Master ABOS Orthopedic Review: Metabolic Bone, Peds, Ehlers-Danlos, Psoriatic Arthritis | Part 27

Key Takeaway
Ehlers-Danlos Syndrome is a heritable connective tissue disorder characterized by generalized joint hypermobility, skin hyperextensibility, fragility, and easy bruising. It results from a defective Type V collagen protein (COL5A1 mutation). Extraskeletal manifestations include cardiac, respiratory, and neurological complications, with significant phenotypic variability. Surgical challenges involve fragile tissues and delayed wound healing.
Question 1
A 15-month-old infant is brought to the clinic because he is not yet walking and struggles to pull himself to a standing position. His parents also report that he only recently started crawling at 12 months. These delayed motor milestones, along with other skeletal deformities, are common in children with:
View Answer & Explanation
Correct Answer: C
Rationale: Delayed sitting, crawling, and walking are explicitly mentioned as symptoms of rickets in children. The proximal muscle weakness associated with rickets contributes to these motor delays. Main Distractor Rationale: While cerebral palsy and muscular dystrophy can cause delayed motor milestones, the context of "other skeletal deformities" and the overall clinical picture points more specifically to rickets, which directly affects bone development and muscle function due to metabolic derangements.
Question 2
A 65-year-old male presents with chronic back pain and a recent history of a low-energy compression fracture of a lumbar vertebra. Radiographs of the lumbar spine reveal multiple biconcave vertebral bodies and indistinct, blurred trabeculae.

View Answer & Explanation
Correct Answer: C
Rationale: The radiographic findings of fractures, biconcave vertebral bodies, indistinct or blurred trabeculae, and bowing of the endplates are characteristic signs of bone softening and impaired mineralization seen in osteomalacia. Main Distractor Rationale: While osteoporosis can lead to vertebral compression fractures, these are typically wedge-shaped or crush fractures, and the trabeculae, though sparse, are usually distinct. The biconcave shape and blurred trabeculae are more indicative of the bone softening of osteomalacia.
Question 3
A 70-year-old female with a history of malabsorption syndrome presents with severe groin pain after a minor fall. An AP radiograph of the pelvis reveals a fracture of the right pubic bone. Further imaging and workup suggest a weakened pelvic ring due to metabolic bone disease.

View Answer & Explanation
Correct Answer: C
Rationale: The clinical context of malabsorption (a risk factor for vitamin D deficiency and osteomalacia), a low-energy fracture of the pubic bone, and evidence of a weakened pelvic ring are highly suggestive of osteomalacia, often coexisting with osteoporosis (osteoporomalacia) in older adults. The text specifically mentions pubic bone fractures due to a weakened pelvic ring in osteoporomalacia. Main Distractor Rationale: While severe osteoporosis can lead to insufficiency fractures, the underlying malabsorption and the specific mention of a "weakened pelvic ring" in the context of the provided text points more directly to osteomalacia, which often presents with osteoporosis in older patients as "osteoporomalacia."
Question 4
A 40-year-old male presents with progressive muscle weakness, bone pain, and multiple pseudofractures (Looser's zones) on radiographs. Laboratory tests show hypophosphatemia, phosphaturia, and normal serum calcium. Further investigation reveals a small, benign mesenchymal tumor. This presentation is most consistent with:
View Answer & Explanation
Correct Answer: C
Rationale: The combination of osteomalacia symptoms (bone pain, muscle weakness, pseudofractures), hypophosphatemia, phosphaturia, and the presence of a tumor (often mesenchymal) is characteristic of oncogenic osteomalacia. This condition is caused by tumors that secrete fibroblast growth factor 23 (FGF23), leading to renal phosphate wasting and impaired vitamin D activation. Main Distractor Rationale: While vitamin D deficiency osteomalacia shares many symptoms, the specific findings of hypophosphatemia, phosphaturia, normal serum calcium, and the presence of a tumor distinguish oncogenic osteomalacia from simple nutritional vitamin D deficiency.
Question 5
A 75-year-old female is diagnosed with a metabolic bone disorder. Her bone mineral density (BMD) T-score is -3.0 at the hip, indicating osteoporosis. Additionally, a bone biopsy shows evidence of impaired mineralization. The coexistence of these two conditions is best described as:
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that "Very often the osteomalacia and the osteoporosis are together" and refers to this combined condition as "osteoporomalacia." This term accurately describes the coexistence of reduced bone mass (osteoporosis) and impaired bone mineralization (osteomalacia). Main Distractor Rationale: Osteopenia refers to bone density that is lower than normal but not as severe as osteoporosis (T-score between -1.0 and -2.5). It does not specifically imply a mineralization defect, which is central to osteomalacia.
Question 6
A 2-year-old boy with rickets demonstrates characteristic cupping and fraying of the metaphyseal region of the wrist on initial radiographs. After 1 year of adequate vitamin D substitution treatment, follow-up radiographs are obtained.

View Answer & Explanation
Correct Answer: C
Rationale: The provided image and text (Fig. 7.34 c) clearly demonstrate that after 1 year of adequate substitution vitamin-D treatment, there is significant improvement in the characteristic radiological appearance of rickets at the wrist, including resolution of cupping and fraying. This indicates the effectiveness of treatment in promoting mineralization. Main Distractor Rationale: Worsening of metaphyseal cupping and fraying would indicate treatment failure or progression of the disease, which is contrary to the expected outcome of adequate vitamin D substitution.
Question 7
A 50-year-old male is diagnosed with osteomalacia secondary to chronic kidney disease. The primary metabolic derangement directly leading to the insufficient mineralization of bone in this patient is:
View Answer & Explanation
Correct Answer: B
Rationale: The text states that osteomalacia "is caused by a deficiency of vitamin D, which reduces bone formation by altering calcium and phosphorus metabolism." Regardless of the underlying cause (vitamin D deficiency, renal disorders, etc.), the final common pathway leading to insufficient mineralization is the disruption of calcium and phosphorus homeostasis, which are essential for bone mineralization. Main Distractor Rationale: While excessive parathyroid hormone secretion can occur in chronic kidney disease (secondary hyperparathyroidism) and contribute to bone disease (renal osteodystrophy), the direct mechanism for insufficient mineralization in osteomalacia is the altered calcium and phosphorus metabolism, which PTH dysregulation can exacerbate but is not the sole primary derangement causing the mineralization defect itself.
Question 8
A 3-year-old child presents with a waddling gait and difficulty climbing stairs. Physical examination reveals proximal muscle weakness and bowing of the legs. These findings, in the context of skeletal deformities, suggest:
View Answer & Explanation
Correct Answer: C
Rationale: Proximal muscle weakness, bowing of the legs, and bone pain are explicitly listed as characteristics of rickets in children. The waddling gait and difficulty climbing stairs are direct consequences of proximal muscle weakness. Main Distractor Rationale: While Duchenne muscular dystrophy also causes progressive proximal muscle weakness and a waddling gait, it is a primary muscle disorder without the characteristic skeletal deformities (like bowing of legs) or the underlying mineralization defect seen in rickets.
Question 9
A 78-year-old female patient is evaluated for chronic back pain and progressive stooping. Clinical examination reveals significant kyphosis and a noticeable loss of height. Her abdomen appears bulging. These clinical features are consistent with advanced:

View Answer & Explanation
Correct Answer: B
Rationale: The clinical description of loss of height, kyphosis, and a bulging abdomen in an elderly female is specifically highlighted in the text and image (Fig. 7.36) as characteristic of osteoporomalacia. These features result from vertebral compression fractures and spinal deformities caused by weakened, poorly mineralized bone. Main Distractor Rationale: While spondylolisthesis can cause back pain, it does not typically present with generalized loss of height, kyphosis, and a bulging abdomen as primary features of the condition itself, nor does it involve the systemic bone softening seen in osteoporomalacia.
Question 10
A 6-month-old infant presents with delayed motor development and bowing of the legs. A 40-year-old adult presents with diffuse bone pain and muscle weakness. Both patients are diagnosed with a disease characterized by insufficient mineralization of bone. The term used to distinguish the disease in the infant from that in the adult is:
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "This disease [osteomalacia] causes the bending and misshaping of bones, such as bow-legging of the lower limbs, and is called rickets when it occurs in children." Rickets is essentially osteomalacia occurring before epiphyseal closure, affecting growth plates. Main Distractor Rationale: Osteoporosis is a distinct condition characterized by reduced bone mass but normal mineralization, and it is not the term used to differentiate osteomalacia in children from adults.
Question 11
A 55-year-old female is diagnosed with osteomalacia. Her physician is investigating the cause. Which of the following is NOT listed as a common cause of vitamin D deficiency leading to osteomalacia?
View Answer & Explanation
Correct Answer: D
Rationale: The text lists reduced exposure to sunlight, insufficient intake of vitamin D-enriched foods, and improper digestion and absorption of food with vitamin D as common causes of vitamin D deficiency. Renal tubular disorders (like Fanconi's syndrome) are also mentioned as a cause of osteomalacia, but they are not a cause of vitamin D *deficiency* itself, rather a cause of phosphate wasting leading to osteomalacia. Excessive intake of calcium supplements is not listed as a cause of vitamin D deficiency or osteomalacia; in fact, calcium is often supplemented in treatment. Main Distractor Rationale: Renal tubular disorders are a cause of osteomalacia, but not by causing vitamin D *deficiency*. They cause phosphate wasting, which leads to impaired mineralization. However, the question specifically asks for what is NOT a cause of vitamin D deficiency leading to osteomalacia. Excessive calcium intake is the most incorrect option as it does not cause vitamin D deficiency or osteomalacia.
Question 12
A 48-year-old male presents with chronic, widespread bone pain that is described as a dull ache, particularly in the spine, pelvis, and lower extremities. He also reports general malaise and easy fatigability. These symptoms, when delayed until the disorder has advanced, are characteristic of:
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that in adults, symptoms of osteomalacia are "often delayed until the disorder has advanced. These include easy fatigability, malaise, diffuse bone pain, and spasms." This directly matches the clinical vignette. Main Distractor Rationale: Fibromyalgia is characterized by widespread musculoskeletal pain, fatigue, and tenderness in specific points, but it is a soft tissue pain disorder and does not involve the underlying bone softening or specific radiographic findings of osteomalacia.
