Lesser Toe Angular Deformity: An Intraoperative Masterclass on Surgical Correction

Key Takeaway
This masterclass provides an exhaustive guide to surgical correction of lesser toe angular deformities. Delve into comprehensive anatomy, meticulous preoperative planning, and granular, real-time intraoperative execution of procedures like FDL transfer and Weil osteotomy. Learn critical pearls, pitfalls, and post-operative management, ensuring optimal patient outcomes for complex foot conditions.
Welcome, colleagues, to the operating theater. Today, we embark on a comprehensive exploration of a ubiquitous yet deceptively complex challenge in foot and ankle surgery: angular deformities of the lesser toes. Far from being mere cosmetic nuisances, these multiplanar deviations precipitate profound functional disability, intractable pain, and a severe deterioration in a patient's quality of life. As reconstructive orthopedic surgeons, our mandate extends beyond simple realignment; we must meticulously restore the intricate biomechanical harmony of the forefoot to achieve a pain-free, functionally robust digit that accommodates normal footwear and withstands the rigors of the gait cycle.
Comprehensive Introduction and Patho-Epidemiology
Before we contemplate surgical intervention, a profound mastery of the underlying patho-anatomy and epidemiological context is absolutely paramount. Angular deformities of the lesser toes represent a spectrum of structural failures, each defined by distinct etiologies, variable presentations, and specific biomechanical derangements. The overarching goal of any intervention hinges on accurately categorizing the deformity to tailor a highly specific surgical algorithm.
Clinical Definitions and Deformity Spectrum
The quintessential presentation is the Crossover Second Toe Deformity. In this scenario, the second digit subluxates dorsomedially, frequently overlapping the hallux. Conversely, it may present as an inferomedial subluxation, effectively crossing beneath the great toe. This deformity is intrinsically linked to a hyperextension or hyperflexion contracture at the metatarsophalangeal (MTP) joint, coupled with profound adduction of the second ray. This is not an isolated event but a catastrophic failure of the stabilizing structures.

Equally challenging is the Congenital Crossover Fifth Toe, a variable developmental anomaly wherein the proximal phalanx of the fifth digit deviates dorsomedially, overriding the fourth toe. Patients invariably present with debilitating irritation and hyperkeratotic lesions on the dorsum of the fifth digit, exacerbated by conventional shoe wear. This requires a nuanced understanding of the dorsal contractures and skin tension lines prior to surgical release.

The Curly Toe Deformity represents a distinct congenital entity, predominantly observed in the pediatric population. It is characterized by a flexible flexion deformity at both the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints. This often manifests with the fourth toe underlapping the third, and the fifth underlapping the fourth. The etiology is frequently attributed to an imbalance or paresis of the intrinsic musculature, although the exact pathophysiological mechanism remains a subject of academic debate.
Isolated Deformities and Natural Progression
We must also distinguish the Isolated Metatarsophalangeal (MTP) Angular Deformity. This pathology involves pure varus or valgus angulation occurring exclusively at the MTP articulation. It is frequently, though not exclusively, observed in conjunction with advanced hallux varus or hallux valgus, highlighting the interconnected nature of forefoot biomechanics.
Finally, Clinodactyly must be recognized as a distinct structural anomaly. Unlike MTP-driven deformities, clinodactyly involves coronal plane deviation (varus or valgus) arising from an abnormal angulation within the phalangeal shaft or at the interphalangeal joint surfaces themselves. While more ubiquitous in the hand, pedal clinodactyly is often syndromic and requires intra-articular or extra-articular osteotomies rather than soft-tissue balancing.

The natural history of these deformities invariably follows a predictable, attritional cascade. The initial insult typically manifests as localized MTP joint synovitis. Chronic inflammation degrades the capsuloligamentous complex, precipitating dynamic subluxation. Unchecked, this relentless progression culminates in frank dorsomedial or inferomedial dislocation. This attritional process disproportionately targets the lateral collateral ligament and the lateral aspect of the plantar plate, particularly in the pathogenesis of the crossover second toe.

