Lateral Column Lengthening: An Intraoperative Masterclass for Acquired Flatfoot Deformity

Key Takeaway
Join us in the OR for a comprehensive masterclass on lateral column lengthening, a critical procedure for supple acquired flatfoot deformity. We'll meticulously detail surgical anatomy, precise patient positioning, and the granular, real-time execution of the Evans osteotomy, from incision to fixation. Gain invaluable insights into pearls, pitfalls, and post-operative care, ensuring optimal outcomes for your patients.
Comprehensive Introduction and Patho-Epidemiology
The Evolution of Acquired Flatfoot Deformity
Welcome, fellows and colleagues, to the operating theater and this comprehensive masterclass. Today, we are addressing a pervasive yet biomechanically complex challenge in foot and ankle surgery: the supple acquired flatfoot deformity secondary to posterior tibial tendon insufficiency (PTTI). Our focus will be on the lateral column lengthening (LCL) procedure, specifically the anterior calcaneal osteotomy, classically known as the Evans osteotomy. This procedure, whether utilized in isolation or, more commonly, combined with medial-sided soft tissue or bony techniques, remains our preferred and most powerful method for correcting the dorsolateral peritalar subluxation and hindfoot valgus characteristic of Stage II disease, as originally classified by Johnson and Strom and later modified by Myerson.
The pathogenesis of this deformity is deeply rooted in the progressive failure of the dynamic and static stabilizers of the medial longitudinal arch. Posterior tibial tendon insufficiency represents the most frequent etiology of unilateral acquired flatfoot in the adult population. However, it is paramount to understand that the tendon does not fail in isolation. As the posterior tibial tendon undergoes myxoid degeneration and loses its mechanical advantage, a cascading failure of the secondary support structures ensues. The spring ligament complex (specifically the superomedial and inferior calcaneonavicular ligaments), the plantar fascia, and the deltoid ligament progressively attenuate. This catastrophic loss of medial support allows the midfoot to displace laterally and dorsally on the hindfoot, pivoting around the talonavicular joint, which ultimately manifests as a functionally shortened lateral column.
Clinically, these patients present with a constellation of symptoms that mirror the progressive anatomic collapse. Early in the disease process, patients often describe a vague, aching discomfort localized behind the medial malleolus, accompanied by tenosynovitis and swelling along the tendon sheath. As the deformity progresses, they report a profound lack of propulsion power during the toe-off phase of gait and demonstrate a pathognomonic inability to perform a single-limb heel rise. Eventually, the pain profile shifts from medial to lateral. This lateral-sided "ankle" pain is typically the result of subfibular and sinus tarsi impingement, a mechanical consequence of the lateral shoulder of the talus abutting the floor of the sinus tarsi and the anterior process of the calcaneus due to severe hindfoot valgus.
Biomechanics of Posterior Tibial Tendon Insufficiency
To master the correction, one must first master the biomechanical failure. In a normal foot, the posterior tibial tendon acts as the primary dynamic inverter of the hindfoot, locking the transverse tarsal joints (talonavicular and calcaneocuboid) during the stance phase to create a rigid lever arm for propulsion. When this tendon fails, the subtalar joint remains everted during the terminal stance. Consequently, the transverse tarsal joints remain unlocked and parallel, leading to a profound loss of structural rigidity in the midfoot. The ground reaction forces then drive the forefoot into abduction and dorsiflexion relative to the hindfoot.
As the deformity becomes more pronounced, the hindfoot shifts lateral to the mechanical axis of the lower extremity. This lateral translation alters the moment arm of the Achilles tendon. The powerful gastrocnemius-soleus complex, which normally acts as a plantarflexor and mild invertor, is converted into a deforming force, acting as a strong hindfoot evertor that exponentially worsens the valgus alignment. Furthermore, the navicular and medial cuneiform displace dorsal to the talar head, leaving the talar head "uncovered" medially and plantarly. The forefoot loses its inherent ability to supinate, leading to a compensatory forefoot varus.