Question 13
A 3-month-old female infant is brought to the clinic for a routine check-up. On physical examination, the pediatrician notes asymmetric thigh skin folds and a positive Ortolani maneuver on the right hip. The left hip examination is normal. Radiographs are ordered.
View Answer & Explanation
Correct Answer: C
Rationale: For infants younger than 4-6 months, the femoral head and acetabulum are largely cartilaginous and not well visualized on plain radiographs. Ultrasound is the preferred imaging modality for diagnosing developmental dysplasia of the hip (DDH) in this age group as it allows for dynamic assessment of hip stability and visualization of cartilaginous structures. AP pelvis radiographs are less reliable in this age group due to poor ossification. CT and MRI are typically reserved for more complex cases or pre-operative planning.
Question 14
A newborn male is diagnosed with congenital talipes equinovarus (CTEV), or clubfoot, of the right foot. The foot demonstrates equinus, varus, adduction, and cavus, which cannot be passively corrected. The infant is otherwise healthy.
View Answer & Explanation
Correct Answer: C
Rationale: The Ponseti method, involving serial manipulation and casting, is the gold standard for initial treatment of idiopathic clubfoot. It is highly successful in achieving correction without surgery in the majority of cases. Immediate surgical correction is typically reserved for failed conservative treatment or complex cases. Static bracing and physical therapy alone are insufficient for correcting the rigid deformities of clubfoot. Observation is inappropriate as early intervention is crucial for optimal outcomes.
Question 15
A 6-year-old male presents with a 3-month history of a painless limp and occasional right knee pain. On examination, he has limited internal rotation and abduction of the right hip. Radiographs of the hip show increased density and fragmentation of the right femoral epiphysis, with widening of the joint space.
View Answer & Explanation
Correct Answer: D
Rationale: The clinical presentation (age, painless limp, limited hip motion) and radiographic findings (increased density, fragmentation of the femoral epiphysis, widening of the joint space) are classic for Legg-Calvé-Perthes disease, which is idiopathic avascular necrosis of the femoral head. SCFE typically occurs in older, obese adolescents. Septic arthritis and transient synovitis usually present with acute, painful symptoms. JIA would likely have more systemic symptoms and different radiographic findings.
Question 16
A 13-year-old obese male presents to the emergency department with a 2-week history of left knee pain and a progressive limp. He denies trauma. On examination, his left leg is externally rotated, and he has significantly limited internal rotation and abduction of the left hip. Radiographs show a posterior and inferior displacement of the capital femoral epiphysis relative to the femoral neck.
View Answer & Explanation
Correct Answer: D
Rationale: This patient has a stable Slipped Capital Femoral Epiphysis (SCFE). The most appropriate immediate management is in situ percutaneous pinning to stabilize the physis and prevent further slippage. Weight-bearing is contraindicated. NSAIDs and physical therapy do not address the mechanical instability. Spica casting is not effective for SCFE. Open reduction is generally reserved for unstable slips or severe deformity after pinning, due to higher risks of avascular necrosis.
Question 17
A 2-year-old obese African American boy is brought to the clinic by his parents due to progressive bowing of his right lower leg. The bowing has worsened over the past 6 months. Physical examination reveals a prominent varus deformity of the right tibia. Radiographs show medial metaphyseal beaking, fragmentation, and depression of the medial tibial epiphysis.
View Answer & Explanation
Correct Answer: C
Rationale: The patient's age (toddler), obesity, race, progressive unilateral bowing, and characteristic radiographic findings (medial metaphyseal beaking, fragmentation, and depression of the medial tibial epiphysis) are highly suggestive of Blount's disease (tibia vara). Physiologic genu varum is typically bilateral, resolves spontaneously, and lacks these specific radiographic changes. Rickets would show more generalized growth plate abnormalities and often other systemic signs. A physeal bar would result from trauma or infection, and an osteochondroma would present as a distinct bony mass.
Question 18
A 7-year-old girl presents with a 6-month history of progressive scoliosis. Her physical exam reveals a right thoracic curve with a rib hump on forward bending. Radiographs show a 35-degree right thoracic curve with a hemivertebra at T8. The remaining spine appears normal.
View Answer & Explanation
Correct Answer: C
Rationale: The presence of a hemivertebra at T8 is a congenital vertebral anomaly, which is the hallmark of congenital scoliosis. This type of scoliosis is caused by malformations of the vertebrae during embryonic development. Idiopathic scoliosis has no identifiable cause and typically presents in adolescence without vertebral anomalies. Neuromuscular scoliosis is associated with underlying neurological or muscular conditions. Scheuermann's kyphosis involves wedging of multiple vertebral bodies and endplate irregularities, primarily affecting the sagittal plane. Postural scoliosis is non-structural and corrects with positioning.
Question 19
A 1-month-old infant is noted to have a persistent head tilt to the right and difficulty turning her head to the left. Palpation of the left sternocleidomastoid muscle reveals a firm, non-tender mass. There is no history of trauma or infection.
View Answer & Explanation
Correct Answer: B
Rationale: The classic presentation of congenital muscular torticollis includes a head tilt, limited range of motion of the neck, and often a palpable mass (fibromatosis colli) in the sternocleidomastoid muscle, typically appearing between 2-4 weeks of age. Klippel-Feil syndrome involves congenital fusion of cervical vertebrae and would present with a short neck and limited motion, but not typically a sternocleidomastoid mass. Atlantoaxial rotatory subluxation is usually acute and painful. Brachial plexus injury would manifest with arm weakness. Sandifer syndrome is associated with gastroesophageal reflux and dystonic posturing.
Question 20
A 10-year-old boy with a known history of osteogenesis imperfecta (OI) presents with acute pain and deformity of his right forearm after a minor fall. Radiographs confirm a displaced fracture of the radius and ulna. He has a history of multiple previous fractures, blue sclera, and hearing loss.
View Answer & Explanation
Correct Answer: B
Rationale: For an acute fracture in a patient with OI, the immediate management is immobilization, similar to other fractures. However, given the underlying genetic disorder, referral for genetic counseling is crucial for family planning and understanding the disease. Bisphosphonates are used to increase bone density and reduce fracture rates in OI, but are not the primary acute treatment for a fracture. Open reduction and internal fixation may be necessary for complex fractures but is not the initial universal step. Vitamin D and calcium are important for bone health but not specific to OI. Growth hormone is not indicated for OI.
Question 21
A 4-year-old boy presents with a progressive flatfoot deformity. On examination, his foot is rigid, and he has limited subtalar motion. Radiographs show a bony bridge between the talus and calcaneus.
View Answer & Explanation
Correct Answer: C
Rationale: The combination of a rigid flatfoot, limited subtalar motion, and a bony bridge between the talus and calcaneus on radiographs is diagnostic of a tarsal coalition, specifically a talocalcaneal coalition in this case. Flexible flatfoot is typically asymptomatic and corrects with toe-standing. Congenital vertical talus presents with a "rocker-bottom" foot and dorsal dislocation of the navicular. An accessory navicular is a separate ossicle and typically causes medial foot pain, not rigid flatfoot. Charcot-Marie-Tooth disease is a neurological condition that can cause foot deformities but would not show a bony coalition.
Question 22
A 15-year-old male presents with a history of tall stature, long slender limbs, arachnodactyly, and pectus excavatum. He reports recent onset of low back pain. On examination, he has hypermobility of joints and a positive thumb sign and wrist sign. Radiographs of the spine show mild scoliosis.
View Answer & Explanation
Correct Answer: C
Rationale: The constellation of tall stature, long slender limbs (arachnodactyly), pectus excavatum, joint hypermobility, and positive thumb/wrist signs are classic features of Marfan syndrome, a connective tissue disorder. Ehlers-Danlos syndrome also involves joint hypermobility and skin laxity but typically lacks the specific skeletal features like arachnodactyly and ocular/cardiac manifestations of Marfan. Homocystinuria shares some features but has distinct metabolic abnormalities. Achondroplasia causes short stature and disproportionate dwarfism. Klinefelter syndrome affects males with an extra X chromosome and has different phenotypic features.
Question 23
A 9-year-old boy with neurofibromatosis type 1 (NF1) presents with progressive bowing and shortening of his right tibia. Radiographs show anterior bowing, cortical thickening, and a narrow medullary canal, with an area of lucency suggesting a pseudarthrosis. He has multiple café-au-lait spots and axillary freckling.
View Answer & Explanation
Correct Answer: B
Rationale: Congenital pseudarthrosis of the tibia (CPT) is a rare but well-recognized complication of neurofibromatosis type 1 (NF1). The clinical presentation of progressive bowing, shortening, and radiographic findings of anterior bowing, cortical thickening, and pseudarthrosis in a patient with NF1 is highly characteristic of CPT. Physiologic bowing resolves spontaneously. Blount's disease affects the proximal tibia and has distinct radiographic features. Fibrous dysplasia can cause bowing but typically presents differently and is not directly linked to NF1 in this manner. Rickets would show generalized growth plate abnormalities.
Question 24
A 5-year-old boy with achondroplasia presents with progressive lower extremity weakness, gait disturbance, and hyperreflexia. He has a history of disproportionate short stature, macrocephaly, and midface hypoplasia. MRI of the spine is ordered.
View Answer & Explanation
Correct Answer: C
Rationale: Patients with achondroplasia are at increased risk for neurological complications, most notably foramen magnum stenosis due to abnormal endochondral ossification at the skull base. This can lead to compression of the cervicomedullary junction, causing myelopathy, lower extremity weakness, hyperreflexia, and gait disturbance. Spinal muscular atrophy is a genetic neuromuscular disorder. Tethered cord syndrome is associated with spina bifida. Lumbar disc herniation is less common in this age group and typically presents with radicular pain. Syringomyelia is a fluid-filled cyst within the spinal cord.
Question 25
A 1-year-old girl is diagnosed with a congenital radial club hand (radial longitudinal deficiency) of her left arm. She has significant radial deviation of the wrist and shortening of the forearm. Her thumb is hypoplastic. She has no other apparent anomalies.
View Answer & Explanation
Correct Answer: E
Rationale: Radial longitudinal deficiency (radial club hand) is frequently associated with other congenital anomalies and syndromes. It is crucial to screen for these conditions. VACTERL association (Vertebral, Anorectal, Cardiac, Tracheoesophageal, Renal, Limb) can include radial ray defects. Holt-Oram syndrome involves cardiac defects and upper limb anomalies. Fanconi anemia is a bone marrow failure syndrome with radial ray defects. TAR syndrome is characterized by thrombocytopenia and bilateral absence of the radius. Therefore, all listed options represent conditions that should be considered and screened for in a patient with radial club hand.
