Mastering Deltoid Ligament Reconstruction: An Intraoperative Guide

Key Takeaway
This masterclass guides orthopaedic fellows through deltoid ligament reconstruction for chronic insufficiency, primarily in stage IV AAFD. We cover essential anatomy, meticulous preoperative planning, exact patient positioning, and a step-by-step minimally invasive allograft technique. Critical intraoperative pearls, potential pitfalls, and comprehensive postoperative protocols are emphasized, ensuring optimal outcomes for complex medial ankle instability.
Comprehensive Introduction and Patho-Epidemiology
The surgical management of deltoid ligament insufficiency represents one of the most formidable challenges in reconstructive foot and ankle surgery. Historically underappreciated, the deltoid ligament is now recognized as the primary medial stabilizer of the tibiotalar and subtalar joints. When we discuss deltoid ligament deficiency today, we are addressing a profound failure of the entire medial ankle complex, most frequently encountered in the context of late-stage Progressive Collapsing Foot Deformity (PCFD), formerly known as adult acquired flatfoot deformity (AAFD). This pathology is not merely an isolated ligamentous tear; it is the culmination of a biomechanical cascade that destroys the medial column's integrity, fundamentally altering the mechanical axis of the lower extremity and leading to catastrophic joint subluxation.
The pathomechanics of chronic deltoid insufficiency are inextricably linked to the failure of the dynamic and static restraints of the medial arch. As the posterior tibial tendon (PTT) becomes attenuated or frankly ruptured, the active ability to dynamically invert the hindfoot and stabilize the transverse tarsal joint during the stance phase of gait is entirely lost. Consequently, the mechanical axis of the leg shifts medial to the center of the ankle joint. This relentless, uncompensated valgus thrust places immense, unsustainable tensile loads on the static medial soft tissues, namely the spring ligament complex and the deltoid ligament. Over time, the native deltoid ligament complex undergoes myxoid degeneration and pathological elongation, eventually failing to resist tibiotalar valgus tilt.
While degenerative attritional failure secondary to PCFD is the most common etiology, deltoid ligament deficiency can also arise from severe traumatic events, chronic athletic microtrauma, or iatrogenic causes following extensive medial ankle dissection. It is imperative to distinguish chronic, attritional insufficiency from acute avulsions or ruptures associated with rotational ankle fractures (e.g., Weber B or C with medial clear space widening). In acute trauma, primary repair with suture anchors or transosseous sutures is generally sufficient. Conversely, in the chronic setting, the native ligamentous tissue is fibrotic, retracted, and biologically non-viable for simple primary repair or reefing. The tissue simply lacks the structural integrity to withstand the physiological loads of weight-bearing, necessitating anatomic reconstruction using robust autograft or allograft tissue.
Progression to stage IV PCFD is the hallmark clinical scenario for deltoid ligament incompetence. In this advanced stage, the chronic valgus force generated by the severe, long-standing hindfoot deformity causes the talus to tilt pathologically within the ankle mortise. This tibiotalar tilt signals a profound, global instability of the ankle joint that demands comprehensive surgical intervention. Failure to address the incompetent deltoid ligament during the reconstruction of a stage IV PCFD will invariably lead to recurrent valgus deformity, accelerated tibiotalar osteoarthritis, and ultimate failure of any concomitant medial column or hindfoot procedures.
Detailed Surgical Anatomy and Biomechanics
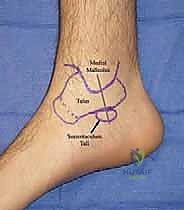
A masterful reconstruction of the deltoid ligament requires an intimate, three-dimensional understanding of the medial ankle anatomy. The deltoid ligament complex is not a single, monolithic band, but rather a highly sophisticated, multi-fascicular structure that provides essential restraint for the tibiotalar joint, subtalar joint, and talonavicular joint. It is universally classified into deep and superficial components, each serving distinct biomechanical roles. Navigating this anatomy intraoperatively requires precision to restore function while avoiding catastrophic iatrogenic injury to adjacent neurovascular bundles and tendinous structures.
The Deep Deltoid Ligament Complex
The deep portion of the deltoid ligament is the primary, indispensable stabilizer of the tibiotalar joint, acting as the primary restraint to lateral talar excursion and external rotation of the talus within the mortise. It originates from the intercollicular groove and the posterior colliculus of the medial malleolus. Its insertion is firmly planted on the medial face of the talar body, precisely near the center of rotation of the tibiotalar joint. These fibers are characteristically short, stout, and horizontally oriented. Crucially, they are intra-articular but extrasynovial. The deep deltoid is further subdivided into the anterior tibiotalar ligament (ATTL) and the posterior tibiotalar ligament (PTTL). Attenuation or rupture of these deep fibers directly and immediately results in lateral talar shift and valgus tibiotalar tilt.
The Superficial Deltoid Ligament Complex
