Latissimus Dorsi Transfer for Irreparable Posterosuperior Rotator Cuff Tears: An Intraoperative Masterclass

Key Takeaway
Join us in the OR for a comprehensive masterclass on Latissimus Dorsi Transfer for irreparable posterosuperior rotator cuff tears. We'll meticulously cover patient selection, intricate surgical anatomy, precise intraoperative steps, critical pearls and pitfalls, and robust postoperative rehabilitation protocols. This detailed guide ensures a deep understanding of technique and rationale for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
The management of massive, irreparable posterosuperior rotator cuff tears remains one of the most formidable challenges in contemporary orthopedic surgery. When the supraspinatus and infraspinatus tendons are retracted, severely atrophied, and infiltrated with adipose tissue, anatomic restoration of the native footprint becomes a biomechanical and biologic impossibility. In these highly selected scenarios, the latissimus dorsi tendon transfer emerges not merely as a salvage operation, but as a sophisticated kinematic reconstruction designed to restore the essential transverse force couple of the glenohumeral joint.
Understanding the patho-epidemiology of these lesions requires an appreciation of shoulder biomechanics. The normal shoulder relies on a delicate balance between the anterior structures (subscapularis) and the posterior structures (infraspinatus and teres minor) to compress the humeral head into the glenoid concavity during active elevation. This concavity compression provides the stable fulcrum necessary for the deltoid to elevate the arm. When the posterosuperior cuff fails irrecoverably, this fulcrum is lost. The unopposed pull of the deltoid results in superior migration of the humeral head, leading to subacromial impingement, progressive articular cartilage wear, and the debilitating clinical presentation of pain and profound weakness, often termed "pseudoparalysis."
The rationale behind the latissimus dorsi transfer, originally popularized by Christian Gerber in the late 1980s, is to re-establish this lost posterior compressive force. By harvesting the latissimus dorsi—a native internal rotator, adductor, and extensor—and transferring its insertion to the superolateral greater tuberosity, we fundamentally alter its biomechanical vector. When successfully re-routed and rehabilitated, the transferred muscle acts as an external rotator and an active depressor of the humeral head. This procedure does not recreate a normal shoulder; rather, it stabilizes the humeral head, allowing the native deltoid to function efficiently once again, thereby restoring active forward flexion and external rotation while significantly mitigating the patient's pain profile.
Defining the Irreparable Tear
In the surgical theater, the definition of an "irreparable" tear transcends preoperative imaging and becomes a tactile reality. We define a tear as truly irreparable when, following extensive intra-articular and extra-articular releases, coracohumeral ligament sectioning, and capsular mobilization, the tendon edge cannot be advanced to the articular margin of the greater tuberosity with the arm resting at the patient's side or in less than 60 degrees of abduction. Attempting to repair a tendon under extreme tension in these conditions guarantees biological failure, suture pull-through, and a rapid return of symptoms.
Preoperatively, advanced imaging provides critical predictive indicators of irreparability. The Goutallier classification system remains the gold standard for assessing fatty infiltration on non-contrast MRI or CT arthrography. Tendons exhibiting Grade 3 (equal amounts of fat and muscle) or Grade 4 (more fat than muscle) fatty degeneration of the supraspinatus and infraspinatus bellies possess severely compromised elasticity and excursion. Furthermore, the Patte classification of tendon retraction, specifically Grade III (retraction proximal to the glenoid rim), strongly correlates with the inability to achieve a tension-free repair.
However, the ultimate determination is an intraoperative one. As surgeons, we must critically evaluate the tissue quality. Tendons that have undergone chronic retraction often present as thinned, friable, and mechanically incompetent tissue that will not hold a high-strength suture. Recognizing this intraoperatively is paramount; persisting with an ill-fated primary repair rather than transitioning to a planned tendon transfer or alternative salvage procedure is a disservice to the patient and a failure of surgical judgment.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel touches the skin, a profound, three-dimensional understanding of the regional anatomy is absolutely mandatory. The axilla and posterior shoulder girdle contain a dense network of critical neurovascular structures. In the context of a latissimus dorsi transfer, precision prevents peril. The margin for error when dissecting the muscle belly and mobilizing its pedicle is measured in millimeters.