Detailed Surgical Anatomy and Biomechanics
A successful surgical reconstruction demands an encyclopedic knowledge of forefoot anatomy. The stability of the lesser toes relies on an exquisitely delicate equilibrium between the static ligamentous restraints and the dynamic myotendinous forces. Disruption of a single vector can precipitate a rapid, cascading collapse of the entire digit.
Static Stabilizing Structures
The primary static stabilizers are the Collateral Ligaments (Medial and Lateral) and the Plantar Plate. The collateral ligaments originate from the dorsal-eccentric aspect of the metatarsal head, fanning out to insert onto the base of the proximal phalanx and the margins of the plantar plate. They are the primary restrictors of transverse plane deviation and dorsal translation. Attenuation or frank rupture of the Lateral Collateral Ligament (LCL) is the hallmark of medial crossover deformities.
The Plantar Plate is a robust, fibrocartilaginous, trapezoidal structure that intimately reinforces the plantar MTP joint capsule. It serves a dual purpose: resisting MTP joint hyperextension and providing a smooth, stable fulcrum for the flexor tendons. Disruption of the plantar plate—most commonly an avulsion from its phalangeal insertion—is the defining pathological event in sagittal plane instability and subsequent dorsal dislocation.

The Joint Capsule itself provides secondary, global stability. However, in chronic deformities, the dorsal capsule invariably undergoes profound contracture, tethering the proximal phalanx in a hyperextended posture. Surgical release of this dorsal contracture is a mandatory step in virtually all corrective algorithms.

Dynamic Myotendinous Forces
The dynamic stabilizers are a complex interplay of extrinsic and intrinsic musculature. The Extensor Digitorum Longus (EDL) and Extensor Digitorum Brevis (EDB) exert a powerful dorsal vector. When the plantar plate fails, these extensors gain a mechanical advantage, exacerbating the dorsal subluxation. Conversely, the Flexor Digitorum Longus (FDL) and Flexor Digitorum Brevis (FDB) provide the counterbalancing plantar flexion force.
The true keystones of dynamic stability, however, are the Lumbricals and Interossei. These intrinsic muscles course plantar to the MTP joint axis (acting as MTP flexors) and dorsal to the PIP/DIP joint axes (acting as interphalangeal extensors). This unique anatomical arrangement is essential for stabilizing the proximal phalanx against the metatarsal head during the propulsive phase of gait. Intrinsic failure or imbalance directly precipitates the classic "claw toe" and crossover deformities.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention must be highly calculated, balancing the severity of the deformity against the patient's physiological reserves and functional demands. We must strictly differentiate between flexible, reducible deformities and rigid, fixed contractures, as this distinction dictates our entire surgical approach.
Determining Operability
Surgical intervention is indicated when exhaustive conservative measures—including extra-depth footwear, custom orthoses with metatarsal offloading, and dynamic splinting—have failed to provide durable symptomatic relief. Painful, intractable plantar keratoses (IPKs) beneath the lesser metatarsal heads, or ulcerating dorsal corns over the PIP joints, are strong surgical indications.