Question 26
A 14-year-old girl presents with a 45-degree right thoracic idiopathic scoliosis. She has reached skeletal maturity (Risser 5) and has no neurological deficits. She reports mild back pain but is otherwise asymptomatic.
View Answer & Explanation
Correct Answer: C
Rationale: For skeletally mature adolescents with idiopathic scoliosis, a curve greater than 40-45 degrees is generally an indication for surgical correction (spinal fusion) to prevent further progression and improve cosmetic appearance. Observation is for smaller curves or those with minimal progression. Bracing is effective for curves between 25-45 degrees in skeletally immature patients to prevent progression, but it is not effective once skeletal maturity is reached. Physical therapy and NSAIDs can help with symptoms but do not correct the curve.
Question 27
A 6-month-old infant is diagnosed with congenital vertical talus (CVT), also known as "rocker-bottom foot." On examination, the foot is rigid, dorsiflexed, and the navicular is dorsally dislocated on the talus. Radiographs confirm the characteristic findings.
View Answer & Explanation
Correct Answer: C
Rationale: Congenital vertical talus is a rigid deformity that typically requires surgical correction. While some attempts at serial casting may be made, definitive correction usually involves extensive soft tissue release (including the Achilles tendon, peroneal tendons, and often the posterior capsule) and reduction of the talonavicular joint, followed by pinning. Observation, orthotics, or physical therapy alone are insufficient for correcting this rigid deformity. Serial casting is the primary treatment for clubfoot, not CVT.
Question 28
A 2-year-old boy presents with a history of a short, webbed neck, low posterior hairline, and limited cervical range of motion. Radiographs of the cervical spine show fusion of multiple cervical vertebrae.
View Answer & Explanation
Correct Answer: B
Rationale: The classic triad of Klippel-Feil syndrome includes a short neck, low posterior hairline, and limited cervical range of motion, caused by congenital fusion of two or more cervical vertebrae. Sprengel's deformity is a congenital elevation of the scapula. Congenital muscular torticollis involves the sternocleidomastoid muscle. Cervical spondylosis is a degenerative condition in adults. Neurofibromatosis type 1 has different skeletal manifestations and is not characterized by cervical vertebral fusion as a primary feature.
Question 29
A 1-month-old infant is found to have polydactyly of the right hand, specifically an extra digit on the ulnar side (postaxial polydactyly). The extra digit is small, rudimentary, and attached by a narrow pedicle.
View Answer & Explanation
Correct Answer: B
Rationale: For a rudimentary postaxial polydactyly (Type A or B) attached by a narrow pedicle, simple ligation at the base of the pedicle is often sufficient. This procedure can be performed in the nursery or early infancy, allowing the digit to necrose and fall off. Surgical excision is reserved for more complex or well-formed digits. Observation is not appropriate as the extra digit can cause functional issues or be unsightly. While genetic workup may be considered for complex or syndromic cases, simple postaxial polydactyly is often isolated. Physical therapy is not indicated for a rudimentary digit.
Question 30
A 16-year-old male presents with a painful bony mass on the medial aspect of his distal femur. He reports the mass has been slowly growing for several years and is now causing pain with activity. Radiographs show a sessile osteochondroma extending away from the joint, with continuity of the cortex and medulla with the parent bone. He has multiple similar lesions elsewhere.
View Answer & Explanation
Correct Answer: C
Rationale: The presence of multiple osteochondromas, particularly with a history of slow growth and pain, is characteristic of Multiple Hereditary Exostoses (MHE), an autosomal dominant disorder. A solitary osteochondroma would only involve one lesion. Enchondromas are cartilaginous tumors within the bone. Osteosarcoma is a malignant bone tumor with aggressive features. Fibrous dysplasia is a developmental anomaly where normal bone is replaced by fibrous tissue. The key here is "multiple similar lesions elsewhere," pointing to MHE.
Question 31
A 4-year-old boy with spina bifida and a myelomeningocele at L3-L4 level presents with progressive hip dislocation. On examination, he has paralysis of the quadriceps and ankle dorsiflexors, but intact hip flexors and adductors. Radiographs confirm bilateral hip dislocation.
View Answer & Explanation
Correct Answer: D
Rationale: In patients with spina bifida and paralytic hip dislocation, the imbalance of muscle forces (strong hip flexors/adductors and weak abductors/extensors) is a primary cause. Surgical management often involves soft tissue releases (e.g., adductor and iliopsoas release) and tendon transfers (e.g., external oblique to greater trochanter) to rebalance the hip musculature and facilitate reduction. Open reduction and osteotomies (C and E) may be necessary in some cases, but addressing the muscle imbalance with soft tissue procedures is often a crucial initial or concomitant step. Observation and bracing are generally ineffective for established paralytic dislocations. The goal is often to achieve stable, functional hips, not necessarily anatomical reduction at all costs, especially if ambulation is not expected.
Question 32
A 1-year-old male infant presents with a short left femur and a significant discrepancy in leg length. Radiographs show a hypoplastic left femur with a deficient proximal segment, consistent with Proximal Femoral Focal Deficiency (PFFD). The foot and ankle appear normal.
View Answer & Explanation
Correct Answer: C
Rationale: Management of PFFD depends on the severity of the deficiency and the expected leg length discrepancy. For a significant discrepancy, limb lengthening procedures (e.g., using external fixators) are often considered to equalize leg length and improve function. Immediate prosthetic fitting might be considered for very severe cases or after limb lengthening. Amputation of the foot is typically reserved for cases where the foot is severely deformed or non-functional, often as part of a Syme's amputation to facilitate prosthetic fitting. Observation alone is insufficient for significant discrepancies. Hip reconstruction may be part of a broader surgical plan but is not the primary intervention for leg length discrepancy.
Question 33
A 3-month-old female infant presents for a routine check-up. Physical examination reveals asymmetric thigh folds and a positive Ortolani click on the right hip. Radiographs show a shallow right acetabulum and a superolateral displacement of the right femoral head. The left hip appears normal.
View Answer & Explanation
Correct Answer: B
Rationale: This presentation is classic for developmental dysplasia of the hip (DDH) in an infant under 6 months of age. A Pavlik harness is the treatment of choice for reducible hips in this age group, aiming to maintain the hip in flexion and abduction to promote acetabular development. Observation is inappropriate for a dislocated hip. Spica cast or surgical interventions are reserved for older infants, failed Pavlik harness treatment, or irreducible dislocations.
Question 34
A 12-year-old obese male presents with a 3-month history of left hip and knee pain, worse with activity. He walks with an antalgic gait and holds his left leg in external rotation. Physical examination reveals limited internal rotation and abduction of the left hip. Radiographs of the pelvis show a posterior and inferior displacement of the left capital femoral epiphysis relative to the metaphysis.
View Answer & Explanation
Correct Answer: B
Rationale: This is a classic presentation of a stable slipped capital femoral epiphysis (SCFE). The treatment of choice for stable SCFE is in situ pinning with a single screw to prevent further slippage and promote physeal closure. Non-weight-bearing alone is insufficient. Open reduction is typically reserved for unstable SCFE or severe slips. Osteotomy is considered for residual deformity after pinning or for severe chronic slips. Total hip arthroplasty is a salvage procedure for severe complications like avascular necrosis or advanced degenerative changes.
Question 35
A 6-year-old boy presents with a 6-month history of a painless limp. Physical examination reveals a Trendelenburg gait and limited abduction and internal rotation of the right hip. Radiographs show increased density and fragmentation of the right femoral head epiphysis, with widening of the medial joint space.
View Answer & Explanation
Correct Answer: B
Rationale: This clinical picture is consistent with Legg-Calvé-Perthes disease. The goal of treatment is to maintain containment of the femoral head within the acetabulum to preserve its spherical shape during revascularization and remodeling. Bracing (e.g., Scottish Rite brace) or osteotomies (femoral or pelvic) are used for containment, depending on the age and severity. Activity restriction and observation may be appropriate for very mild cases or younger children, but bracing is often indicated for more significant involvement. Core decompression is for avascular necrosis in adults, not Perthes. Total hip arthroplasty is a salvage procedure for end-stage disease. Bisphosphonates are not a primary treatment for Perthes.
Question 36
A newborn male is noted to have a foot deformity characterized by equinus of the ankle, varus of the hindfoot, adduction of the forefoot, and cavus. The foot is rigid and cannot be passively corrected to a neutral position. The remainder of the physical examination is unremarkable.
View Answer & Explanation
Correct Answer: A
Rationale: This is a classic presentation of congenital talipes equinovarus (CTEV), or clubfoot. The Ponseti method, involving serial manipulation and casting, is the gold standard for initial treatment, with a high success rate. Surgical release is typically reserved for failed Ponseti treatment or recurrent deformities. Custom orthotics and AFOs are used for maintenance after correction, not as primary treatment. Observation and stretching are insufficient for a rigid clubfoot.
Question 37
A 2-year-old boy presents with progressive bowing of his right lower leg. His parents report he started walking at 12 months, and the bowing has become more noticeable since then. Physical examination reveals a sharp, angular deformity of the proximal right tibia, with medial metaphyseal beaking. Radiographs confirm the severe varus deformity and show fragmentation and sclerosis of the medial proximal tibial physis.
View Answer & Explanation
Correct Answer: C
Rationale: This presentation is characteristic of Blount's disease (tibia vara), specifically infantile Blount's, given the age and severity. Physiologic bowing typically resolves by 2 years of age and does not show the characteristic radiographic changes. Bracing can be attempted in very early or mild cases, but for progressive or severe deformity in a 2-year-old, a proximal tibial osteotomy is often required to correct the alignment. Distal femoral osteotomy is incorrect as the deformity is tibial. Hemiepiphysiodesis is typically used for older children with less severe or progressive deformities, not for the acute angular deformity seen in infantile Blount's.
Question 38
A 4-week-old infant presents with a head tilt to the right and difficulty turning her head to the left. Physical examination reveals a palpable mass in the middle third of the left sternocleidomastoid muscle. Passive range of motion shows limited rotation and lateral flexion of the cervical spine.