If left untreated, the sinus tarsi completely obliterates, and lateral impingement becomes the dominant clinical complaint. Over time, the peroneus brevis undergoes adaptive shortening and contracture, acting as an unopposed antagonist to the deficient posterior tibial tendon and exacerbating the forefoot abduction. What begins as a supple, flexible, and passively correctable foot gradually transitions into a rigid, irreducible deformity, marking the critical clinical transition from Stage II to Stage III disease. At this advanced stage, joint-sparing procedures like the LCL become contraindicated, necessitating complex, stiffness-inducing arthrodesis procedures such as a triple arthrodesis to restore a plantigrade foot.
Clinical Presentation and Staging
Accurate clinical staging is the bedrock of our surgical decision-making tree. Stage I disease is characterized by tenosynovitis of the posterior tibial tendon without structural deformity; the arch remains intact, and the patient can perform a single heel rise, albeit with pain. Stage II involves a flexible deformity. Stage II is further subdivided: Stage IIa presents with primarily hindfoot valgus and medial arch collapse but minimal forefoot abduction, while Stage IIb is defined by significant forefoot abduction (uncovering of the talar head >40%) and often dictates the necessity of a lateral column lengthening to restore the footprint.
Stage III represents a rigid, non-correctable hindfoot valgus and forefoot abduction, with fixed arthritic changes in the subtalar or transverse tarsal joints. Stage IV, added later to the classification, involves the ankle joint, where deltoid ligament attenuation leads to talar tilt and valgus angulation within the ankle mortise itself. The Evans osteotomy is specifically targeted at Stage IIb deformities. It acts as a structural "kickstand," physically lengthening the lateral border of the foot, which indirectly forces the midfoot out of abduction, covers the talar head, and rotates the hindfoot out of valgus through the intact plantar fascial and ligamentous hinges.
Detailed Surgical Anatomy and Biomechanics
Osteology of the Lateral Column
Before a scalpel is ever passed to the surgeon, a meticulous, three-dimensional understanding of the regional osteology is absolutely paramount. Anatomically and functionally, the lateral column is defined as the contiguous osseous chain comprising the fourth and fifth metatarsals, the cuboid, the calcaneocuboid joint, and the calcaneus. Unlike the relatively rigid medial column, the lateral column is designed for mobility and shock absorption. The calcaneocuboid joint is the primary motion segment of this column, possessing a saddle-shaped articular surface that allows for a complex, multi-planar gliding motion crucial for accommodating uneven terrain.
The calcaneus is the largest tarsal bone and forms the foundation of the heel. Our surgical focus is on its anterior process, a saddle-shaped projection that articulates distally with the cuboid. Just proximal and medial to this process lies the anterior and middle facets of the subtalar joint. The critical radiographic and anatomic landmark here is the angle of Gissane, formed by the intersection of the downward slope of the posterior facet and the upward slope of the anterior process. When performing an Evans osteotomy, the cut must be meticulously placed approximately 1.0 to 1.5 cm proximal to the calcaneocuboid joint line. This precise location is dictated by the need to be distal to the anterior and middle facets to prevent catastrophic iatrogenic intra-articular violation of the subtalar joint.
The cuboid, a wedge-shaped bone, acts as the keystone of the lateral arch. It articulates with the calcaneus posteriorly, the bases of the 4th and 5th metatarsals anteriorly, and the navicular and lateral cuneiform medially. The integrity of the calcaneocuboid joint must be rigorously assessed preoperatively. If the joint exhibits significant degenerative changes, an extra-articular Evans osteotomy may exacerbate the arthritis by increasing joint contact pressures. In such instances, a calcaneocuboid distraction arthrodesis is the preferred alternative to achieve lateral column lengthening while simultaneously ablating the arthritic joint.

Soft Tissue Envelopes and Musculotendinous Units
The soft tissue envelope of the lateral hindfoot is deceptively complex and houses several structures that must be mobilized or protected. Upon incising the skin and subcutaneous tissues, the first major muscular structure encountered is the Extensor Digitorum Brevis (EDB) muscle belly. The EDB originates from the anterior superior surface of the calcaneus, the floor of the sinus tarsi, and the inferior extensor retinaculum. Its muscle belly lies directly superficial to the anterior process of the calcaneus and the calcaneocuboid joint. To achieve adequate osseous exposure for the osteotomy, the origin of the EDB must be sharply elevated off the calcaneus and reflected distally.