The superficial components of the deltoid ligament form a broad, fan-shaped array that crosses two joints (the ankle and the subtalar joint). Pankovich and Shivaram classically described this layer as comprising the tibionavicular, tibiocalcaneal, and superficial tibiotalar ligaments. These fibers originate broadly across the anterior border and tip of the medial malleolus and extend distally to insert onto the navicular tuberosity, the sustentaculum tali, and the medial talar tubercle, respectively. While the deep deltoid prevents talar shift, the superficial deltoid acts as a secondary restraint to talar eversion and provides significant stability to the medial hindfoot, resisting calcaneal valgus. Reconstruction techniques must address both layers to restore true multidirectional stability.
Critical Neurovascular and Muscular Intervals
Surgical exposure of the medial ankle is fraught with potential hazards. The saphenous nerve and the great saphenous vein run anterior to the medial malleolus. The saphenous nerve, a terminal sensory branch of the femoral nerve, is highly variable in its arborization over the medial malleolus. Our initial longitudinal incision and subsequent tibial tunnel placement must be meticulously planned and executed with blunt dissection to retract and protect these structures. Iatrogenic injury to the saphenous nerve can result in debilitating neuromas or painful paresthesias that overshadow an otherwise successful biomechanical reconstruction.
Furthermore, the posterior tibial tendon (PTT) sheath lies immediately posterior to the medial malleolus, intimately wrapping around the sustentaculum tali of the calcaneus. During the creation of the calcaneal tunnel, the surgeon must carefully incise the retinaculum and retract the PTT sheath inferiorly. This allows access to the bony footprint of the sustentaculum without damaging the tendon itself, which, although often diseased in PCFD, may be targeted for concomitant debridement or transfer. Additionally, the sustentaculum tali forms the roof of the middle facet of the subtalar joint. Calcaneal tunnel drilling must be perfectly centralized within the sustentaculum to avoid breaching the subtalar articulation, which would precipitate iatrogenic subtalar arthritis.
Exhaustive Indications and Contraindications
The decision to proceed with a deltoid ligament reconstruction requires a highly nuanced clinical judgment, balancing the severity of the deformity against the patient's physiological capacity for extensive reconstruction and subsequent rehabilitation. The primary indication is chronic deltoid ligament insufficiency resulting in a flexible (reducible) tibiotalar valgus tilt, most commonly seen in Stage IV PCFD. The reducibility of the deformity is the absolute crux of the decision-making process; the surgeon must be able to passively correct the talus back beneath the tibial plafond to a neutral anatomical position.
Contraindications are equally critical to recognize. A rigid, non-reducible tibiotalar valgus deformity is an absolute contraindication for ligamentous reconstruction. Attempting to reconstruct a rigid joint will inevitably lead to hardware failure, graft rupture, and persistent deformity. In such cases, a tibiotalocalcaneal (TTC) arthrodesis or pantalar arthrodesis is the required salvage procedure. Furthermore, advanced tibiotalar osteoarthritis (Kellgren-Lawrence grade III or IV) precludes joint-sparing reconstruction, as re-aligning an arthritic joint will not alleviate the patient's pain and may exacerbate it by altering contact pressures on denuded cartilage.
Patient-specific factors also dictate surgical candidacy. Severe peripheral neuropathy, such as that seen in Charcot neuroarthropathy, is an absolute contraindication, as the lack of protective sensation will lead to rapid destruction of the reconstruction. Active local or systemic infection, severe peripheral vascular disease, and profound medical comorbidities that preclude prolonged anesthesia or non-weight-bearing rehabilitation must also be carefully weighed.
| Category | Specific Criteria | Rationale / Clinical Impact |
|---|---|---|
| Primary Indications | Stage IV PCFD with flexible tibiotalar valgus | Restores medial stability; prevents progression to end-stage arthritis. |
| Chronic medial ankle instability post-trauma | Addresses attritional elongation of the medial collateral complex. | |
| Iatrogenic deltoid failure (flexible) | Salvages medial column collapse following prior incomplete surgeries. | |
| Absolute Contraindications | Rigid, non-reducible tibiotalar valgus | Ligament reconstruction cannot overcome fixed bony/capsular contractures. Requires TTC fusion. |
| Advanced tibiotalar osteoarthritis | Re-alignment will not resolve arthritic pain; requires arthrodesis or arthroplasty. | |
| Active infection or severe vascular disease | High risk of catastrophic surgical site infection or limb loss. | |
| Charcot neuroarthropathy | Insensate joints will rapidly destroy soft tissue reconstructions. | |
| Relative Contraindications | Morbid obesity (BMI > 40) | Exponentially increases stress on the graft, raising the risk of early mechanical failure. |
| Non-compliant patient | Inability to adhere to strict 6-8 week NWB protocols will doom the graft. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the foundation upon which a successful deltoid ligament reconstruction is built. The evaluation begins with a comprehensive clinical assessment. We must confirm the presence of hindfoot valgus and evaluate the strength of the PTT. A positive Silfverskiöld test is frequently encountered, indicating a gastrocnemius or triceps surae contracture resulting from chronic hindfoot valgus and equinus compensation. Re-establishing plantigrade alignment without addressing this contracture (via gastrocnemius recession or Achilles lengthening) will subject the midfoot to excessive dorsiflexion forces, jeopardizing the reconstruction.
Imaging is paramount. Weight-bearing anteroposterior (AP), lateral, and mortise radiographs of the ankle are mandatory. A valgus tilt of the talus within the mortise greater than 4 degrees is a definitive radiographic indicator of deep deltoid ligament insufficiency.