For flexible deformities, soft-tissue rebalancing (e.g., extensor lengthening, capsulotomies, and tendon transfers) is often sufficient. However, if the deformity is rigid, or if there is profound osseous malalignment (such as an excessively long second metatarsal), bony procedures—including metatarsal shortening osteotomies and interphalangeal arthrodeses—become mandatory to achieve lasting correction.
Absolute and Relative Contraindications
We must remain vigilant regarding contraindications. Severe peripheral vascular disease (PVD) is an absolute contraindication; operating on an ischemic digit guarantees necrosis and amputation. Active local or systemic infection precludes elective reconstruction. Relative contraindications include poorly controlled diabetes mellitus, profound peripheral neuropathy (which risks Charcot neuroarthropathy or unrecognized hardware failure), and unrealistic patient expectations regarding postoperative cosmesis versus functional recovery.
Indications and Contraindications Matrix
| Parameter | Indications for Surgery | Contraindications for Surgery |
|---|---|---|
| Clinical Presentation | Failure of conservative therapy (>6 months); Intractable pain; Ulcerating corns/IPKs. | Asymptomatic deformity; purely cosmetic concerns. |
| Deformity Type | Progressive crossover toe; Rigid hammertoe; Plantar plate rupture. | Active Charcot neuroarthropathy. |
| Vascular Status | Palpable pulses; ABI > 0.8; Biphasic/Triphasic doppler signals. | ABI < 0.5; Absent pulses; Severe microvascular disease. |
| Neurologic Status | Intact protective sensation. | Profound peripheral neuropathy (relative). |
| Systemic Health | Optimized glycemic control (HbA1c < 7.5%); Non-smoker. | Active infection; Uncontrolled diabetes; Heavy tobacco use. |

Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the crucible in which surgical success is forged. The clinical examination and radiographic analysis must be synthesized to formulate a precise, step-by-step intraoperative blueprint.
Clinical and Radiographic Evaluation
The physical examination must rigorously assess the flexibility of every joint in the affected ray. The Drawer Test is critical: stabilizing the metatarsal head while applying a dorsal translational force to the proximal phalanx. Excessive dorsal excursion or a palpable "clunk" confirms plantar plate insufficiency. We must also evaluate the great toe; an uncorrected hallux valgus will physically block the realignment of a crossover second toe, necessitating concurrent first ray reconstruction.

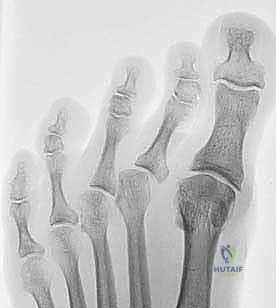
Weight-bearing radiographs are non-negotiable. The AP view allows us to assess the "metatarsal parabola." A second metatarsal that projects significantly distal to the first and third metatarsals is a primary biomechanical driver of crossover deformity and plantar plate rupture. The lateral view delineates the severity of sagittal plane subluxation and PIP joint contracture.


Digital Templating and OR Setup
Digital templating is essential, particularly when planning a Weil osteotomy. We must calculate the exact millimeter of shortening required to restore the metatarsal cascade and decompress the MTP joint. Over-shortening risks transfer metatarsalgia, while under-shortening guarantees deformity recurrence.

In the operating room, the patient is positioned supine. A well-padded thigh tourniquet is applied to ensure a pristine, bloodless surgical field—a necessity given the delicate neurovascular bundles of the forefoot. The foot must be positioned at the extreme edge of the radiolucent table extension to permit unhindered, multi-planar fluoroscopic imaging throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution must proceed systematically, addressing the pathology from proximal to distal, or soft tissue to bone, depending on the specific algorithm chosen. We employ a graduated approach, reassessing the deformity after each sequential release.
Soft Tissue Releases and Capsulotomy
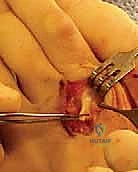
We typically begin with a longitudinal dorsal incision centered over the MTP joint, extending distally to the PIP joint if interphalangeal work is anticipated. Deepening the incision, we identify and protect the dorsal sensory nerve branches. A Z-lengthening of the Extensor Digitorum Longus (EDL) is performed, followed by a tenotomy of the Extensor Digitorum Brevis (EDB).

Next, a comprehensive dorsal capsulotomy is executed. We release the contracted dorsal capsule and the collateral ligaments off the metatarsal head. If the toe remains subluxated, we must inspect the plantar plate. Plantar plate repairs can be performed directly through this dorsal approach (often facilitated by a Weil osteotomy for exposure) or via a separate plantar incision. Suture anchors or transosseous tunnels in the proximal phalanx are utilized to reapproximate the torn plantar plate to its anatomical footprint.