Immediately plantar to our surgical field lie the peroneal tendons—the fibularis longus and brevis. These are critical dynamic stabilizers of the lateral column. They course posterior to the lateral malleolus, run along the lateral wall of the calcaneus within their respective sheaths, and pass inferior to the peroneal tubercle. The peroneus brevis inserts on the styloid process of the fifth metatarsal, while the peroneus longus dives into the cuboid groove to cross the plantar aspect of the foot, inserting on the medial cuneiform and first metatarsal base. During the LCL approach, these tendons must be meticulously identified, mobilized, and retracted plantarward. Inadvertent laceration or excessive traction on these tendons can lead to severe postoperative morbidity and failure of the reconstruction.
Furthermore, the lateral capsuloligamentous structures play a vital role in joint stability. The bifurcate ligament, originating from the anterior process of the calcaneus and splitting to attach to the navicular and cuboid, is a key stabilizer of the transverse tarsal joint. While portions of the calcaneocuboid capsule may be released to facilitate distraction, complete transection of the bifurcate ligament should be avoided if possible, as it contributes to the overall stability of the midfoot complex. The plantar fascia, specifically its lateral band, also provides static support to the lateral column and acts as a tension band that is tightened upon lengthening of the calcaneus.


Neurovascular Topography and Danger Zones
The lateral surgical approach to the calcaneus is fraught with neurovascular hazards that demand the utmost respect. The most prominent and frequently injured structure is the sural nerve. This purely sensory nerve provides innervation to the lateral and posterolateral aspect of the distal third of the leg, the lateral heel, and the lateral border of the foot. It typically courses subcutaneously, crossing the lateral border of the Achilles tendon, running posterior and inferior to the lateral malleolus, and continuing distally parallel to the peroneal tendons. The sural nerve is highly variable in its arborization; it frequently gives off lateral calcaneal branches and communicating branches to the intermediate dorsal cutaneous nerve.
During the initial skin incision and subcutaneous dissection, the surgeon must operate with extreme caution. The incision is typically placed just dorsal to the expected course of the sural nerve, but due to anatomic variability, the nerve or its branches may cross directly into the operative field. Meticulous blunt dissection and the use of loupe magnification are strongly recommended. Retraction of the sural nerve should be gentle, utilizing vessel loops rather than rigid metal retractors, to prevent traction neuropraxia or the formation of a painful postoperative neuroma, which can be far more debilitating for the patient than the original flatfoot deformity.
While the sural nerve is the primary concern, the superficial peroneal nerve (specifically its intermediate dorsal cutaneous branch) can also be at risk, particularly if the incision is extended too far dorsally or proximally towards the sinus tarsi. Vascularly, the lateral tarsal artery, a branch of the dorsalis pedis artery, and terminal branches from the peroneal artery supply the lateral foot and the EDB muscle. While major arterial trunks are generally safe during this specific approach, meticulous hemostasis is required to prevent postoperative hematoma, which can compromise wound healing in an area notoriously prone to delayed primary closure and dehiscence due to the expansion of the lateral column.

Exhaustive Indications and Contraindications
Patient Selection Criteria
The decision to proceed with a lateral column lengthening is nuanced and relies on a synthesis of clinical examination and radiographic findings. The ideal candidate is a patient with a Stage IIb acquired flatfoot deformity. This implies a supple, passively correctable hindfoot valgus and, crucially, a significant component of forefoot abduction. Forefoot abduction is clinically visualized as the "too many toes" sign when viewing the patient from behind. Radiographically, it is quantified by an uncovering of the talar head by the navicular of greater than 30-40% on an anteroposterior (AP) weight-bearing view.