View Answer & Explanation
Correct Answer: B
Rationale: This is a classic presentation of congenital muscular torticollis. The initial treatment of choice, especially in infants diagnosed early, is physical therapy focusing on stretching exercises to lengthen the sternocleidomastoid muscle and strengthen the contralateral neck muscles. Surgical release is reserved for cases that fail conservative management after 6-12 months or for severe fixed deformities. Observation alone is insufficient. Cervical collar immobilization is not indicated. Botulinum toxin injection is not a primary treatment for congenital muscular torticollis in infants.
Question 39
A 10-year-old girl with a history of recurrent fractures from minor trauma presents with a new forearm fracture. She has blue sclerae, hearing loss, and dental abnormalities. Radiographs show generalized osteopenia and multiple healed fractures in various stages of remodeling.
View Answer & Explanation
Correct Answer: B
Rationale: This patient's presentation (recurrent fractures, blue sclerae, hearing loss, dental abnormalities, osteopenia) is highly suggestive of Osteogenesis Imperfecta (OI). While genetic counseling is important, the primary medical management to reduce fracture frequency and improve bone density is bisphosphonate therapy. Calcium and Vitamin D are supportive but not primary treatments for OI. Growth hormone is not indicated. Surgical stabilization is for acute fractures, not a general preventative measure for all bones. Genetic counseling is crucial but not the sole management.
Question 40
A 14-year-old boy presents with progressive back pain and increasing truncal asymmetry. Physical examination reveals a significant right thoracic curve with a rib hump on forward bending. Radiographs show a 55-degree right thoracic curve with apical vertebral rotation and no evidence of congenital vertebral anomalies.
View Answer & Explanation
Correct Answer: C
Rationale: This patient has adolescent idiopathic scoliosis (AIS) with a curve magnitude of 55 degrees. For AIS, curves greater than 45-50 degrees in skeletally immature or mature patients are typically indications for surgical correction (spinal fusion) to prevent further progression and improve alignment. Observation is for curves less than 20-25 degrees. Bracing is for progressive curves between 25-45 degrees in skeletally immature patients. Physical therapy and chiropractic manipulation have not been shown to alter the natural history of progressive AIS.
Question 41
A 3-year-old child with achondroplasia presents with progressive lower extremity weakness, hyperreflexia, and clonus. MRI of the cervical spine reveals severe cervicomedullary junction compression due to a narrowed foramen magnum.
View Answer & Explanation
Correct Answer: C
Rationale: Achondroplasia is characterized by disproportionate short stature and can lead to complications like cervicomedullary junction compression due to a small foramen magnum. The presented neurological symptoms (weakness, hyperreflexia, clonus) indicate significant spinal cord compression, which is a neurosurgical emergency. Surgical posterior fossa decompression is indicated to relieve the compression and prevent irreversible neurological damage. Observation, physical therapy, or bracing are insufficient for symptomatic cord compression. Genetic counseling is important for the family but does not address the acute neurological issue.
Question 42
A 7-year-old boy presents with a 6-month history of progressive flatfoot deformity. His parents note that his foot remains flat even when standing on tiptoes. Physical examination reveals a rigid, painful flatfoot with a prominent bulge on the medial aspect of the foot, just anterior to the medial malleolus. Radiographs show a talonavicular coalition.
View Answer & Explanation
Correct Answer: C
Rationale: This presentation is classic for a symptomatic rigid flatfoot due to a tarsal coalition, specifically a talonavicular coalition. The inability to form an arch on tiptoes is a key sign of rigidity. For symptomatic tarsal coalitions, surgical resection of the bar is the treatment of choice, especially for cartilaginous or fibrous coalitions, to restore motion and relieve pain. Arch supports and NSAIDs may provide temporary symptomatic relief but do not address the underlying structural problem. Triple arthrodesis is a salvage procedure for severe, degenerative, or failed resections. Serial casting is not effective for rigid tarsal coalitions.
Question 43
A 1-year-old child presents with a congenital absence of the radius, resulting in a severely radially deviated hand and forearm shortening. The thumb is also hypoplastic. The child has no other obvious systemic anomalies.
View Answer & Explanation
Correct Answer: C
Rationale: This describes radial club hand (radial longitudinal deficiency). The primary goal of treatment is to improve wrist alignment and function. Centralization (or radialization) of the wrist is the most common surgical procedure, typically performed between 6-12 months, to align the hand with the ulna. Pollicization is for thumb hypoplasia, which may be performed concurrently or subsequently. Observation and stretching are insufficient for severe deformities. Ulnar lengthening is not the primary procedure for radial club hand. It's important to rule out associated syndromes (e.g., VACTERL, Holt-Oram) with systemic workup.
Question 44
A 5-year-old boy presents with a history of recurrent dislocations of the patella. Physical examination reveals generalized ligamentous laxity, a high-riding patella (patella alta), and a positive J-sign. Radiographs show trochlear dysplasia and an increased tibial tubercle-trochlear groove (TT-TG) distance.
View Answer & Explanation
Correct Answer: B
Rationale: Recurrent patellar dislocations in a child with patella alta, trochlear dysplasia, and increased TT-TG distance indicate significant patellofemoral instability. MPFL reconstruction is a common and effective surgical procedure to stabilize the patella by restoring the primary medial restraint. Quadriceps strengthening is important but often insufficient for recurrent dislocations with significant anatomical abnormalities. Lateral retinacular release alone is rarely indicated and can worsen instability. Tibial tubercle osteotomy may be combined with MPFL reconstruction, especially for a significantly increased TT-TG distance, but MPFL reconstruction addresses the primary ligamentous deficiency. Total knee arthroplasty is not indicated in a 5-year-old.
Question 45
A 1-month-old infant is noted to have a foot deformity where the entire sole of the foot is convex, resembling a "rocker-bottom" foot. The hindfoot is in equinus, and the forefoot is dorsiflexed. The deformity is rigid and irreducible. Radiographs show a vertical talus.
View Answer & Explanation
Correct Answer: C
Rationale: This describes congenital vertical talus (CVT), also known as congenital convex pes valgus. It is a rigid flatfoot deformity. Unlike clubfoot, the Ponseti method alone is usually insufficient. The preferred treatment involves an initial period of serial casting (reverse Ponseti method) to stretch the soft tissues, followed by surgical correction to reduce the talonavicular joint and stabilize the foot. Observation, stretching, or custom orthotics are ineffective for this rigid deformity. Immediate surgery without casting is less common and may be more challenging due to soft tissue contractures.
Question 46
A 9-year-old boy presents with a 3-month history of worsening pain and swelling in his right knee. Physical examination reveals warmth, effusion, and limited range of motion in the knee. Laboratory tests show elevated ESR and CRP. Radiographs show soft tissue swelling and joint space widening, with no clear evidence of fracture or infection. He has a history of similar symptoms in his left ankle a year prior.
View Answer & Explanation
Correct Answer: C
Rationale: The presentation of chronic, inflammatory arthritis affecting multiple joints (right knee, previous left ankle) in a child, with elevated inflammatory markers, is highly suggestive of Juvenile Idiopathic Arthritis (JIA). Septic arthritis is typically acute, unilateral, and associated with more severe systemic symptoms. Osteomyelitis is a bone infection. Transient synovitis is usually acute, self-limiting, and primarily affects the hip. Legg-Calvé-Perthes disease affects the hip and is an avascular necrosis, not a generalized inflammatory arthritis.
Question 47
A 6-month-old infant presents with a short, webbed neck, low hairline, and restricted cervical spine motion. Radiographs of the cervical spine show multiple fused cervical vertebrae, including a C2-C3 fusion and a C5-C6 fusion.
View Answer & Explanation
Correct Answer: C
Rationale: The classic triad of a short neck, low posterior hairline, and restricted cervical range of motion, combined with radiographic evidence of fused cervical vertebrae, is diagnostic of Klippel-Feil syndrome. Congenital muscular torticollis involves a sternocleidomastoid contracture. Sprengel's deformity is a congenital elevation of the scapula. Spinal muscular atrophy is a neuromuscular disorder. Neurofibromatosis type 1 can cause spinal deformities but typically not this specific pattern of cervical fusion with the classic triad.
Question 48
A 4-year-old boy with spina bifida (myelomeningocele at L4-L5) presents with progressive bilateral hip dislocation. He has weak quadriceps and absent ankle dorsiflexion. Radiographs confirm bilateral hip dislocations.
View Answer & Explanation
Correct Answer: C
Rationale: Hip dislocations in children with myelomeningocele are often paralytic and require surgical intervention, especially if symptomatic or progressive. Given the age and neurological level, open reduction combined with a varus derotation osteotomy (to address femoral anteversion and valgus) is often necessary to achieve stable reduction and improve function. Observation is inappropriate for symptomatic dislocations. A Pavlik harness is ineffective for paralytic dislocations. Total hip arthroplasty is not indicated in a 4-year-old. Spica cast alone is insufficient to maintain reduction in paralytic dislocations.
Question 49
A 15-year-old female presents with a 6-month history of right knee pain, worse with activity. Physical examination reveals tenderness over the anterior aspect of the proximal tibia, just distal to the patellar tendon insertion. There is no effusion, and range of motion is full. Radiographs show fragmentation and irregularity of the tibial tubercle apophysis.
View Answer & Explanation
Correct Answer: B
Rationale: This is a classic presentation of Osgood-Schlatter disease, an apophysitis of the tibial tubercle, common in active adolescents. The condition is self-limiting and typically resolves with skeletal maturity. Treatment is primarily conservative, focusing on activity modification, rest, ice, and NSAIDs for pain relief. Surgical excision is rarely indicated and only for persistent, painful ossicles after skeletal maturity. Corticosteroid injections are generally contraindicated due to risk of tendon rupture. Patellar tendon repair is for acute ruptures. Total knee arthroplasty is not indicated.
Question 50
A 7-year-old boy presents with a painful limp and swelling over the medial aspect of his left foot. He reports a history of mild foot pain for several months, which has recently worsened. Physical examination reveals tenderness and swelling over the navicular bone. Radiographs show sclerosis, fragmentation, and flattening of the left navicular bone.
View Answer & Explanation
Correct Answer: B
Rationale: This is a classic presentation of Kohler's disease, an avascular necrosis of the navicular bone, common in young children. It is typically self-limiting. Treatment is conservative, focusing on pain relief and protecting the navicular bone during the revascularization phase. This includes activity modification, NSAIDs, and often a walking cast or custom orthotics for support and comfort. Surgical interventions like osteotomy, fusion, or excision are not indicated for Kohler's disease.