The Latissimus Dorsi Muscle and Tendon Complex
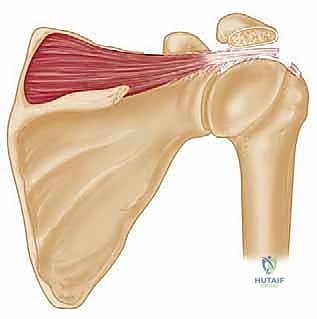
The latissimus dorsi is a massive, fan-shaped muscle that covers the inferior half of the posterior trunk. Its origin is incredibly broad, arising from the posterior layer of the thoracolumbar fascia (attaching to the spinous processes of T7 through L5 and the sacrum), the posterior third of the iliac crest, the lower three or four ribs, and occasionally the inferior angle of the scapula. As the muscle fibers converge toward the axilla, they undergo a remarkable morphological change: the muscle twists upon itself a full 180 degrees.
This anatomical twist dictates that the fibers originating most superiorly on the spine insert most inferiorly on the humerus, while the fibers originating from the iliac crest insert most superiorly. The tendon inserts into the floor of the intertubercular groove of the humerus, immediately anterior to the insertion of the teres major. The latissimus tendon is flat and robust, averaging 3.1 cm in width and 8.4 cm in length at its insertion point. Crucially for our surgical dissection, the humeral insertion of the latissimus dorsi never extends more distally along the humeral shaft than the insertion of the teres major. This consistent anatomical relationship is our primary landmark during the initial release.
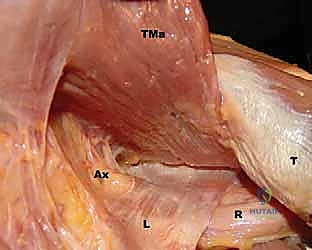
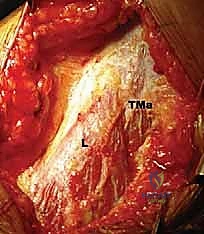
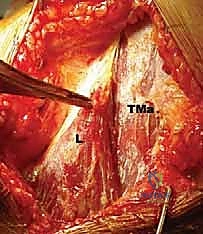
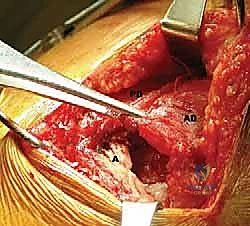
FIG 1 • A. Cadaveric dissection showing the interval between the teres major (TMa) and latissimus dorsi (L) tendons, with the radial nerve (R) deep to the latissimus and the axillary nerve (Ax) superior.
The Neurovascular Pedicle and Critical Structures
The viability of the transferred muscle relies entirely on the preservation of its solitary neurovascular pedicle: the thoracodorsal artery and nerve. Originating from the posterior cord of the brachial plexus (comprising nerve roots C6, C7, and C8), the thoracodorsal nerve travels distally along the posterior wall of the axilla. It enters the anterior, deep surface of the latissimus dorsi muscle belly approximately 13 cm medial and distal to its humeral insertion.
During mobilization, we must trace this pedicle proximally to ensure adequate excursion of the transferred tendon. Anatomic studies confirm that the pedicle is typically of sufficient length to allow for a tension-free transfer to the greater tuberosity, provided the surgeon meticulously releases all fascial adhesions and fibrous bands tethering the anterior surface of the muscle belly to the chest wall. Failure to adequately release these bands will result in a tethered transfer, limiting the reach of the tendon and placing dangerous traction on the thoracodorsal nerve.