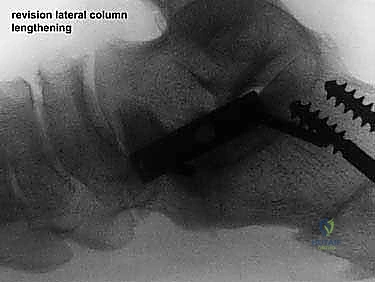
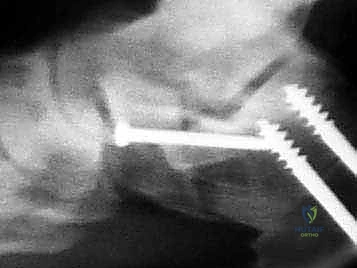
The Evans osteotomy is a powerful tool for triplanar correction. By inserting a structural graft into the anterior calcaneus, we effectively lengthen the lateral column. Due to the intact medial soft tissue hinges (the plantar fascia and medial ligaments), this lengthening forces the navicular to rotate medially back over the talar head, correcting the forefoot abduction. Simultaneously, it plantarflexes the first ray and drives the hindfoot out of valgus and into a more neutral alignment. Therefore, patients who exhibit profound transverse plane dominance in their deformity reap the greatest biomechanical benefit from this specific procedure.
It is rare to perform an Evans osteotomy in isolation. It is almost universally combined with a medializing calcaneal osteotomy (MCO) to correct severe hindfoot valgus, a flexor digitorum longus (FDL) transfer to replace the deficient posterior tibial tendon, and a gastrocnemius recession or Achilles tendon lengthening to address the ubiquitous equinus contracture. The LCL is the structural "heavy lifter" of this reconstructive ensemble, providing the necessary skeletal realignment to protect the soft tissue transfers from premature cyclic failure.
Absolute and Relative Contraindications
Recognizing when not to perform a lateral column lengthening is a hallmark of an experienced foot and ankle surgeon. Absolute contraindications include the presence of a rigid, fixed deformity (Stage III flatfoot). Attempting to lengthen the lateral column in a rigid foot will not result in correction of the deformity; instead, it will dramatically increase the contact pressures across the transverse tarsal and subtalar joints, leading to rapid, catastrophic iatrogenic arthritis and intractable pain. Such patients require corrective arthrodesis.
Another absolute contraindication is the presence of advanced, symptomatic osteoarthritis in the calcaneocuboid or subtalar joints. The Evans osteotomy increases the compressive forces across the calcaneocuboid joint by altering the tension in the lateral band of the plantar fascia and the long plantar ligament. If the joint is already arthritic, this increased pressure will exacerbate symptoms. In these scenarios, if lateral column lengthening is still required to correct forefoot abduction, a calcaneocuboid distraction arthrodesis is the mandated alternative.
Relative contraindications include severe peripheral vascular disease, uncontrolled diabetes mellitus with profound neuropathy, and active local or systemic infection. Furthermore, patients with isolated Stage IIa disease (hindfoot valgus without significant forefoot abduction) may be overcorrected by an Evans osteotomy, leading to a rigid, supinated foot and lateral column overload. In these patients, an isolated medializing calcaneal osteotomy combined with soft tissue reconstruction is often sufficient.