FIG 1 • Standing AP weight-bearing radiograph of the ankle demonstrating severe valgus tibiotalar tilt, the hallmark of deep deltoid complex insufficiency.
Advanced imaging, specifically Magnetic Resonance Imaging (MRI), is highly recommended. MRI allows for the direct visualization of the deltoid ligament's integrity, confirming discontinuity, severe attenuation, or fibrotic degeneration. Furthermore, it is essential for assessing the status of the articular cartilage of the tibiotalar and subtalar joints. If we plan to utilize an autograft (such as a split peroneus longus), the MRI confirms the health of the peroneal tendons.
Before positioning the patient, an Examination Under Anesthesia (EUA) is performed. This is the final, definitive opportunity to confirm the reducibility of the tibiotalar deformity free from patient guarding. Intraoperative fluoroscopy is utilized during the EUA to objectively visualize the correction of the talus beneath the tibial plafond. Any concomitant bony procedures required to restore the mechanical axis—such as a medial displacement calcaneal osteotomy (MDCO), lateral column lengthening, or first tarsometatarsal arthrodesis—must be executed prior to the deltoid reconstruction. The foot must be anatomically aligned before the new ligament graft is tensioned.
Patient positioning is standardized but critical. The patient is placed supine on the operating table. A soft bump is placed beneath the ipsilateral hip; this internally rotates the lower extremity, bringing the medial malleolus parallel to the floor and optimizing our surgical trajectory. A thigh tourniquet is applied over cast padding to ensure a bloodless field, which is vital for identifying the saphenous nerve and precisely placing the osseous tunnels. The entire lower extremity is prepped and draped freely above the knee, allowing the surgeon to continuously assess the overall mechanical axis of the leg relative to the hindfoot throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
Today, we detail the Minimally Invasive Deltoid Ligament Reconstruction (MIDLR) technique. This advanced procedure anatomically reconstructs both the deep (tibiotalar) and superficial (tibiocalcaneal) layers of the deltoid ligament using a robust allograft, thereby preserving host tissue and minimizing donor site morbidity.
Initial Exposure and Graft Preparation
The procedure begins with a meticulously planned medial longitudinal incision. The incision extends from approximately 2 cm proximal to the tip of the medial malleolus, coursing distally to a point just inferior to the palpable prominence of the sustentaculum tali. Dissection is carried sharply through the dermis, followed by blunt dissection through the subcutaneous tissues to rigorously identify and protect the saphenous vein and nerve, retracting them anteriorly. The periosteum over the medial malleolus is incised, and subperiosteal flaps are elevated to expose the anterior and posterior colliculi, the medial face of the talus, and the sustentaculum tali.
Simultaneously, the graft is prepared on the back table. We utilize a dense, high-tensile cadaveric allograft, typically a peroneus longus or posterior tibial tendon, measuring approximately 20 cm in length and 6 to 7 mm in diameter. The graft is "forked" by splitting one end longitudinally for two-thirds of its length, leaving a 5 cm unsplit proximal portion. This unsplit end will serve as the tibial limb, while the two split tails will become the talar (deep) and calcaneal (superficial) limbs. Krackow stitches using #2 high-strength non-absorbable suture are placed in all three terminal ends to facilitate passage and tensioning.