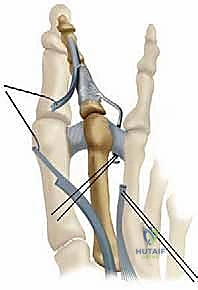
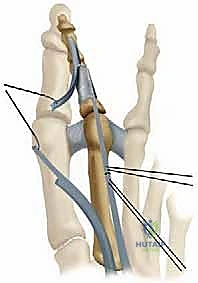
Flexor-to-Extensor Tendon Transfer (Girdlestone-Taylor)
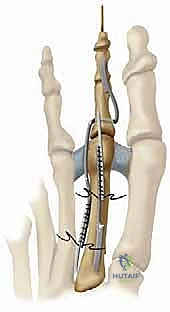
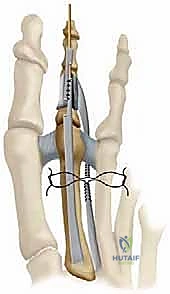
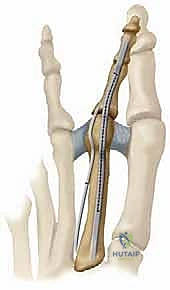
For flexible deformities lacking severe osseous malalignment, the Girdlestone-Taylor procedure is a highly effective dynamic stabilizer. The FDL tendon is harvested via a plantar incision at the distal interphalangeal crease or through the primary dorsal incision by tracing it proximally. The tendon is split longitudinally into two slips.

These slips are routed dorsally, passing adjacent to the proximal phalanx—taking extreme care to avoid the neurovascular bundles—and are sutured to the extensor hood or directly to each other over the dorsal aspect of the proximal phalanx. This transfer effectively converts a deforming plantar-flexion force at the DIP joint into a stabilizing plantar-flexion force at the MTP joint, correcting the clawing mechanism.
The Weil Osteotomy
When dealing with a rigid deformity, a dislocated MTP joint, or a disproportionately long metatarsal, the Weil osteotomy is the gold standard. Utilizing a microsagittal saw, an osteotomy is initiated at the dorsal cartilage margin of the metatarsal head, angled proximally and plantarly, parallel to the weight-bearing surface of the foot (typically 10 to 15 degrees relative to the metatarsal shaft).

This precise geometry allows the metatarsal head to slide proximally, achieving controlled shortening without plantar displacement, thereby decompressing the joint. The capital fragment is then provisionally fixed with a K-wire, and definitive fixation is achieved using one or two specialized twist-off or headless compression screws (typically 2.0mm). The overhanging dorsal ledge of the proximal metatarsal shaft is then meticulously resected to prevent dorsal impingement.

Proximal Interphalangeal (PIP) Joint Arthrodesis
If a rigid hammertoe deformity persists at the PIP joint, an arthrodesis is mandated. We resect the articular cartilage of the distal aspect of the proximal phalanx and the proximal aspect of the middle phalanx using a rongeur or a saw, creating flat, cancellous bony surfaces.


Fixation can be achieved via a traditional longitudinal intramedullary Kirschner wire (K-wire) driven distally through the toe and then retrograded into the proximal phalanx. Alternatively, modern intramedullary implants (e.g., nitinol memory-metal clips or specialized two-piece screw systems) offer robust internal fixation without the morbidity of exposed pins.


Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, reconstructive forefoot surgery carries a distinct complication profile. We must be prepared to identify and manage these adverse events swiftly to salvage the functional outcome.
The "Floating Toe" Phenomenon
Perhaps the most notorious complication following a Weil osteotomy is the "floating toe" deformity, characterized by an inability of the toe to contact the ground during weight-bearing. This occurs due to the proximal translation of the intrinsic muscle origins, which alters their mechanical axis, effectively converting them from MTP flexors to MTP extensors.