Furthermore, we must navigate the relationship between the latissimus dorsi and the teres major. In approximately 70% of the population, these tendons insert separately. However, in the remaining 30%, the tendons are conjoined near their insertion. In these instances, blunt dissection is insufficient; sharp, meticulous dissection is required to separate the latissimus from the teres major without compromising the integrity of either structure or inadvertently injuring the underlying radial nerve.
Navigating the Radial and Axillary Nerves
The release of the latissimus dorsi insertion places two major peripheral nerves at immediate risk: the radial nerve and the axillary nerve. The radial nerve passes anterior and deep to the latissimus tendon, averaging a mere 2.4 cm medial to the humeral shaft at the superior border of the tendon. This proximity is highly dynamic; the distance increases with external rotation and abduction of the arm, and dangerously decreases with internal rotation and adduction.
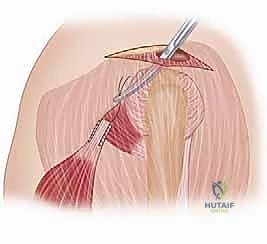
Similarly, the axillary nerve runs superior to the latissimus dorsi tendon just before it exits the quadrangular space to innervate the deltoid and teres minor. In neutral rotation and adduction, the average distance between the axillary nerve and the superior border of the latissimus tendon is only 1.9 cm. During the subdeltoid tunneling phase of the procedure, where the harvested tendon is passed from the posterior axilla to the superior footprint, the surgeon must maintain a plane superficial to the teres minor to avoid compressing or lacerating the axillary nerve.
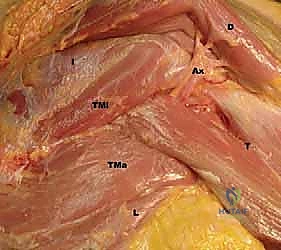
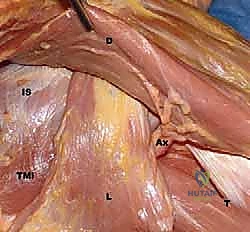
FIG 1 • C. Cadaveric dissection of the superficial muscular anatomy of the posterior shoulder, showing the axillary nerve (Ax) exiting the quadrilateral space.
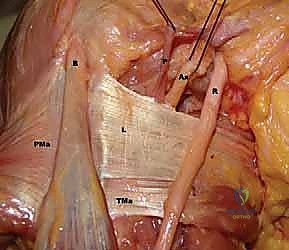
FIG 1 • Additional cadaveric view highlighting the dense neurovascular network surrounding the latissimus insertion.
Exhaustive Indications and Contraindications
The success of a latissimus dorsi transfer is inextricably linked to rigorous, almost uncompromising patient selection. This is a biomechanically demanding procedure that requires significant postoperative patient compliance and neuromuscular re-education. It is not a panacea for all massive rotator cuff tears.
Defining the Ideal Surgical Candidate
The ideal candidate for a latissimus dorsi transfer is typically a younger, physiologically active patient (generally under 65 years of age, though physiologic age supersedes chronological age) who presents with debilitating pain and weakness secondary to an irreparable posterosuperior rotator cuff tear. The primary indication is often intractable pain that has failed exhaustive conservative management, coupled with a loss of active external rotation and elevation.
Crucially, the patient must possess an intact and fully functional subscapularis tendon. The subscapularis is the critical anterior component of the transverse force couple; if it is deficient, the transferred latissimus dorsi will simply pull the humeral head posteriorly and superiorly, leading to rapid clinical failure and accelerated joint destruction. Furthermore, the patient must have a strong, functional deltoid muscle, as the transfer relies on the deltoid to perform the actual work of arm elevation once the humeral head is stabilized.
We also look for patients who can achieve at least shoulder-level active forward flexion preoperatively, or those who demonstrate significant improvement in active elevation following a diagnostic subacromial/intra-articular injection of local anesthetic (the "lidocaine test"). This test helps differentiate true biomechanical pseudoparalysis from pain-inhibited movement (pseudoparesis). Finally, the glenohumeral joint must be relatively free of advanced osteoarthritis.