| Category | Specific Condition/Factor | Rationale / Consequence |
|---|---|---|
| Indications | Stage IIb Acquired Flatfoot | Supple deformity with >40% talonavicular uncoverage; ideal for triplanar correction. |
| Indications | Severe Forefoot Abduction | LCL acts as a structural block, physically rotating the midfoot back into alignment. |
| Indications | Failed Conservative Tx | Persistent pain/dysfunction despite >6 months of bracing, orthotics, and physical therapy. |
| Absolute Contraindications | Stage III Rigid Flatfoot | Fixed deformity; lengthening will cause severe iatrogenic joint compression and arthritis. |
| Absolute Contraindications | Calcaneocuboid Arthritis | Increased joint reaction forces post-LCL will exacerbate arthritic pain; requires CC fusion instead. |
| Relative Contraindications | Stage IIa Flatfoot (No Abduction) | Risk of overcorrection into a rigid varus/supinated foot, leading to 5th metatarsal overload. |
| Relative Contraindications | Severe Peripheral Neuropathy | Inability to detect postoperative complications, hardware failure, or pressure ulcerations. |


Pre-Operative Planning, Templating, and Patient Positioning
Radiographic Assessment and Advanced Imaging
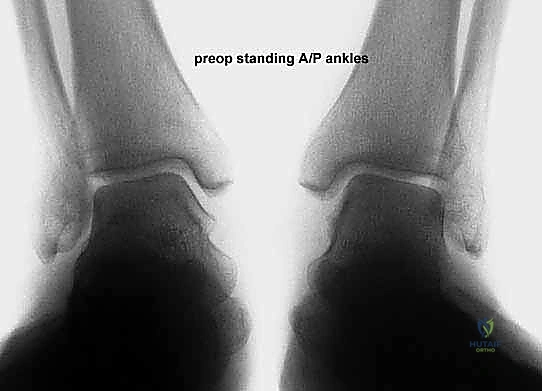
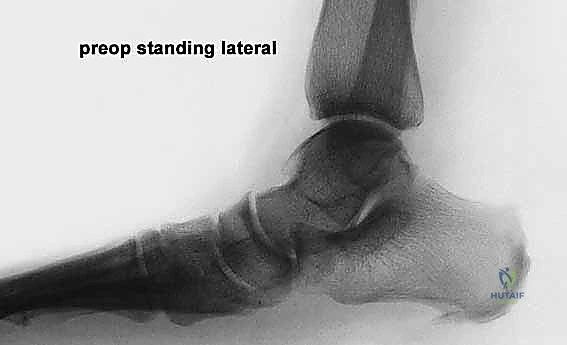
Effective preoperative planning is the absolute cornerstone of a successful surgical outcome. The process begins with obtaining and meticulously analyzing bilateral, weight-bearing foot and ankle radiographs. Non-weight-bearing films are virtually useless for assessing the true magnitude of a dynamic, load-dependent deformity like acquired flatfoot. The standard series must include weight-bearing anteroposterior (AP), lateral, and oblique views of the foot, as well as a standing ankle mortise view.
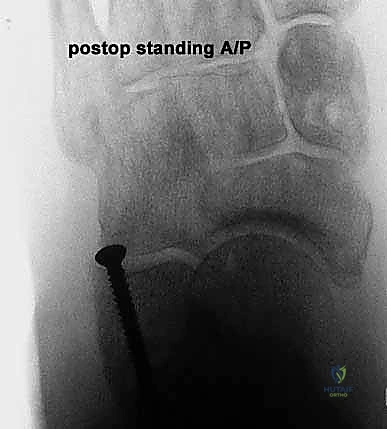
On the lateral radiograph, we evaluate the talo-first metatarsal angle (Meary's angle). In a normal foot, this angle is 0 degrees; the axes of the talus and first metatarsal are colinear. A positive angle indicates a sag of the longitudinal arch at the talonavicular or naviculocuneiform joints. We also assess the calcaneal pitch and the distance from the medial cuneiform to the floor. On the AP view, the critical measurement is the talonavicular coverage angle, which quantifies forefoot abduction. We assess the percentage of the talar head that is uncovered laterally by the navicular. Normal coverage is approximately 70-80%; in severe Stage IIb flatfoot, coverage may drop below 50%. The AP view also allows measurement of the talocalcaneal angle (Kite's angle), which increases as the hindfoot falls into valgus.
While plain radiographs dictate the structural bony plan, Magnetic Resonance Imaging (MRI) is invaluable for assessing the soft tissue envelope. MRI allows for direct visualization of the posterior tibial tendon, identifying tenosynovitis, interstitial tearing, or complete rupture. It also evaluates the integrity of the spring ligament complex, the deltoid ligament, and the presence of bone marrow edema in the lateral column (indicative of sinus tarsi or subfibular impingement). Furthermore, MRI helps rule out other pathologies that can mimic PTTI, such as a spring ligament tear in isolation or inflammatory arthropathies.