Question 51
A 1-year-old infant presents with a congenital deformity of the hand where the thumb and index finger are fused together. The remaining fingers are normal. The parents are concerned about future hand function.
View Answer & Explanation
Correct Answer: C
Rationale: This describes syndactyly, the congenital fusion of digits. Surgical release is the definitive treatment to separate the fingers, improve function, and prevent progressive deformity, especially in the first web space (thumb-index finger) which is critical for grasp. The timing of surgery depends on the severity and specific digits involved, but typically occurs between 6 months and 2 years of age. Observation, casting, or splinting alone will not correct the fusion. Amputation is not indicated.
Question 52
A 28-year-old female presents with a history of recurrent joint dislocations and skin that feels unusually soft and stretches easily. She reports that minor cuts often heal slowly, leaving wide, thin scars. Physical examination reveals generalized joint hypermobility and skin hyperextensibility. Which of the following is the most likely underlying genetic defect?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical presentation of generalized joint hypermobility, skin hyperextensibility, and delayed wound healing with atrophic scars is characteristic of Ehlers-Danlos Syndrome. The provided text explicitly states that Ehlers-Danlos Syndrome is caused by a mutation leading to a nonfunctional COL5A1 allele, resulting in a functionally defective type V collagen protein. FBN1 mutation is associated with Marfan syndrome, lysyl hydroxylase defect with kyphoscoliotic EDS, COL1A1 with osteogenesis imperfecta, and alpha-L-iduronidase deficiency with Hurler syndrome (a mucopolysaccharidosis), none of which are directly stated as the cause of Ehlers-Danlos Syndrome in the provided text.
Question 53
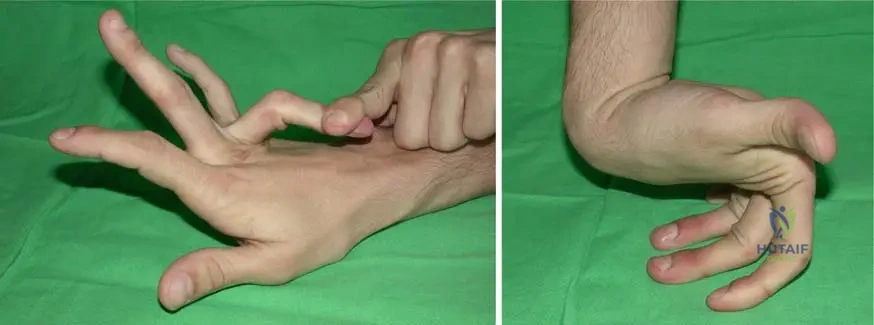
A 15-year-old male presents with a history of easy bruising and skin fragility. On examination, his skin is noted to be remarkably soft and can be stretched significantly beyond normal limits. He also demonstrates excessive range of motion in multiple joints, including his elbows and knees, as shown in the images below. This constellation of findings is most consistent with a disorder primarily affecting which of the following?

View Answer & Explanation
Correct Answer: C
Rationale: The clinical features described (easy bruising, skin fragility, skin hyperextensibility, and generalized joint hypermobility) are hallmarks of Ehlers-Danlos Syndrome. The provided text explicitly states that Ehlers-Danlos Syndrome is a "heritable disorder of connective tissue (collagen fibers and mucopolysaccharides)." Therefore, it primarily affects connective tissue. The images further illustrate the excessive mobility of joints, a key feature of connective tissue laxity.
Question 54
A 4-year-old boy is brought to the clinic due to concerns about his skin. His parents describe his skin as being unusually stretchy and delicate. Physical examination confirms significant skin hyperelasticity, particularly noticeable in his lower extremity and neck region, as depicted in the provided images. This finding is a characteristic manifestation of which condition?
View Answer & Explanation
Correct Answer: C
Rationale: The vignette describes a 4-year-old boy with significant skin hyperelasticity, especially in the lower extremity and neck, which is directly illustrated by the provided images and described in the text as "Fig. 12.7 a, b Skin hyperelasticity of a 4-year-old boy in lower extremity (a) and in the neck region (b)". The text identifies this as a characteristic of Ehlers-Danlos Syndrome. Marfan Syndrome primarily affects the cardiovascular, ocular, and skeletal systems, while Osteogenesis Imperfecta involves bone fragility. Neurofibromatosis Type 1 is characterized by café-au-lait spots and neurofibromas, and Epidermolysis Bullosa by extreme skin fragility leading to blistering, none of which match the described skin hyperelasticity.
Question 55
A 32-year-old female presents with chronic joint pain and a history of multiple joint subluxations. On physical examination, she demonstrates the ability to hyperextend her elbows and knees significantly beyond the normal range, as shown in the images. Her skin is also noted to be soft and velvety. These findings are indicative of a generalized disorder characterized by:
View Answer & Explanation
Correct Answer: B
Rationale: The vignette describes a patient with chronic joint pain, subluxations, and hyperextensible joints, consistent with Ehlers-Danlos Syndrome. The image further illustrates "Excessive mobility of the joints." The text explicitly lists "generalized joint hypermobility" as a characteristic of Ehlers-Danlos Syndrome. The other options are not consistent with the described clinical picture or the known features of Ehlers-Danlos Syndrome.
Question 56
A 22-year-old male with a known diagnosis of Ehlers-Danlos Syndrome undergoes a minor surgical procedure. Postoperatively, the surgeon notes that his wound healing is unusually slow, and the resulting scar is wide and thin. This observation is consistent with which characteristic feature of Ehlers-Danlos Syndrome?
View Answer & Explanation
Correct Answer: C
Rationale: The provided text explicitly states that Ehlers-Danlos Syndrome is characterized by "delayed wound healing with formation of atrophic scars." The clinical scenario directly reflects this characteristic. The other options describe processes that are either opposite to what is observed in EDS or are not mentioned as features of the syndrome in the provided text.
Question 57
A 45-year-old female with a long-standing history of generalized joint hypermobility and skin hyperextensibility presents for a routine physical. During her workup, an echocardiogram reveals heart dilatation and she is found to have pulmonary hypertension. These findings represent which category of extraskeletal manifestations associated with her condition?
View Answer & Explanation
Correct Answer: D
Rationale: The vignette describes a patient with classic features of Ehlers-Danlos Syndrome who also presents with heart dilatation and pulmonary hypertension. The provided text explicitly lists "respiratory and cardiac complications due to pulmonary hypertension, heart dilatation, and particular aortic dissection" as extraskeletal manifestations of Ehlers-Danlos Syndrome. Therefore, these findings fall under respiratory and cardiac complications.
Question 58
A 10-year-old boy with Ehlers-Danlos Syndrome is undergoing a comprehensive evaluation. His parents report concerns about his balance and coordination, and he has recently been diagnosed with sensorineural deafness. These neurological findings are consistent with which of the following extraskeletal manifestations of Ehlers-Danlos Syndrome?
View Answer & Explanation
Correct Answer: C
Rationale: The vignette describes a patient with Ehlers-Danlos Syndrome experiencing sensorineural deafness and issues with balance and coordination (suggesting cerebellar ataxia). The provided text explicitly lists "Neurologic complications are sensorineural deafness, chorea and cerebellar ataxia, and percussion myotonia." This directly matches the described findings. The other options are not listed as specific neurological complications of Ehlers-Danlos Syndrome in the provided text.
Question 59
A 50-year-old male with a history of recurrent joint dislocations and skin fragility is being evaluated for worsening shortness of breath. Pulmonary function tests reveal evidence of pulmonary hypertension. This respiratory complication is a known extraskeletal manifestation of Ehlers-Danlos Syndrome, which is primarily a disorder of:
View Answer & Explanation
Correct Answer: B
Rationale: The vignette describes a patient with classic features of Ehlers-Danlos Syndrome (joint dislocations, skin fragility) and a respiratory complication (pulmonary hypertension). The text states that Ehlers-Danlos Syndrome is a "heritable disorder of connective tissue (collagen fibers and mucopolysaccharides)." Therefore, the underlying pathology leading to these diverse manifestations, including respiratory complications, is a defect in connective tissue.
Question 60
A 7-year-old girl presents with generalized joint hypermobility and skin that is easily bruised and tears. Her parents report that she has always had very soft skin. Genetic testing is performed, and the results confirm a diagnosis of Ehlers-Danlos Syndrome. The primary collagen type affected by the mutation described in this condition is:
View Answer & Explanation
Correct Answer: E
Rationale: The provided text explicitly states that Ehlers-Danlos Syndrome is caused by a mutation leading to a nonfunctional COL5A1 allele, "resulting in a functionally defective type V collagen protein." Therefore, Type V collagen is the primary collagen type affected as described in this specific context.
Question 61
A 25-year-old pregnant woman with Ehlers-Danlos Syndrome is being counseled regarding potential complications. She expresses concern about her skin's fragility and tendency to bruise easily, even from minor trauma. This characteristic is directly related to the underlying defect in:
View Answer & Explanation
Correct Answer: C
Rationale: The vignette highlights "fragile and soft skin" and "easy bruising" as features of Ehlers-Danlos Syndrome. The text defines EDS as a "heritable disorder of connective tissue (collagen fibers and mucopolysaccharides)." These skin manifestations are a direct consequence of the compromised integrity of the connective tissue, particularly collagen, which provides structural support to the skin and blood vessels. While bruising can involve coagulation, the primary defect in EDS leading to easy bruising and skin fragility is the structural weakness of the connective tissue itself, not a primary hematological disorder.
Question 62
A family presents with several members diagnosed with Ehlers-Danlos Syndrome. While some individuals exhibit severe joint hypermobility and significant skin involvement, others in the same family show milder symptoms, primarily limited to easy bruising. This observation highlights which aspect of Ehlers-Danlos Syndrome?
View Answer & Explanation
Correct Answer: C
Rationale: The vignette describes varying severity of symptoms within the same family, which is known as intrafamilial variability, and also implies variability between families (interfamilial). The provided text explicitly states, "Inter- and intrafamilial phenotypic variability is observed, but no genotype–phenotype correlations have been made so far." This directly supports option C. The text also states it is a "heritable disorder," not necessarily spontaneous mutation in all, and does not specify an X-linked pattern. The lack of uniform expression contradicts complete penetrance with uniform expression.