FIG 3 • A. True AP radiographic view showing minimal superior migration and preserved joint space, indicative of an ideal candidate.

FIG 3 • A. Continued: True AP radiographic view confirming absence of significant degenerative changes.

FIG 3 • B. Axillary lateral view demonstrating excellent joint space preservation and absence of posterior glenoid wear or osteophytes.
Identifying Contraindications and Poor Prognosticators
Contraindications to this procedure must be strictly respected to avoid catastrophic outcomes. The most absolute contraindication is an irreparable tear of the subscapularis. Without anterior restraint, the latissimus transfer will fail biomechanically. Similarly, a dysfunctional deltoid muscle (e.g., due to previous axillary nerve injury) precludes this operation, as the primary motor for elevation is absent.
Advanced glenohumeral osteoarthritis (Hamada Grade 3 or higher) is a strong contraindication. If the articular cartilage is severely degraded, stabilizing the humeral head against a worn glenoid will not relieve pain and may exacerbate stiffness. In these scenarios, a reverse total shoulder arthroplasty (RTSA) is the definitively superior option.
True pseudoparalysis—defined as the absolute inability to actively elevate the arm beyond 90 degrees in the scapular plane, which does not improve with a lidocaine injection—is a relative contraindication. While some surgeons will attempt a transfer in these cases, the failure rate is significantly higher, and patients must be counseled that the primary goal is pain relief, not necessarily the restoration of overhead function. Finally, patients with severe medical comorbidities, inability to comply with a grueling 6-to-12-month rehabilitation protocol, or those lacking the cognitive capacity for neuromuscular re-education should be excluded.
FIG 3 • C. Radiographic findings of severe degenerative arthritis with massive osteophyte formation and superior migration. This is an absolute contraindication for LD transfer.

FIG 3 • D. Axillary lateral view showing advanced osteoarthritis with posterior glenoid wear, suggestive of a poor candidate better suited for arthroplasty.
Indications and Contraindications Matrix
| Parameter | Favorable Indication (Proceed with LD Transfer) | Absolute/Relative Contraindication (Consider Alternatives) |
|---|---|---|
| Patient Age/Activity | Younger, high functional demands | Elderly, low functional demands |
| Subscapularis Status | Intact and functional | Torn, irreparable, or severe fatty infiltration |
| Deltoid Status | Intact and strong (Grade 5/5) | Weak, denervated (axillary nerve palsy) |
| Glenohumeral Joint | Preserved joint space (Hamada 1-2) | Advanced Osteoarthritis (Hamada 3-5) |
| Active Elevation | > 90 degrees, or improves with Lidocaine | < 90 degrees (True Pseudoparalysis) unresponsive to local anesthetic |
| Coracoacromial Arch | Intact | Disrupted (previous radical acromionectomy) leading to superior escape |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative preparation is the foundation of a smooth intraoperative experience. This involves a meticulous physical examination, critical appraisal of advanced imaging, and precise operating room setup to facilitate both the harvest and the transfer of the tendon.
Clinical Evaluation and Kinematic Assessment
The physical examination must be exhaustive. We begin by assessing the active and passive range of motion. A discrepancy between passive and active motion highlights the muscular deficit. If passive motion is significantly restricted, the patient has a concomitant adhesive capsulitis or joint contracture that must be aggressively treated with physical therapy prior to any surgical intervention; transferring a muscle into a stiff joint guarantees failure.
Specific provocative tests are essential. The External Rotation Lag Sign (inability to maintain maximal external rotation with the arm at the side) and the Hornblower's Sign (inability to externally rotate the arm when abducted to 90 degrees) are critical indicators of severe infraspinatus and teres minor dysfunction, confirming the necessity of a posterior transfer. Conversely, we must rigorously test the subscapularis using the Belly Press Test, the Bear Hug Test, and the Lift-Off Test. Any weakness here is a red flag. Finally, deltoid strength must be confirmed manually in all three planes (anterior, middle, posterior).