Graft Selection and Adjunctive Procedures
A critical preoperative decision is the selection of the interpositional graft material. The options primarily include structural autograft or structural allograft. Historically, tricortical iliac crest autograft was considered the gold standard due to its superior osteoinductive and osteoconductive properties. However, harvesting autograft from the iliac crest is associated with significant donor site morbidity, including chronic pain, hematoma, and lateral femoral cutaneous nerve injury.
Consequently, the paradigm has shifted, and fresh-frozen or freeze-dried structural allograft (typically tricortical iliac crest, patellar wedge, or femoral head allograft) is now our preferred choice. Allograft eliminates donor site morbidity, significantly decreases operative time, and provides excellent structural support. Given the compressive forces across the osteotomy site, allograft incorporation rates are exceptionally high, making the risk-benefit ratio heavily favor allograft in the adult population. Recently, porous titanium wedges have also been introduced as an alternative, offering immediate structural stability without the risk of disease transmission or graft resorption, though long-term data is still evolving.
Surgical planning must also account for the entire reconstructive package. The LCL is rarely an isolated event. If the patient has a fixed equinus contracture (tested via the Silfverskiöld test), a gastrocnemius recession or percutaneous Achilles tendon lengthening is mandatory to relieve the deforming plantarflexion force on the midfoot. If severe hindfoot valgus is present, a medializing calcaneal osteotomy is planned to translate the mechanical axis medially. Finally, a soft tissue procedure, typically an FDL transfer to the navicular and spring ligament imbrication, is planned to restore the dynamic medial restraint.

Operating Room Setup and Patient Positioning
Proper patient positioning and operating room setup are vital for surgical efficiency and optimal visualization. The patient is positioned supine on a standard radiolucent operating table. A crucial step is the placement of a large sandbag or gel bump beneath the ipsilateral hip. Because the lower extremity naturally rests in external rotation, this hip bump internally rotates the limb, bringing the lateral aspect of the foot and ankle into a neutral, highly accessible position for the primary surgeon and the surgical assistant.
A well-padded pneumatic thigh tourniquet is applied to the proximal thigh. A bloodless surgical field is absolutely critical for this procedure. The lateral anatomy is complex, and the sural nerve is easily obscured by bleeding. The tourniquet will be inflated to approximately 250-300 mmHg just prior to the incision, following exsanguination of the limb with an Esmarch bandage.
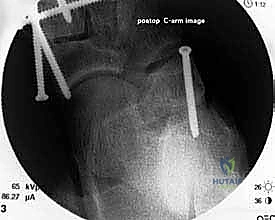
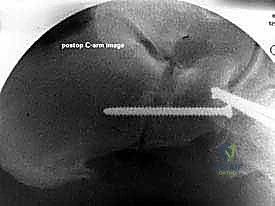
Intraoperative fluoroscopy is indispensable. The C-arm must be draped sterilely and positioned, usually entering from the contralateral side of the table or coming in obliquely from the foot of the bed. The setup must allow for rapid, effortless acquisition of true AP, lateral, and axial views of the calcaneus and midfoot without requiring the surgeon to reposition the patient or awkwardly contort the limb. We routinely verify the fluoroscopic views prior to prepping and draping to ensure the C-arm trajectory is unobstructed by the table pedestal or the contralateral leg.

Step-by-Step Surgical Approach and Fixation Technique
Incision, Exposure, and Soft Tissue Management
With the patient prepped, draped, and the tourniquet inflated, we commence the surgical approach. We utilize a longitudinal lateral incision, approximately 6 to 8 centimeters in length. The incision is centered directly over the calcaneocuboid joint. It extends proximally towards the inferior aspect of the sinus tarsi and distally towards the base of the fourth metatarsal. The trajectory of the incision should be roughly parallel to the plantar border of the foot, ensuring it is perpendicular to the calcaneocuboid joint line.