Question 63
A 60-year-old male with a history of Ehlers-Danlos Syndrome presents to the emergency department with acute chest pain and shortness of breath. Imaging reveals an aortic dissection. This severe cardiovascular event is a known complication of Ehlers-Danlos Syndrome due to the underlying defect in:
View Answer & Explanation
Correct Answer: C
Rationale: The vignette describes a patient with Ehlers-Danlos Syndrome experiencing aortic dissection. The provided text lists "aortic dissection" as a cardiac complication. Since EDS is a "heritable disorder of connective tissue," the fragility of the aortic wall, which is rich in connective tissue, makes it susceptible to dissection. Therefore, the underlying defect in vascular connective tissue integrity is the primary cause.
Question 64
A 30-year-old female with Ehlers-Danlos Syndrome is being evaluated for chronic pain. Her physical exam reveals widespread joint hypermobility and skin hyperextensibility. The fundamental components of connective tissue primarily affected in this syndrome, as described in the provided text, are:
View Answer & Explanation
Correct Answer: B
Rationale: The provided text explicitly states that Ehlers-Danlos Syndrome is a "heritable disorder of connective tissue (collagen fibers and mucopolysaccharides)." This directly identifies the fundamental components primarily affected. While other components are part of connective tissue, the text specifically highlights collagen fibers and mucopolysaccharides in the context of EDS.
Question 65
A 19-year-old male with a family history of Ehlers-Danlos Syndrome presents with generalized joint hypermobility and skin that is easily bruised. He is concerned about potential long-term complications. Which of the following neurological findings is specifically mentioned as a complication of Ehlers-Danlos Syndrome in the provided text?
View Answer & Explanation
Correct Answer: C
Rationale: The vignette describes a patient with features of Ehlers-Danlos Syndrome. The provided text explicitly lists "Neurologic complications are sensorineural deafness, chorea and cerebellar ataxia, and percussion myotonia." Chorea is directly mentioned as a neurological complication. The other options are not listed in the provided text as neurological complications of Ehlers-Danlos Syndrome.
Question 66
A 40-year-old female with Ehlers-Danlos Syndrome is being evaluated for persistent muscle stiffness and delayed relaxation after muscle contraction. On examination, percussion of her muscles elicits a sustained contraction. This specific neurological finding is known as:
View Answer & Explanation
Correct Answer: D
Rationale: The vignette describes a patient with Ehlers-Danlos Syndrome exhibiting muscle stiffness and delayed relaxation, with percussion eliciting sustained contraction. The provided text explicitly lists "percussion myotonia" as a neurological complication of Ehlers-Danlos Syndrome. This term precisely describes the clinical finding.
Question 67
A 2-year-old child is suspected of having Ehlers-Danlos Syndrome due to extreme joint laxity and very soft skin. The parents inquire about the predictability of the disease course. Based on the provided information, which statement regarding genotype-phenotype correlation in Ehlers-Danlos Syndrome is most accurate?
View Answer & Explanation
Correct Answer: C
Rationale: The provided text explicitly states, "Inter- and intrafamilial phenotypic variability is observed, but no genotype–phenotype correlations have been made so far." This directly supports option C, indicating that the genetic mutation does not reliably predict the specific clinical manifestations or severity in EDS. The other options contradict this statement.
Question 68
A 35-year-old male presents with a history of recurrent shoulder dislocations and chronic knee pain. On examination, he demonstrates the ability to touch his thumb to his forearm and hyperextend his metacarpophalangeal joints beyond 90 degrees. His skin is noted to be unusually soft and easily stretched. These findings are consistent with a disorder primarily affecting the structural integrity of:
View Answer & Explanation
Correct Answer: C
Rationale: The vignette describes classic signs of Ehlers-Danlos Syndrome: recurrent joint dislocations, chronic joint pain, generalized joint hypermobility (as demonstrated by specific maneuvers), and soft, stretchy skin. The provided text defines EDS as a "heritable disorder of connective tissue (collagen fibers and mucopolysaccharides)." Therefore, the structural integrity of collagen and mucopolysaccharides is primarily affected.
Question 69
A 55-year-old female with Ehlers-Danlos Syndrome is being evaluated for a planned elective surgery. Given her diagnosis, the surgical team should be particularly aware of which of the following intraoperative and postoperative challenges?
View Answer & Explanation
Correct Answer: C
Rationale: The provided text characterizes Ehlers-Danlos Syndrome by "fragile and soft skin, delayed wound healing with formation of atrophic scars, and easy bruising." These features directly translate into significant surgical challenges, including tissue fragility during dissection, compromised wound closure, and increased risk of hematoma formation. The other options are not specifically mentioned as direct surgical challenges related to the core pathology of EDS in the provided text.
Question 70
A 29-year-old male presents with a history of recurrent joint dislocations and skin hyperextensibility. His mother and maternal grandmother have similar symptoms. This familial pattern of inheritance is consistent with Ehlers-Danlos Syndrome, which is described as a:
View Answer & Explanation
Correct Answer: C
Rationale: The vignette describes a familial pattern of symptoms consistent with Ehlers-Danlos Syndrome. The provided text explicitly states, "Th is syndrome is a heritable disorder of connective tissue (collagen fi bers and mucopolysaccharides)." This directly supports the classification of EDS as a heritable disorder. The other options are incorrect classifications based on the provided text.
Question 71
A 4-year-old boy is being evaluated for generalized joint hypermobility and skin hyperelasticity, as depicted in the clinical images. His parents also report that he bruises very easily. These findings are characteristic of Ehlers-Danlos Syndrome. Which of the following is NOT listed as an extraskeletal manifestation of this syndrome in the provided text?
View Answer & Explanation
Correct Answer: E
Rationale: The vignette describes a child with classic features of Ehlers-Danlos Syndrome, consistent with the provided images. The question asks which option is NOT an extraskeletal manifestation listed in the text. The text explicitly lists "respiratory and cardiac complications due to pulmonary hypertension, heart dilatation, and particular aortic dissection" and "Neurologic complications are sensorineural deafness, chorea and cerebellar ataxia, and percussion myotonia." Renal cysts are not mentioned anywhere in the provided text as an extraskeletal manifestation of Ehlers-Danlos Syndrome.
Question 72
A 28-year-old female presents with chronic joint pain and a history of recurrent shoulder dislocations. On physical examination, she demonstrates the ability to touch her thumb to her forearm, hyperextend her elbows and knees beyond 10 degrees, and easily place her palms flat on the floor with knees extended. Her skin is noted to be soft and velvety. Which of the following is the most likely underlying genetic defect?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical presentation of generalized joint hypermobility, soft skin, and recurrent dislocations is highly suggestive of Ehlers-Danlos Syndrome (EDS). The provided text explicitly states that Ehlers-Danlos Syndrome is caused by "a mutation, leading to a nonfunctional COL5A1 allele, and resulting in a functionally defective type V collagen protein." Option A (FBN1 mutation) is associated with Marfan Syndrome. Option C (lysyl hydroxylase defect) is associated with Kyphoscoliotic EDS. Option D (COL1A1 mutation) is associated with Osteogenesis Imperfecta. Option E (alpha-L-iduronidase deficiency) is associated with Hurler Syndrome (MPS I).
Question 73
A 15-year-old male is evaluated for easy bruising and skin fragility. His mother reports that he has always had very "stretchy" skin and that his wounds heal slowly, often leaving wide, thin scars. Physical examination confirms skin hyperextensibility and atrophic scars. Which of the following connective tissue components is primarily affected in this condition?
View Answer & Explanation
Correct Answer: C
Rationale: The case describes classic features of Ehlers-Danlos Syndrome (EDS), including skin hyperextensibility, fragility, easy bruising, and atrophic scars. The provided text states, "This syndrome is a heritable disorder of connective tissue (collagen fibers and mucopolysaccharides)." While other components like elastin and proteoglycans are part of connective tissue, the primary defect in EDS, as described, involves collagen fibers and mucopolysaccharides. Fibrillin-1 is primarily associated with Marfan syndrome.
Question 74
A 35-year-old male with a known diagnosis of Ehlers-Danlos Syndrome presents to the emergency department with acute chest pain radiating to his back. His blood pressure is 180/100 mmHg, and he appears distressed. Given his underlying condition, which of the following cardiac complications is he at highest risk for?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical vignette describes a patient with EDS presenting with acute chest and back pain, which is highly concerning for an acute aortic event. The provided text explicitly lists "aortic dissection" as a known extraskeletal manifestation of Ehlers-Danlos Syndrome, alongside pulmonary hypertension and heart dilatation. While mitral valve prolapse can be seen in EDS, aortic dissection represents a more acute and life-threatening complication consistent with the presentation. Atrial fibrillation, pericarditis, and myocardial infarction are less directly linked to the specific connective tissue defect of EDS as primary complications.
Question 75
A 7-year-old boy with Ehlers-Danlos Syndrome is noted by his parents to have difficulty hearing and occasionally stumbles when walking. On examination, he exhibits some uncoordinated movements. Which of the following neurologic complications is consistent with his presentation?
View Answer & Explanation
Correct Answer: C
Rationale: The provided text lists "sensorineural deafness, chorea and cerebellar ataxia, and percussion myotonia" as neurologic complications of Ehlers-Danlos Syndrome. The boy's symptoms of difficulty hearing and stumbling/uncoordinated movements directly align with sensorineural deafness and cerebellar ataxia. The other options are not specifically mentioned as neurologic complications of EDS in the provided text.
Question 76
A 4-year-old boy is brought to the clinic due to concerns about his skin. His parents describe his skin as unusually soft and easily bruised. On physical examination, the physician demonstrates the ability to stretch the skin on his forearm significantly before it recoils slowly. This finding is most accurately described as:
View Answer & Explanation
Correct Answer: C
Rationale: The clinical vignette describes a classic skin manifestation of Ehlers-Danlos Syndrome: the ability to stretch the skin significantly. The provided text explicitly characterizes EDS by "skin hyperextensibility." While skin atrophy (B) can be seen in the form of atrophic scars, the primary finding described is the stretchiness. Cutis laxa (A) is a different connective tissue disorder characterized by loose, inelastic skin that hangs in folds. Dermatitis (D) and Psoriasis (E) are inflammatory skin conditions unrelated to the described findings.