TECH FIG 1 • Preparation of the forked allograft. The tendon is split longitudinally, and Krackow sutures are meticulously placed in the tibial, talar, and calcaneal limbs.
Osseous Tunnel Creation
The success of the reconstruction relies entirely on anatomic tunnel placement. We begin with the tibial tunnel. Under fluoroscopic guidance, a starting point is identified in the mid-coronal plane of the medial malleolus, exactly 1 cm proximal to the tibiotalar joint line (plafond). A guidewire is advanced from medial to lateral, parallel to the joint surface, exiting the lateral tibial cortex. This is over-reamed with a cannulated drill matched to the diameter of the unsplit graft (typically 6-7 mm) to a depth of 30 mm.
TECH FIG 2 • Fluoroscopically guided insertion of the tibial guidewire, ensuring placement parallel to the plafond and 1 cm proximal to the joint line.
Next, the talar tunnel is established to recreate the deep deltoid footprint. The target is the medial central body of the talus, inferior to the articular margin. A guidewire is directed from medial to lateral, aiming slightly anteriorly and inferiorly to avoid penetrating the subtalar joint or the lateral talar articular surface. This is over-reamed to a depth of 20-25 mm using a drill matched to the diameter of the talar limb (typically 4.5-5 mm).

TECH FIG 3 • Drilling the talar tunnel. The trajectory targets the anatomic footprint of the deep deltoid ligament on the medial talar body.
Finally, the calcaneal tunnel is drilled to reconstruct the superficial layer. The PTT sheath is carefully retracted inferiorly to expose the sustentaculum tali. The guidewire is placed in the center of the sustentaculum, directed laterally and slightly inferiorly towards the lateral calcaneal wall. Extreme caution is exercised to maintain a trajectory that remains completely extra-articular, avoiding the middle facet of the subtalar joint located immediately superior to the drill path.

TECH FIG 4 • Preparation of the calcaneal tunnel within the sustentaculum tali, maintaining an extra-articular trajectory beneath the subtalar joint.
Graft Passage, Tensioning, and Fixation
With all tunnels prepared, the graft is introduced into the surgical field. Using passing sutures, the unsplit proximal limb of the graft is drawn into the tibial tunnel.
TECH FIG 5 • Initial introduction of the graft into the surgical field.
TECH FIG 6 • The unsplit tibial limb is passed into the medial malleolar tunnel.
The tibial limb is secured first, typically utilizing a bio-tenodesis interference screw sized identically to the tunnel diameter, ensuring rigid aperture fixation. Once the tibial anchor is secure, the two split tails are routed to their respective distal tunnels.

TECH FIG 7 • Routing the talar limb of the forked graft towards the talar tunnel.

TECH FIG 8 • Routing the calcaneal limb inferiorly towards the sustentaculum tali.
Tensioning is the most critical phase of the operation. The foot is held in neutral dorsiflexion and slight varus to fully reduce the tibiotalar and subtalar joints. The talar limb (reconstructing the deep deltoid) is tensioned first. While the assistant maintains the anatomic reduction, an interference screw is advanced into the talar tunnel, locking the graft and instantly eliminating the valgus talar tilt.
TECH FIG 9 • Tensioning the talar limb while maintaining the hindfoot in a corrected, neutral-to-slight varus position.

