic error, inevitably leading to plastic deformation, bending, or frank fracture of the soft regenerate bone. To mitigate this risk, many surgeons employ a "dynamization" protocol—progressively loosening the frame struts to transfer increasing mechanical load to the bone—prior to definitive removal.

Summary of Landmark Literature and Clinical Guidelines
The foundational literature underpinning distraction osteogenesis is unequivocally traced to Gavriil Ilizarov's seminal publications in the late 1980s, translated into English in Clinical Orthopaedics and Related Research (CORR). Ilizarov's papers on the "tension-stress effect" systematically documented the histological and biomechanical prerequisites for successful bone regeneration, establishing the absolute necessity of corticotomy preservation, rigid fixation, and a rhythmic 1 mm/day distraction rate. These principles remain the immutable biological laws of limb lengthening to this day, regardless of the technological advancements in fixation devices.
In the 1990s, Dror Paley published extensively on the comprehensive classification and management of complications in limb lengthening, effectively standardizing the international approach to these high-risk procedures. Paley's introduction of the CORA methodology and his textbook, Principles of Deformity Correction, revolutionized the pre-operative planning process, transitioning it from an empirical art to a highly reproducible, geometric science. His work established the standard clinical guidelines for mechanical axis restoration and joint orientation angle preservation, which are now globally recognized as the gold standard in orthopedic residency training.
The modern era of limb lengthening literature is heavily focused on mitigating the massive psychological and physical burden of prolonged external fixation. The development of the Taylor Spatial Frame (TSF) by J. Charles Taylor introduced computer-assisted, six-axis deformity correction, significantly reducing the incidence of residual malalignment. More recently, the advent of fully implantable, motorized intramedullary lengthening nails (e.g., PRECICE, STRYDE) has dominated the literature. These devices utilize magnetic gearing systems to lengthen the bone from within, entirely eliminating the external fixator and its associated pin-site infections. While currently
Clinical & Radiographic Imaging Archive