Question 77
A 10-year-old girl presents with a history of multiple joint sprains and dislocations, particularly in her knees and shoulders. On examination, she can hyperextend her metacarpophalangeal joints beyond 90 degrees and passively dorsiflex her wrist to touch her forearm. These findings are indicative of:
View Answer & Explanation
Correct Answer: C
Rationale: The clinical vignette describes a child with excessive range of motion in multiple joints, leading to sprains and dislocations. This is the hallmark of "generalized joint hypermobility," which the provided text lists as a key characteristic of Ehlers-Danlos Syndrome. Localized joint laxity (A) would imply only one or a few joints are affected, not multiple as described. Joint contractures (B) are the opposite of hypermobility. Muscular hypotonia (D) can contribute to joint instability but is not the primary descriptor of the joint findings themselves. Osteoarthritis (E) is a degenerative condition, often a long-term consequence of hypermobility, but not the primary finding.
Question 78
A 22-year-old female with Ehlers-Danlos Syndrome undergoes a minor surgical procedure. Post-operatively, her wound healing is slower than expected, and the resulting scar appears wide and thin. This characteristic wound healing is described in the context of EDS as:
View Answer & Explanation
Correct Answer: C
Rationale: The provided text explicitly states that Ehlers-Danlos Syndrome is characterized by "delayed wound healing with formation of atrophic scars." The description of slower healing and wide, thin scars perfectly matches this characteristic. Keloid formation (A) and hypertrophic scarring (B) involve excessive collagen deposition, which is not typical for EDS. Normal (D) or rapid (E) wound healing are contrary to the known features of EDS.
Question 79
A 6-year-old boy is diagnosed with Ehlers-Danlos Syndrome based on clinical findings of joint hypermobility, skin hyperextensibility, and easy bruising. His parents inquire about the predictability of his future symptoms compared to other family members who also have EDS. What does the current understanding of genotype-phenotype correlation in EDS suggest?
View Answer & Explanation
Correct Answer: C
Rationale: The provided text directly addresses this point, stating, "Inter- and intrafamilial phenotypic variability is observed, but no genotype–phenotype correlations have been made so far." This means that even within the same family or with the same genetic mutation, the clinical presentation can vary significantly, and genetic testing cannot currently predict the exact spectrum or severity of symptoms. Options A, B, D, and E contradict this statement.
Question 80
A 45-year-old female with Ehlers-Danlos Syndrome presents with chronic, widespread musculoskeletal pain. She has a history of multiple joint subluxations and dislocations. Given the underlying connective tissue disorder, what is a common long-term orthopedic complication she is at increased risk for?
View Answer & Explanation
Correct Answer: C
Rationale: While not explicitly stated in the provided text, the generalized joint hypermobility and recurrent instability (subluxations/dislocations) characteristic of EDS lead to abnormal joint mechanics and increased wear and tear on articular cartilage over time. This predisposes individuals with EDS to early-onset osteoarthritis. This is a well-established orthopedic consequence of chronic joint instability in connective tissue disorders. The provided text emphasizes "excessive mobility of the joints," which is the direct precursor to this complication. Osteoporosis (A), avascular necrosis (B), bone tumors (D), and septic arthritis (E) are not directly linked as primary long-term complications of EDS in the same manner as osteoarthritis.
Question 81
A 30-year-old male with Ehlers-Danlos Syndrome is scheduled for an elective knee arthroscopy to address recurrent patellar subluxations. During the surgical planning, the orthopedic surgeon must consider the unique tissue properties associated with EDS. Which of the following is a critical surgical consideration?
View Answer & Explanation
Correct Answer: C
Rationale: Ehlers-Danlos Syndrome is characterized by "fragile and soft skin" and a defect in collagen, which extends to other connective tissues. This fragility means that tissues, including skin, fascia, and joint capsules, are weaker and may not hold sutures well, increasing the risk of wound dehiscence and surgical complications. The text mentions "fragile and soft skin" and "delayed wound healing," which are direct indicators of compromised tissue integrity. Options A, B, D, and E are incorrect; bone healing is not enhanced, tissue strength is compromised, and there is no reduced risk of infection or increased risk of heterotopic ossification specifically mentioned or implied by the core pathology.
Question 82
A 5-year-old boy presents with hypermobile joints and skin that is easily stretched. His parents report that he frequently bruises with minimal trauma. These findings are characteristic of a disorder primarily affecting:
View Answer & Explanation
Correct Answer: C
Rationale: The clinical vignette describes classic symptoms of Ehlers-Danlos Syndrome: hypermobile joints, skin hyperextensibility, and easy bruising. The provided text defines EDS as "a heritable disorder of connective tissue (collagen fibers and mucopolysaccharides)." Therefore, the disorder primarily affects connective tissue. Bone mineralization (A) is related to conditions like osteogenesis imperfecta or rickets. Muscle contractility (B) relates to muscular dystrophies. Nerve conduction (D) relates to neuropathies. Hematopoiesis (E) relates to blood disorders.
Question 83
A 19-year-old female with Ehlers-Danlos Syndrome is being counseled on lifestyle modifications. Given her generalized joint hypermobility, which of the following activities should she most likely be advised to avoid or approach with caution?
View Answer & Explanation
Correct Answer: C
Rationale: The core orthopedic manifestation of EDS is "generalized joint hypermobility," leading to instability and recurrent dislocations/subluxations. High-impact contact sports significantly increase the risk of joint injury, dislocation, and exacerbation of pain due to the inherent laxity of the joints. Low-impact exercises, physical therapy for stabilization, walking, cycling, and strength training with light weights are generally recommended to strengthen supporting musculature and improve proprioception, thereby protecting the joints. Therefore, avoiding high-impact contact sports is a crucial recommendation.
Question 84
A 50-year-old male with a long-standing history of Ehlers-Danlos Syndrome presents with increasing shortness of breath and fatigue. Echocardiography reveals an enlarged heart and elevated pulmonary artery pressures. These findings are consistent with which extraskeletal manifestation of EDS?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical vignette describes cardiac and respiratory symptoms (shortness of breath, fatigue, enlarged heart, elevated pulmonary artery pressures). The provided text explicitly lists "respiratory and cardiac complications due to pulmonary hypertension, heart dilatation, and particular aortic dissection" as extraskeletal manifestations of EDS. Therefore, pulmonary hypertension and heart dilatation are consistent with the patient's presentation. The other options are not listed as specific extraskeletal manifestations in the provided text.
Question 85
A 2-year-old girl is brought to the pediatrician due to concerns about her skin. Her mother notes that the skin on her neck and extremities is unusually stretchy. The pediatrician gently pulls the skin on her neck, observing significant elasticity. This finding, along with generalized joint hypermobility, suggests a defect in:
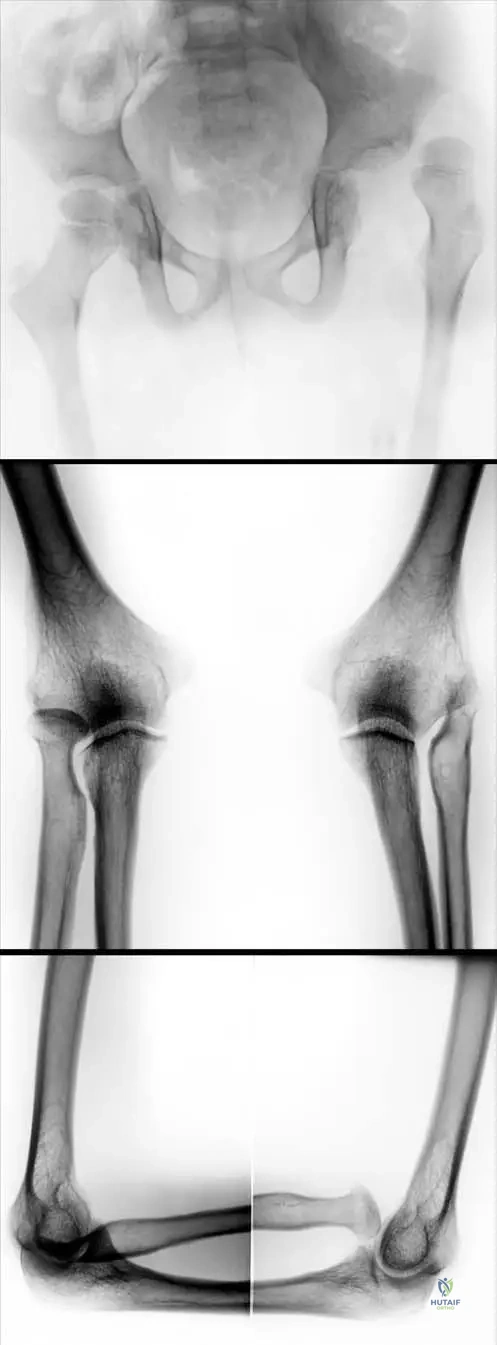
View Answer & Explanation
Correct Answer: C
Rationale: The clinical vignette describes classic features of Ehlers-Danlos Syndrome (EDS), specifically skin hyperextensibility and generalized joint hypermobility. The provided text states that EDS is "caused by a mutation, leading to a nonfunctional COL5A1 allele, and resulting in a functionally defective type V collagen protein." Therefore, the underlying defect is in type V collagen protein function. While elastin (D) contributes to skin elasticity, the primary genetic defect described for EDS in the text is related to collagen. Keratin (A) is a structural protein in skin, hair, and nails. Melanin (B) is involved in pigmentation. Hyaluronic acid (E) is a component of the extracellular matrix but not the primary defect described here.
Question 86
A 25-year-old female with Ehlers-Danlos Syndrome reports experiencing muscle cramps and stiffness, particularly after repetitive movements. On examination, a physician notes a sustained contraction of muscle after a tap with a reflex hammer. This specific neurologic finding is known as:
View Answer & Explanation
Correct Answer: C
Rationale: The clinical vignette describes a specific neurologic phenomenon where muscle contraction is sustained after a percussion stimulus. The provided text explicitly lists "percussion myotonia" as one of the neurologic complications of Ehlers-Danlos Syndrome. Fasciculations (A) are small, involuntary muscle twitches. Myoclonus (B) refers to sudden, brief, involuntary jerking or twitching of a muscle or group of muscles. Dystonia (D) is a movement disorder causing involuntary muscle contractions. Tremor (E) is an involuntary, rhythmic muscle contraction leading to shaking movements.