TECH FIG 10 • Interference screw fixation of the talar limb, securing the deep deltoid reconstruction.
Following deep layer fixation, the calcaneal limb (reconstructing the superficial deltoid) is tensioned. The hindfoot remains in neutral alignment. The calcaneal limb is pulled taut into the sustentacular tunnel and secured with a final interference screw. This dual-layer tensioning restores the complex, multi-planar stability of the medial ankle.

TECH FIG 11 • Final tensioning and interference screw fixation of the calcaneal limb within the sustentaculum tali.
Before closure, a final fluoroscopic evaluation is mandatory. An AP mortise view is obtained to confirm the absolute resolution of the tibiotalar valgus tilt and to verify that all hardware is extra-articular. The wounds are then irrigated and closed in a layered fashion.

TECH FIG 12 • Final intraoperative fluoroscopy confirming anatomic restoration of the mortise and complete resolution of the valgus tilt.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, deltoid ligament reconstruction carries a distinct complication profile. The most prevalent soft-tissue complication is saphenous neuritis or neuroma formation, occurring in approximately 5-10% of cases. This is secondary to the intimate proximity of the nerve to the medial incision and tibial tunnel. Meticulous blunt dissection and the use of protective retractors are paramount. If a neuroma develops and is refractory to conservative management (gabapentinoids, targeted injections), surgical excision and proximal burying of the nerve stump may be required.
A devastating intraoperative complication is the iatrogenic violation of the subtalar joint during calcaneal tunnel drilling. The sustentaculum tali is a relatively narrow osseous bridge; a drill trajectory that strays superiorly will breach the articular cartilage of the middle facet. This inevitably leads to accelerated subtalar osteoarthritis, presenting as chronic, deep hindfoot pain postoperatively. Preoperative templating and strict adherence to fluoroscopic guidance during guidewire placement are non-negotiable to prevent this error. If recognized intraoperatively, the trajectory must be immediately redirected.
The most significant mechanical complication is recurrent valgus deformity and graft failure, seen in up to 15% of long-term follow-ups. This usually stems from one of two errors: failure to adequately correct the underlying bony deformity (e.g., omitting a necessary calcaneal osteotomy) or premature weight-bearing by a non-compliant patient before graft incorporation occurs. If the graft fails and the valgus tilt recurs, the joint rapidly becomes arthritic. Salvage in these scenarios precludes a second soft-tissue reconstruction; the definitive management is a rigid tibiotalocalcaneal (TTC) arthrodesis using an intramedullary nail or robust plating system.
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management |
|---|---|---|---|
| Saphenous Neuritis/Neuroma | 5 - 10% | Meticulous blunt dissection; anterior retraction of the neurovascular bundle. | Gabapentinoids, targeted steroid injections; surgical excision and proximal burying if refractory. |
| Recurrent Valgus Deformity | 10 - 15% | Concomitant correction of all bony deformities (MDCO, column lengthening); strict NWB protocol. | Tibiotalocalcaneal (TTC) or Pantalar Arthrodesis. |
| Subtalar Joint Violation | < 5% | Precise fluoroscopic targeting of the sustentaculum tali; aiming slightly inferiorly. | Conservative management initially; definitive treatment is Subtalar Arthrodesis. |
| Hardware Prominence/Pain | 5 - 8% | Countersinking interference screws; using bio-composite or PEEK materials. | Hardware removal after complete graft incorporation (minimum 9-12 months). |
| Superficial Wound Infection | 2 - 4% | Careful soft tissue handling; avoiding excessive tension on the medial skin flap. | Oral antibiotics, local wound care. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a deltoid ligament reconstruction is prolonged and demands absolute patient compliance. The newly implanted allograft relies entirely on mechanical fixation (interference screws) for the first several weeks until biological incorporation (Sharpey's fibers) begins at the bone-tendon interface. Premature loading will cause micro-motion at this interface, leading to tunnel widening, graft elongation, and ultimate clinical failure.
Phase I: Maximum Protection (Weeks 0 to 6)