The skin is incised cleanly with a #15 blade. The superficial subcutaneous dissection must proceed with extreme caution. This is the danger zone for the sural nerve. Using blunt dissection with a hemostat or Stevens tenotomy scissors, we carefully spread the subcutaneous fat. If the sural nerve or a large communicating branch is encountered, it is meticulously mobilized using a vessel loop and gently retracted dorsally or plantarward, depending on its natural course, to keep it completely out of the operative window. Retraction must be gentle to avoid neuropraxia.
Once the neurovascular structures are protected, we identify the deep fascia. We incise the fascia in line with our skin incision to expose the extensor digitorum brevis (EDB) muscle belly. Using electrocautery and a periosteal elevator, the origin of the EDB is sharply elevated off the anterior and lateral aspects of the calcaneus. The muscle belly is reflected distally and dorsally, exposing the underlying calcaneocuboid joint capsule and the lateral wall of the anterior process of the calcaneus. Plantarly, the peroneal tendon sheath is identified but preserved. The peroneal tendons are gently mobilized and retracted inferiorly using a blunt Hohmann retractor. We now have a clear, unobstructed view of the anterior calcaneus and the calcaneocuboid joint.


Osteotomy Execution and Calcaneal Preparation
The next critical step is marking and executing the osteotomy. Localization is everything. We identify the calcaneocuboid joint line by palpation and visually confirming the articular cartilage. A Keith needle or a small K-wire can be placed into the joint to serve as a definitive radiographic and visual marker. The osteotomy site is marked on the lateral wall of the calcaneus exactly 1.0 to 1.5 centimeters proximal to, and strictly parallel with, the calcaneocuboid joint line. This precise measurement ensures we are safely distal to the anterior and middle facets of the subtalar joint.
Using a sagittal saw with a relatively narrow, fine-toothed blade, the osteotomy is initiated
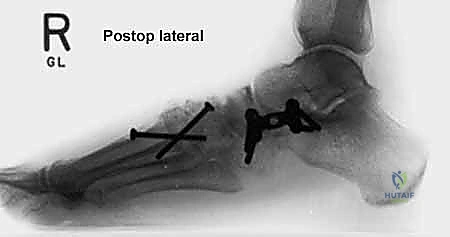
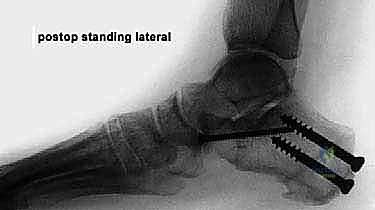
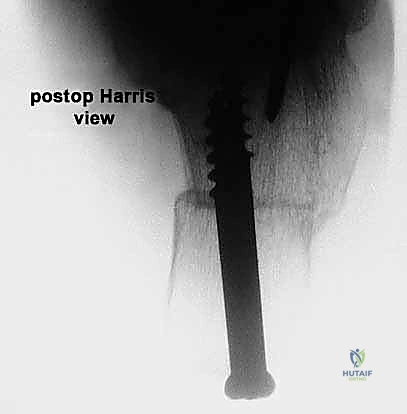
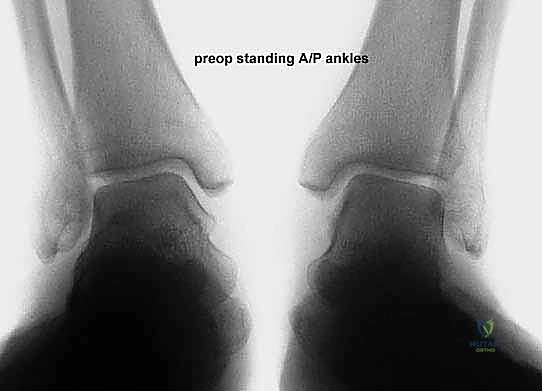
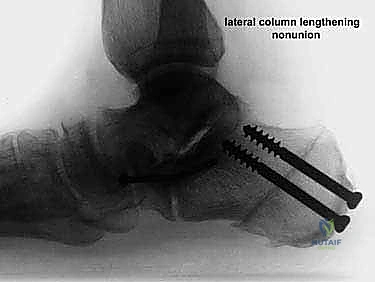
Clinical & Radiographic Imaging Archive