Advanced Imaging Protocols: MRI and CT Arthrography
Standard radiographs (True AP, Scapular Y, and Axillary lateral) are obtained to assess for superior humeral head migration, acromiohumeral distance (AHD < 7mm suggests massive tear), and glenohumeral arthritis. However, advanced cross-sectional imaging is the cornerstone of our planning.
Non-contrast MRI in the sagittal oblique, coronal oblique, and axial planes allows for the definitive assessment of muscle quality. We utilize the Goutallier classification on the T1-weighted sagittal oblique images (typically at the level of the coracoid base, the "Y-view") to quantify fatty infiltration. Grade 3 or 4 infiltration in the supraspinatus and infraspinatus confirms irreparability. We also assess the degree of tendon retraction in the coronal plane. If MRI is contraindicated, a CT arthrogram provides excellent visualization of muscle atrophy and fatty infiltration, though it is slightly less sensitive for subtle tendon pathology.

FIG 4 • Preoperative MRI (Sagittal T1) demonstrating severe Goutallier Grade 4 fatty infiltration of the supraspinatus and infraspinatus muscle bellies.

FIG 5 • Coronal T2 MRI showing massive retraction of the rotator cuff tendons medial to the glenoid rim (Patte Grade III).
Patient Positioning and Operating Room Setup
The procedure is most commonly performed with the patient in the lateral decubitus position, utilizing a bean bag for rigid pelvic and torso stabilization. The patient is rolled slightly posteriorly (approximately 20-30 degrees) to allow simultaneous access to the posterior axilla for the harvest and the superior shoulder for the transfer.
The operative arm is prepped entirely free and suspended in a sterile, pneumatic, articulated arm positioner (such as a Spider or Trimano arm). This device is indispensable, as it allows the surgeon to effortlessly manipulate the arm into varying degrees of abduction, internal rotation, and external rotation throughout the case. As previously noted, manipulating the arm is critical for dropping the radial and axillary nerves away from our dissection planes during the tendon harvest and passage. All bony prominences (fibular head, greater trochanter) must be meticulously padded to prevent neuropraxias during what is often a lengthy procedure.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of the latissimus dorsi transfer is a masterclass in soft tissue handling, neurovascular preservation, and biomechanical fixation. We utilize a two-incision approach: a posterior axillary incision for harvesting the tendon, and a superior approach (often a mini-open or arthroscopically assisted deltoid-splitting approach) for footprint preparation and fixation.
Incision, Superficial Dissection, and Muscle Identification
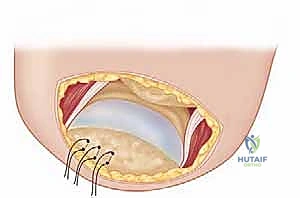
We begin with the posterior axillary incision. With the arm abducted to 90 degrees and internally rotated, an incision is made along the posterior axillary fold, extending from the axilla distally for approximately 10 to 15 centimeters. The subcutaneous tissue is divided, and the superficial fascia is incised to expose the lateral border of the latissimus dorsi muscle.
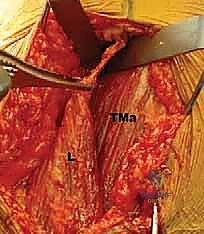
The immediate challenge is distinguishing the latissimus dorsi from the underlying teres major. The latissimus is more superficial and its fibers run more vertically, while the teres major fibers run more horizontally. We develop the interval between these two muscles using blunt dissection, sweeping the teres major medially. It is at this stage we must identify if a conjoined tendon exists; if so, sharp dissection is utilized to separate them, staying strictly on the latissimus side of the interface to protect the teres major.

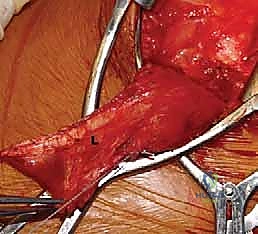
FIG 6 • Initial posterior axillary incision exposing the lateral border of the latissimus dorsi.