Question 87
A 14-year-old boy presents with a history of recurrent ankle sprains and knee pain. Physical examination reveals significant hyperextension of his knees and elbows, and he can easily touch his palms to the floor. His skin is soft and shows several wide, thin scars from minor childhood injuries. Based on these findings, what is the most appropriate initial diagnostic approach?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical vignette presents a classic picture of Ehlers-Danlos Syndrome (EDS) with generalized joint hypermobility, soft skin, and atrophic scars. Diagnosis of EDS, particularly the hypermobile type (which is often associated with the COL5A1 defect mentioned in the text, though the text does not specify types), is primarily clinical, based on established criteria (e.g., the Beighton score for hypermobility and other major/minor criteria). While genetic testing can confirm specific types of EDS, the initial approach is clinical. Genetic sequencing for COL1A1 (A) is for Osteogenesis Imperfecta. Serum creatine kinase (B) and EMG (D) are for muscle disorders. Bone mineral density scan (E) is for osteoporosis. The text describes the clinical features, implying a clinical diagnostic pathway.
Question 88
A 3-year-old girl with Ehlers-Danlos Syndrome is being monitored for potential complications. Her parents are concerned about her heart health. Which of the following cardiac findings, if present, would be considered a direct extraskeletal manifestation of her condition as described in the provided text?
View Answer & Explanation
Correct Answer: C
Rationale: The provided text explicitly lists "heart dilatation" as a respiratory and cardiac complication of Ehlers-Danlos Syndrome. While other cardiac anomalies can occur in the general population or in other syndromes, heart dilatation is specifically mentioned as an extraskeletal manifestation of EDS in the given context. The other options are congenital heart defects not specifically listed as direct manifestations of EDS in the provided text.
Question 89
A 29-year-old pregnant woman with Ehlers-Danlos Syndrome is being managed by a multidisciplinary team. Given the nature of her connective tissue disorder, what is a significant obstetric concern related to tissue fragility?
View Answer & Explanation
Correct Answer: C
Rationale: Although not explicitly detailed in the provided text, the core characteristics of EDS include "fragile and soft skin" and a generalized defect in connective tissue. This fragility extends to other tissues, including the uterus and perineum. Therefore, individuals with EDS are at an increased risk of complications such as uterine rupture, cervical insufficiency, and severe perineal tears during childbirth due to the inherent weakness of these tissues. This is a well-known obstetric complication stemming directly from the described tissue fragility. The other options are not directly linked to the connective tissue defect of EDS.
Question 90
A 16-year-old female with Ehlers-Danlos Syndrome is undergoing evaluation for chronic knee pain and instability. Her physical exam demonstrates significant patellar hypermobility. Which of the following is the most appropriate initial non-surgical management strategy?
View Answer & Explanation
Correct Answer: C
Rationale: The primary orthopedic issue in EDS is "generalized joint hypermobility," leading to instability. For chronic knee pain and patellar hypermobility, the initial non-surgical management focuses on improving dynamic stability. Strengthening the muscles surrounding the joint, particularly the quadriceps (VMO) and core muscles, helps to compensate for the lax ligaments and capsule. Immobilization (A) and bed rest (B) would lead to muscle atrophy and worsen instability. Corticosteroid injections (D) are for inflammation, not primary instability. Immediate surgical stabilization (E) is typically reserved for failed conservative management or severe, recurrent dislocations, and even then, surgical outcomes can be challenging due to tissue fragility.
Question 91
A 42-year-old female presents with a 9-month history of painful, swollen fingers and toes. She also notes persistent, scaly red patches on her scalp and elbows. Physical examination reveals well-demarcated erythematous plaques with silvery scales on the extensor surfaces of her limbs and scalp. Multiple distal interphalangeal (DIP) joints are swollen and tender. Laboratory tests are negative for rheumatoid factor and anti-CCP antibodies. Which of the following best describes the classification of this patient's likely diagnosis?

View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "Psoriatic arthritis is one form of seronegative spondylarthritis (SNSA)." The patient's presentation with psoriatic skin lesions, DIP joint involvement, and seronegativity aligns with this classification. Option A is incorrect as psoriatic arthritis is seronegative. Option D is incorrect as the presentation is inflammatory, not degenerative.
Question 92
A 38-year-old male presents with a 3-month history of pain and stiffness in his lower back, particularly in the mornings. He also reports swelling and pain in his right great toe. On examination, he has well-demarcated erythematous plaques with silvery scales on his elbows and gluteal cleft. Radiographs of the pelvis show evidence of sacroiliitis. Laboratory tests reveal negative rheumatoid factor. Which of the following is the most commonly involved joint type in the peripheral arthritis component of this condition?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that "Polyarthritis is erosive, destructive, and involves most commonly the DIP joints." This makes DIP joints the most characteristic peripheral joint involvement. Options A and B are more typical of rheumatoid arthritis, which is seropositive.
Question 93
A 50-year-old male presents with a 2-year history of chronic low back pain and stiffness, worse in the morning and improving with activity. He has a long-standing history of psoriasis affecting his scalp and nails. Physical examination reveals limited spinal mobility and tenderness over the sacroiliac joints. His fingernails show pitting and onycholysis. Laboratory tests are negative for rheumatoid factor. Given the patient's presentation, what percentage of individuals with psoriasis vulgaris typically develop joint involvement?
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "Incidence of psoriasis vulgaris is 0.5–2%; out of this population 5–10% suff er joint involvement." This directly answers the question regarding the proportion of psoriasis patients who develop arthritis. Options A, C, D, and E are incorrect based on the provided incidence data.
Question 94
A 35-year-old female presents with a 6-month history of painful, swollen fingers and toes, along with diffuse swelling of her right middle finger, giving it a "sausage-like" appearance. She has a known history of psoriasis. Radiographs show erosive changes in the DIP joints and periostitis. Which of the following terms best describes the "sausage-like" swelling observed in her finger?

View Answer & Explanation
Correct Answer: C
Rationale: The text mentions, "Destructive arthritis of distal joints may be manifest in so-called sausage fi ngers." This "sausage finger" appearance is clinically known as dactylitis, which is a characteristic feature of psoriatic arthritis. Synovitis and tenosynovitis are components but dactylitis describes the overall appearance. Cellulitis is an infection and bursitis is inflammation of a bursa.
Question 95
A 48-year-old male presents with new onset arthritis affecting his hands and feet. He denies any prior skin rashes. On examination, he has swollen and tender DIP joints, and some nail pitting is noted. Laboratory tests are negative for rheumatoid factor. He is concerned about the diagnosis given the absence of skin lesions. Which of the following statements regarding the relationship between skin and joint manifestations in psoriatic arthritis is most accurate?
View Answer & Explanation
Correct Answer: D
Rationale: The text states, "Th e skin changes usually precede the joint manifestations, but can happen vice-versa ('arthritis psoriatica sine psoriasis')." This directly supports option D. Options A, B, C, and E are incorrect as they contradict the possibility of joint manifestations preceding skin changes.
Question 96
A 30-year-old female presents with a 4-month history of pain and swelling in her hands and feet. She has a family history of psoriasis. On examination, she has erythematous plaques with silvery scales on her scalp and elbows. Multiple DIP joints are swollen and tender. Radiographs show erosive changes. What is the typical age range for the appearance of psoriatic arthritis?
View Answer & Explanation
Correct Answer: C
Rationale: The text specifies, "Th e disease appears between 30 and 50 years of age." This makes option C the correct answer. The other age ranges are not consistent with the provided information.
Question 97
A 40-year-old male presents with chronic pain at the insertion of his Achilles tendon and on the plantar surface of his heel. He also has a history of psoriasis affecting his nails and scalp. Physical examination reveals tenderness at the Achilles tendon insertion and plantar fascia origin. Laboratory tests are negative for rheumatoid factor. This type of inflammatory process at tendon and ligament insertions is characteristic of psoriatic arthritis and is known as:
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Enthesopathia is common, presenting usually on the plantar surface of the heel and at the attachment of Achilles tendon." This directly defines the condition described in the vignette. Tendinitis is a more general term for tendon inflammation, but enthesopathy specifically refers to inflammation at the insertion site. Bursitis, synovitis, and osteoarthritis describe different pathological processes.
Question 98
A 45-year-old female with a known history of psoriasis presents with a 6-month history of progressive stiffness and pain in her spine, particularly in the lumbar and cervical regions. Radiographs show syndesmophytes and sacroiliitis. Her peripheral joints are largely unaffected. Which of the following laboratory markers is most likely to be positive in this specific presentation of psoriatic arthritis?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "HLAB27 antigen is positive only on cases of spinal spread." Given the patient's spinal involvement (stiffness, pain, syndesmophytes, sacroiliitis), HLA-B27 positivity is expected. RF and anti-CCP are typically negative in psoriatic arthritis. ANA is not specifically mentioned as a diagnostic marker for spinal psoriatic arthritis. CRP is a general inflammatory marker, not specific for spinal involvement.
Question 99
A 33-year-old female presents with a 1-year history of painful, swollen joints in her hands and feet. She has a history of psoriasis since adolescence. On examination, she has well-demarcated erythematous papules and plaques with silver-gray lamellae on her scalp and extensor surfaces. Her DIP joints show significant swelling and tenderness. Radiographs reveal erosive changes and periostitis. Which of the following best describes the typical nature of the polyarthritis in psoriatic arthritis?
View Answer & Explanation
Correct Answer: C
Rationale: The text clearly states, "Polyarthritis is erosive, destructive, and involves most commonly the DIP joints." This directly supports option C. Options A, B, D, and E contradict this description of the joint pathology in psoriatic arthritis.
Question 100
A 40-year-old male presents with a 6-month history of joint pain and swelling. He has a long-standing history of psoriasis. On examination, he has typical psoriatic skin lesions on his elbows and scalp. His DIP joints are swollen and tender, and he has dactylitis of his left index finger. Laboratory tests show negative rheumatoid factor. Which of the following is a characteristic feature of the skin lesions seen in this patient?
View Answer & Explanation
Correct Answer: B
Rationale: The image description and clinical context state, "Typical psoriatic skin lesions... Well-defi ned erythematosus papulae and plaques covered with silver–gray lamellae." This directly matches option B. The other options describe different types of skin lesions not characteristic of psoriasis.
